Category: GRDS
Three Different Problems: Gastritis, Gastroesophageal Reflux, and Bile reflux Gastritis
June 05, 2025 4:52 am
Gastritis is a general term used for the description of symptoms associated with several very different physical conditions and require different treatments based on their ideology . Gastritis, gastroesophageal reflux, and bile reflux gastritis
Gastritis may be caused by excess acid or bile in the stomach. Some patients may have gastroesophageal reflux due to a hiatal hernia, which needs to be treated surgically with Nissen fundoplication, regardless of the size of the hernia, contrary to what gastroenterologists recommend by prescribing antacids for an extended period. I have seen patients who have had one cm hiatal hernia and have been very symptomatic, and others who have had larger hiatal hernias and have been asymptomatic. Size should not be a determinant of whether the patient has had or will have a hernia repair or not.
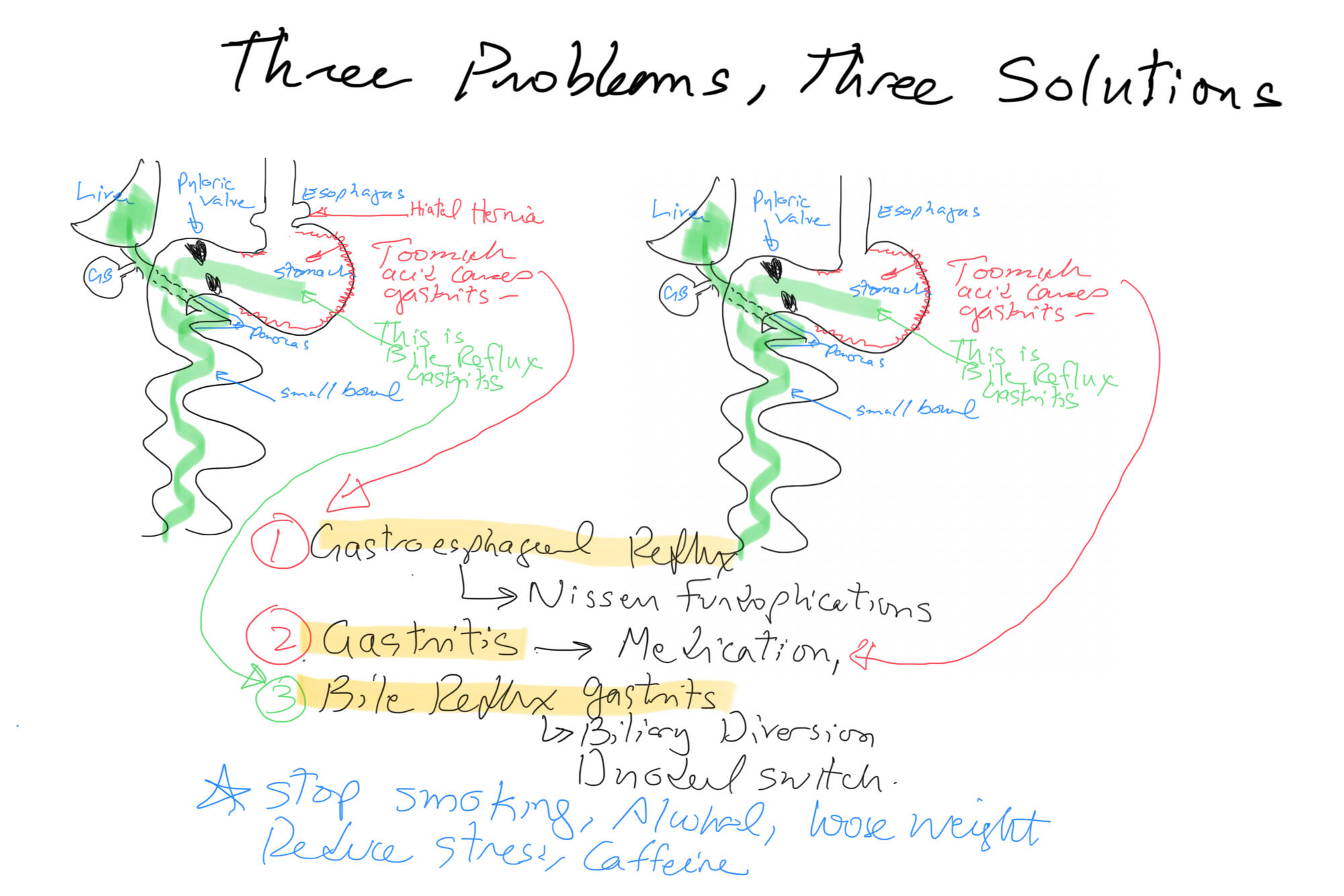
Billiary Diversion is the definitive surgical procedure for Bile Reflux Gastritis.
