Tag: regain
Diabetes and Weight Loss Surgery
April 06, 2020 5:51 am
The scientific literature is riddled with evidence pointing to the benefit of early metabolic surgery as a superior treatment, remission and possible cure option for diabetes. Unfortunately, the medical education, pharmaceutical companies, primary care healthcare delivery systems and third party payers (health insurance companies) have not caught up with the published data. The American Diabetes Association has changed their guidelines to reflected the benefit for combating diabetes with weight loss surgery.
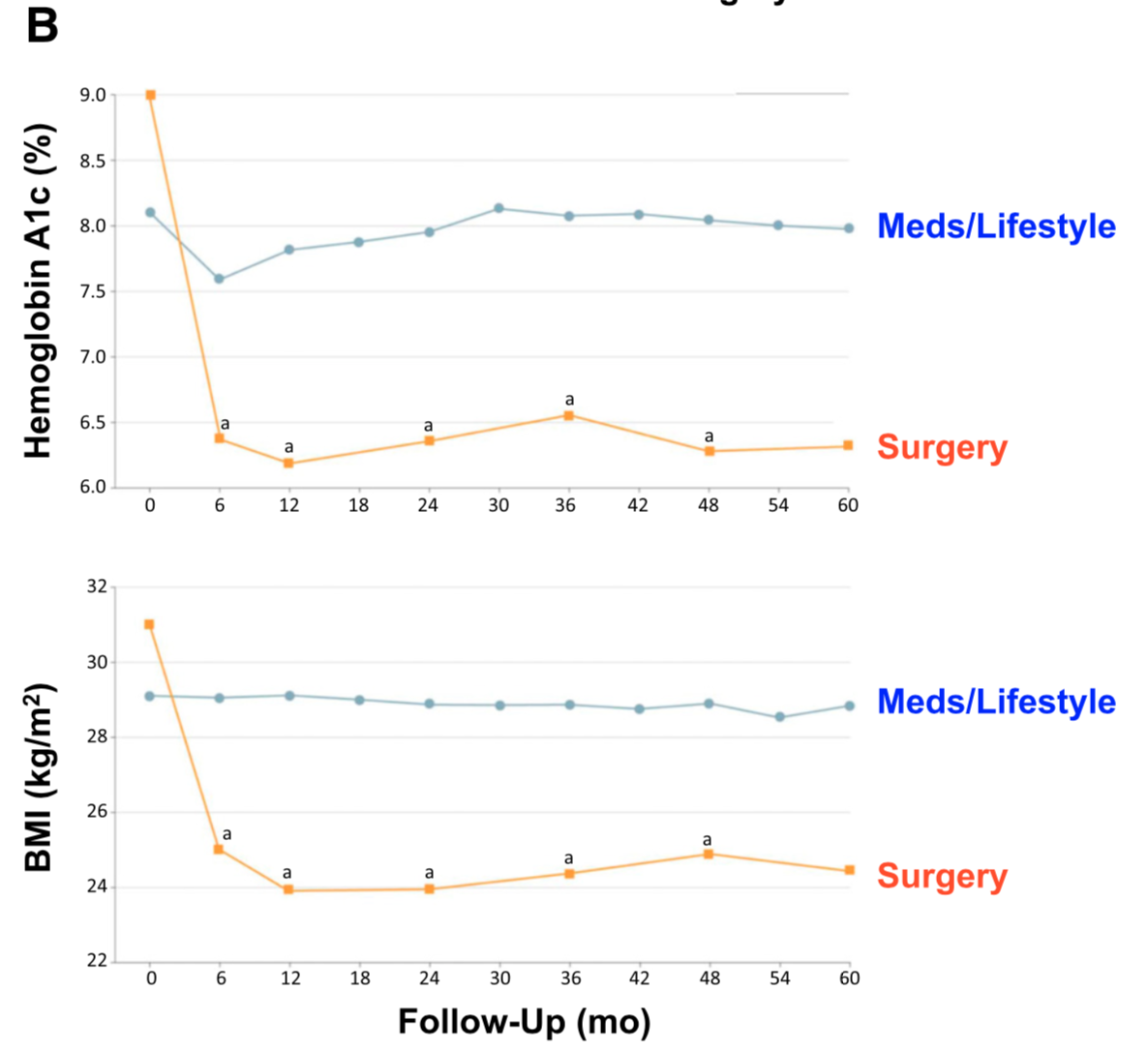
There is ample evidence of the superior outcome of surgery as a treatment option for diabetes when compared to medical managment. Cummings et.al, in a published article in Diabetes Care, showed sustained stabilization of the Hemoglobin A1C six years after surgery. In contrast, there was no significant changes noted in the non-surgical group.