How does a stapler staple and cut at the same time
February 11, 2025 12:27 pm
The gastrointestinal staplers simultaneously pass six rows of staples and cut in between them to create two secure lines of staples, three rows on each side. The staples come in different thicknesses and lengths for various applications. Staple cartridges that are used for colon surgery are usually thicker tissue staples than those that are used for small bowel stapling.
Different manufacturers have different color coding.

Another question I frequently get asked is, How does a stapler staple and cut at the same time? The stapler needs to be thick enough to not tear through the tissue and provide uniform pressure for control of bleeding and prevent leaks. It can not be too large either.
When stapling on the stomach for sleeve gastrectomy, the stomach wall thickness is different. We use different-sized staples to accommodate the thicker part of the lower stomach toward the thinner part of the stomach where it meets the esophagus.


Video of stapler demonstration
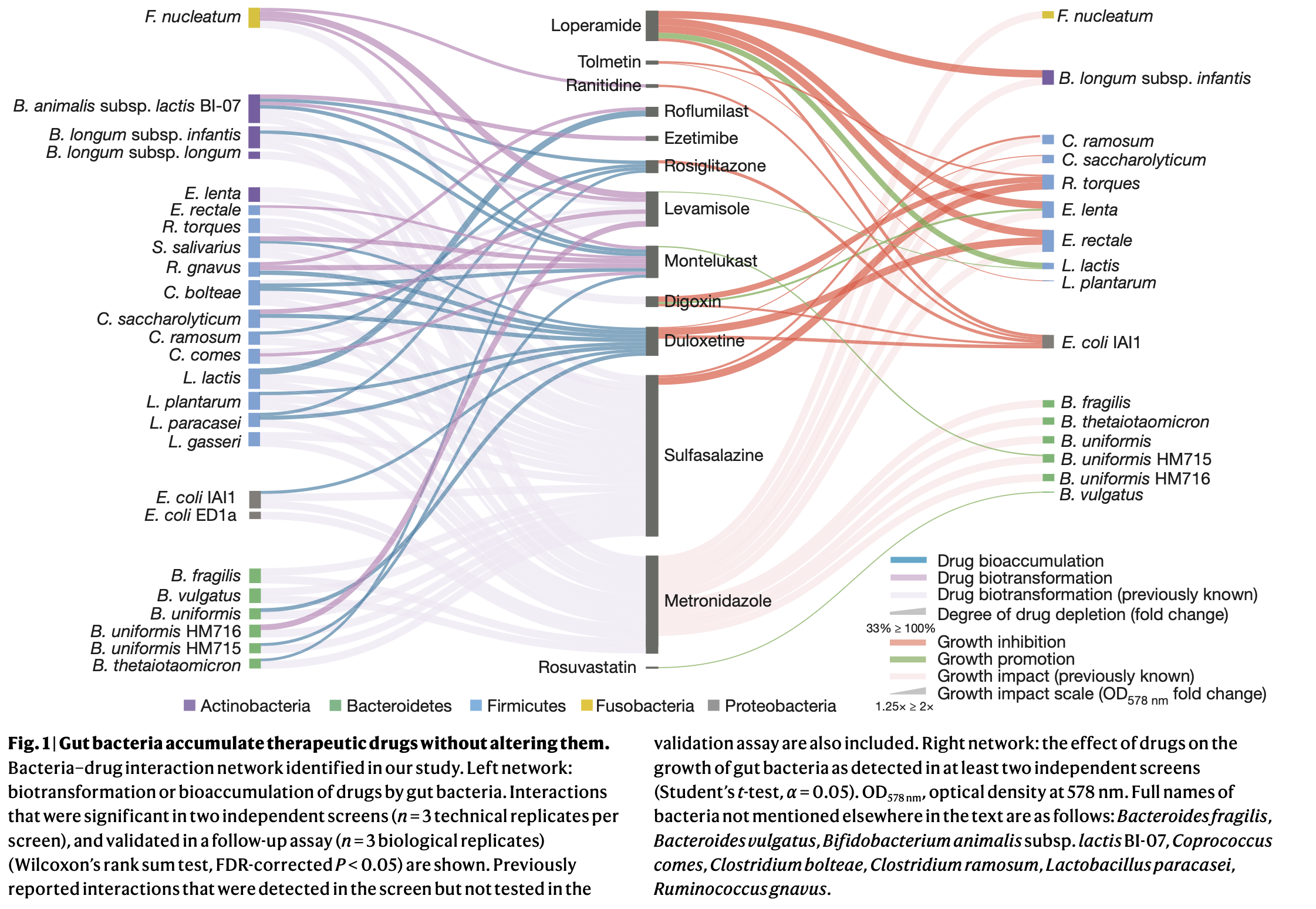
Medication Accumulation in Gut Bacteria May Curb Drug Effectiveness, Alter Gut Microbiome
October 05, 2021 2:06 pm
COVID Vaccines
March 05, 2021 3:50 pm
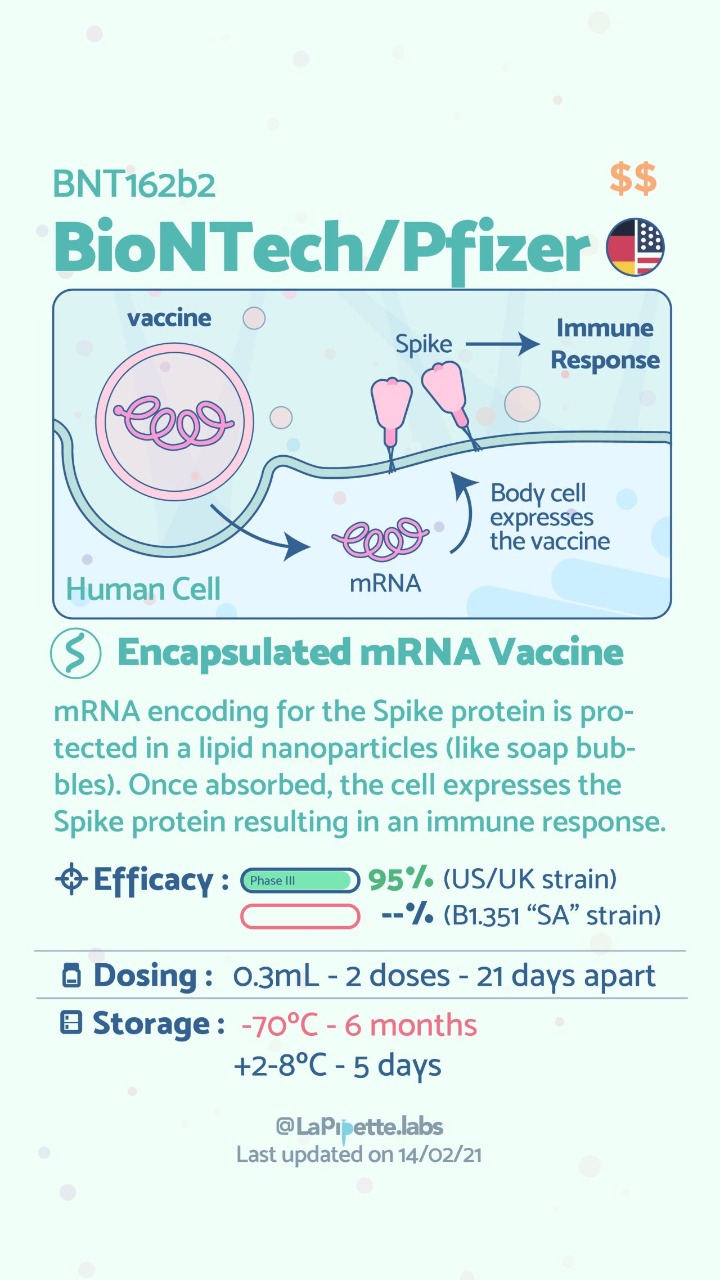
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
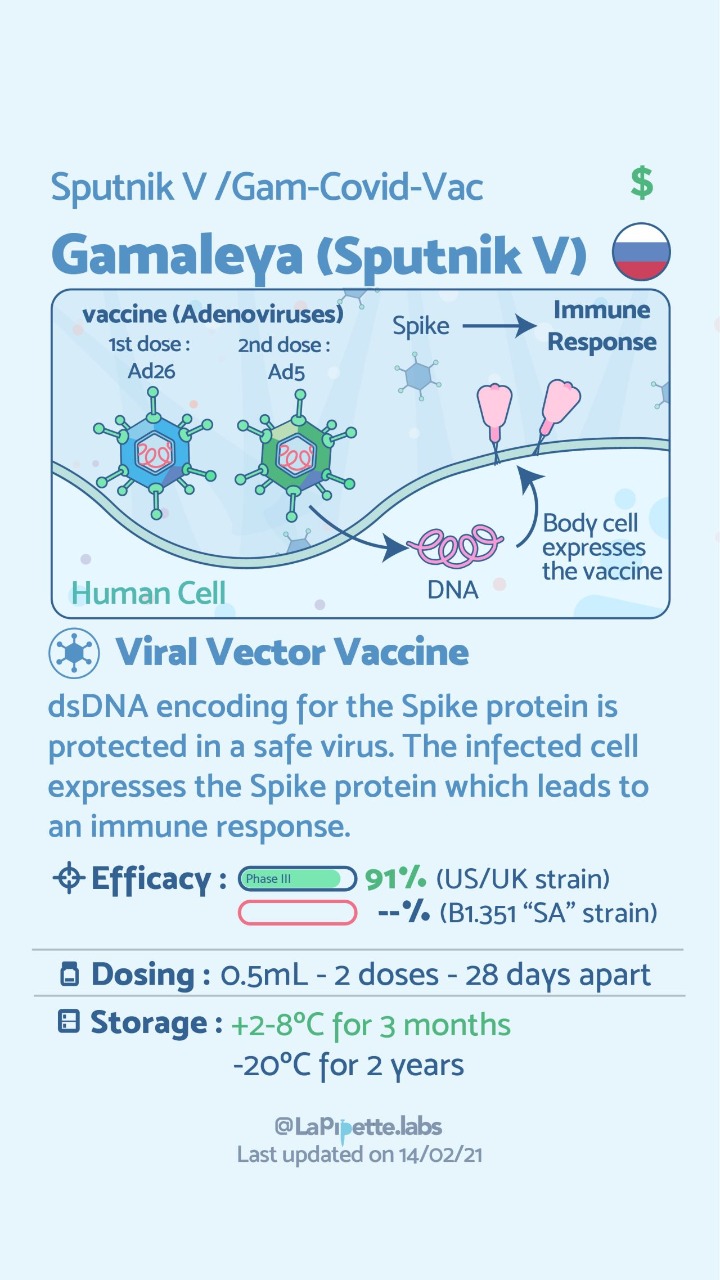
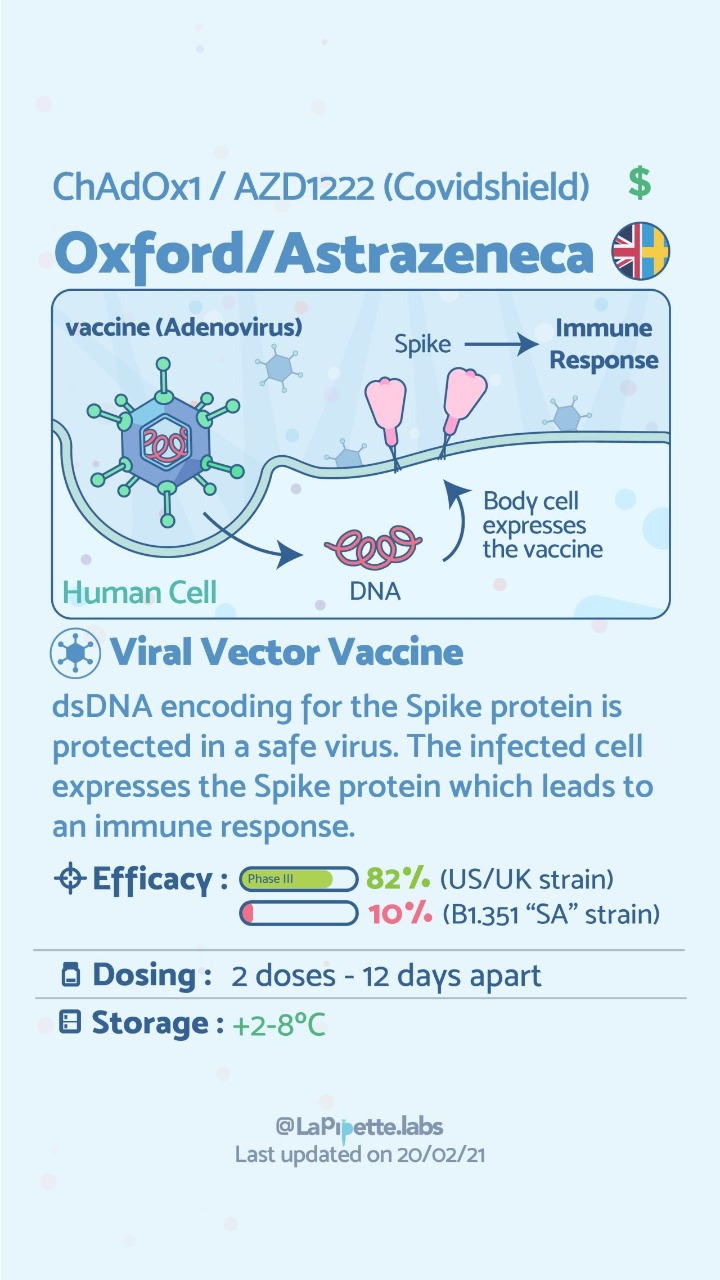
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Vitamin D and Covid -19
May 07, 2020 9:24 am
We are all aware of the many roles that Vitamin D plays in our bodies. This includes immune function in addition to all the regulatory roles that Vitamin D plays in several physiologic reactions. There may be a correlation of low Vitamin D and COVID-19 infection increasing death risk as looked at in research articles.
Covid -19 in a subset of patience causes significant lung injury. These patients require mechanical ventilation.
Previously reported publications have suggested a possible correlation between ace inhibitors and increased risk of pulmonary complications of Covid -19. Some researchers suspect that the Covid-19 may be able to enter lung cells by the ACE receptors.
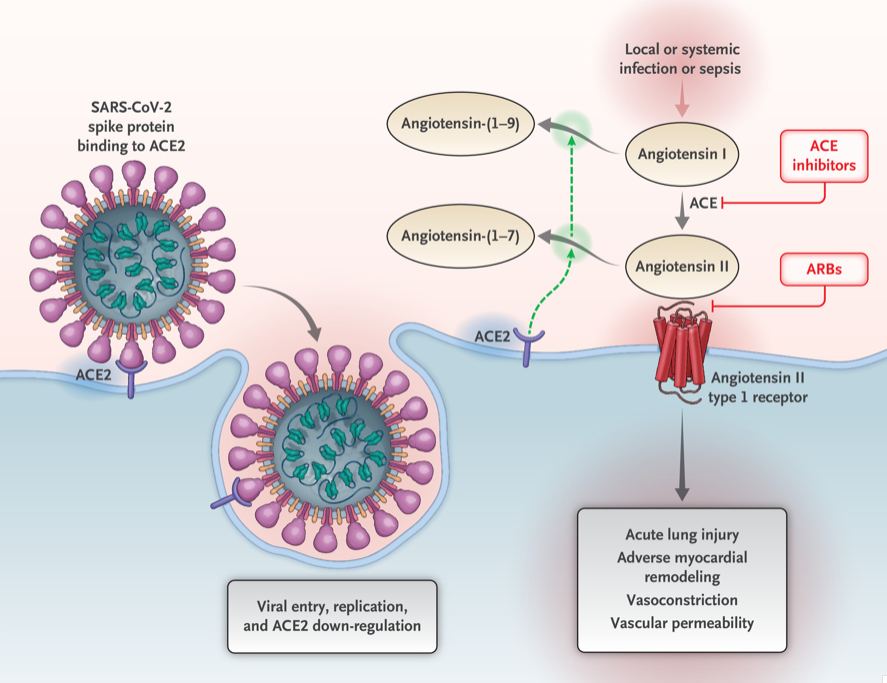
Vitamin D may positively implact the receptor ACE2. This study, report clear correlation between the high death rate with low vitamin D levels in Covid infected patients. There are limitation to this study that the attached abstract outlines.
Our take home message would be to please make sure you have updated labs and that you are all taking the recommended Vitamin D based on your surgical anatomy and laboratory values, not just an average non-bariatric person recommended dose.
https://www.dssurgery.com/wp-content/uploads/2020/05/manuscript.pdf
Protein Intake
October 14, 2019 7:08 am
Protein intake requirements change over time following weight loss surgery. This is based on the requirements imposed on our body by a number of variables. These include, activity level, muscle mass, over all health condition to name a few.
A very young muscular athletic male with a BMI or 30 will require much higher protein intake (and absorption) that an inactive older Female with the same BMI. The same young athletic male will require much higher protein intake is he is recovering from a surgery than his baseline.
As we have stated in the past, the protein intake, should be adequate and not excessive. High level of protein intake that are not accounted for based on muscle mass and activity level, will eventually result in weight gain. The best measure of protein intake in a stable weight patient over 3-4 years post op is their albumin and protein level. Following your yearly laboratory values at a minimum is an important part of weight loss surgery follow up care.
You also need to adjust protein intake when necessary. Protein needs increase depending on physical needs, infection, healing, pregnancy, surgery, age, injury, etc. Plastic surgery requires higher protein needs for appropriate healing.
Information on protein sources and quality here.
The basic formula for protein intake is 1gm/kg of ideal body weight. The calculator below will provide a guide for the protein into based on your stable weight in lbs.
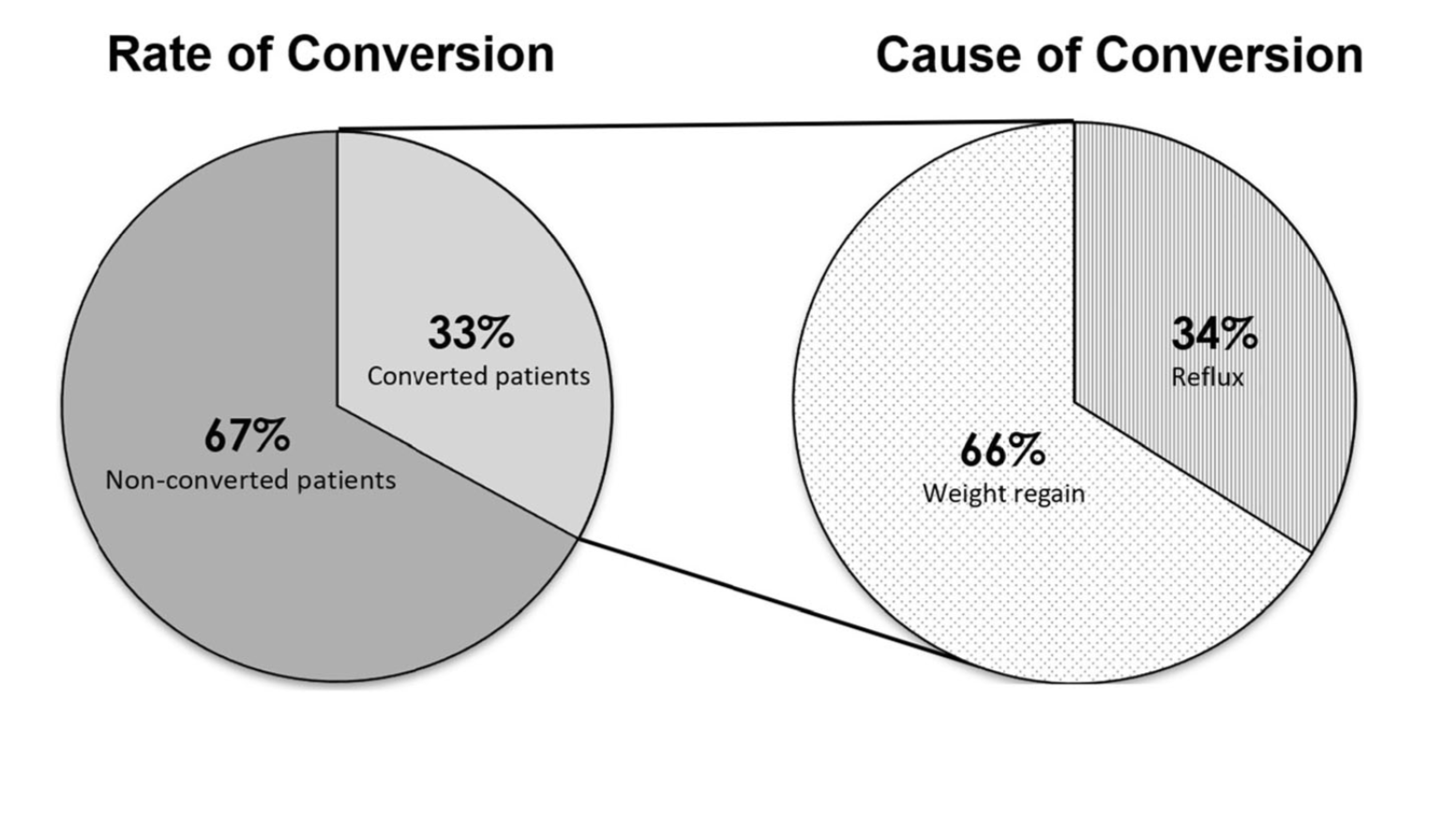
Sleeve And Weight Regain
July 22, 2019 9:50 am
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here
Thyroid Medication Absorption And Weight Loss Surgery
June 10, 2019 8:59 am
Question : “Do I have to take higher dose of thyroid medication after the duodenal switch? ”
Answer : “Maybe”
With all weight loss surgical procedures, there may be changes to absorption of medications. It is easily understood why duodenal switch may results in decreased absorption of fat-soluble medication. What is not as clear is the reduction in absorption of other medication with procedures that do not explicitly change the absorption at the level of the small bowel directly.
The research data is all over on this topic. There is published literature that shows improvement in the thyroid function after gastric bypass and the sleeve gastrectomy. However, the exact mechanism is not completely understood.
There is research that reports “…decreased postoperative levothyroxine requirements.” Other have shows no correlation between the length of the bowel distal to duodenum to absorption of thyroid medication.
With all this confusing data, the best course would be to always “treat the patient and not the lab results.”
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
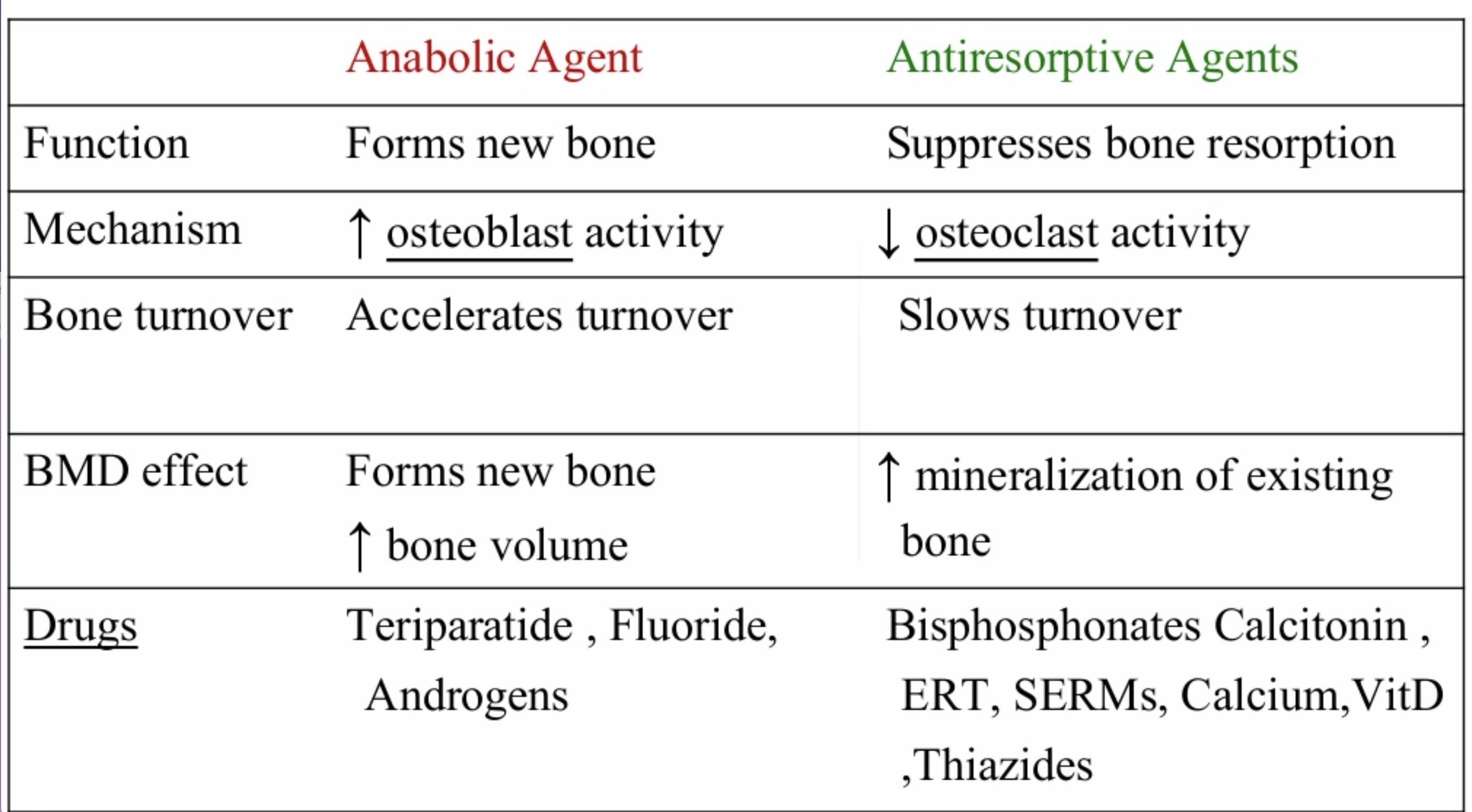
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
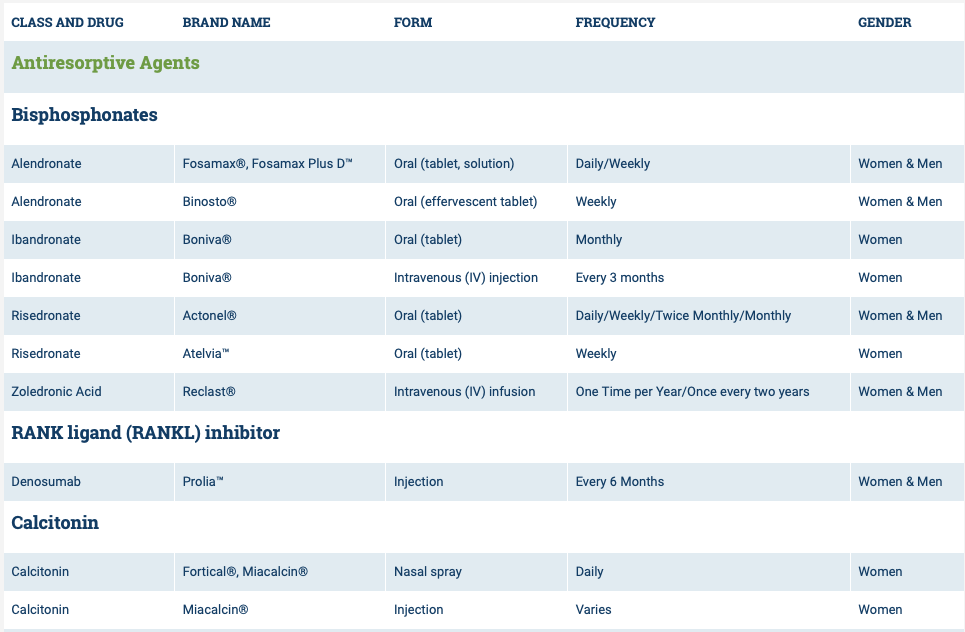
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
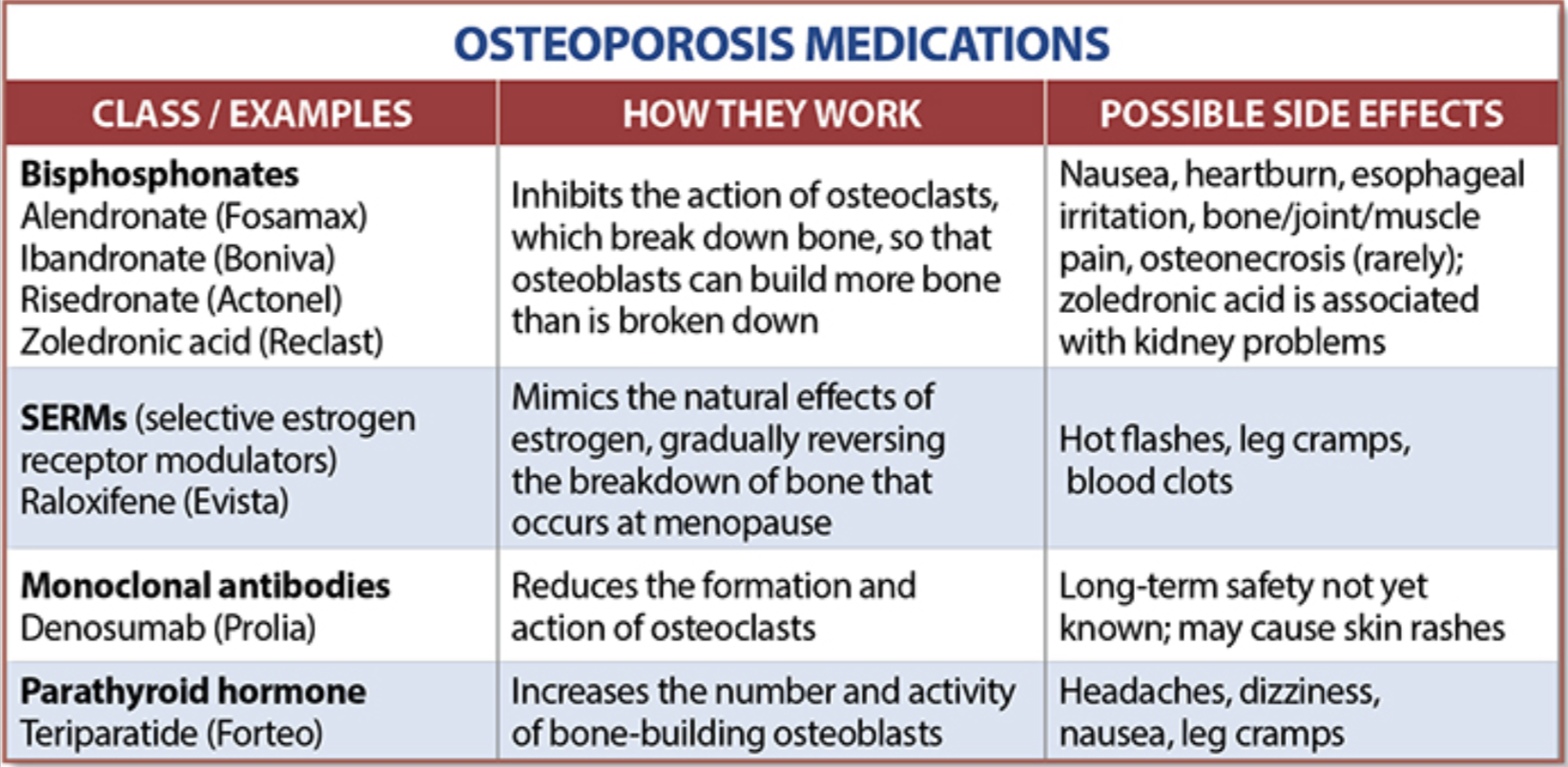
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.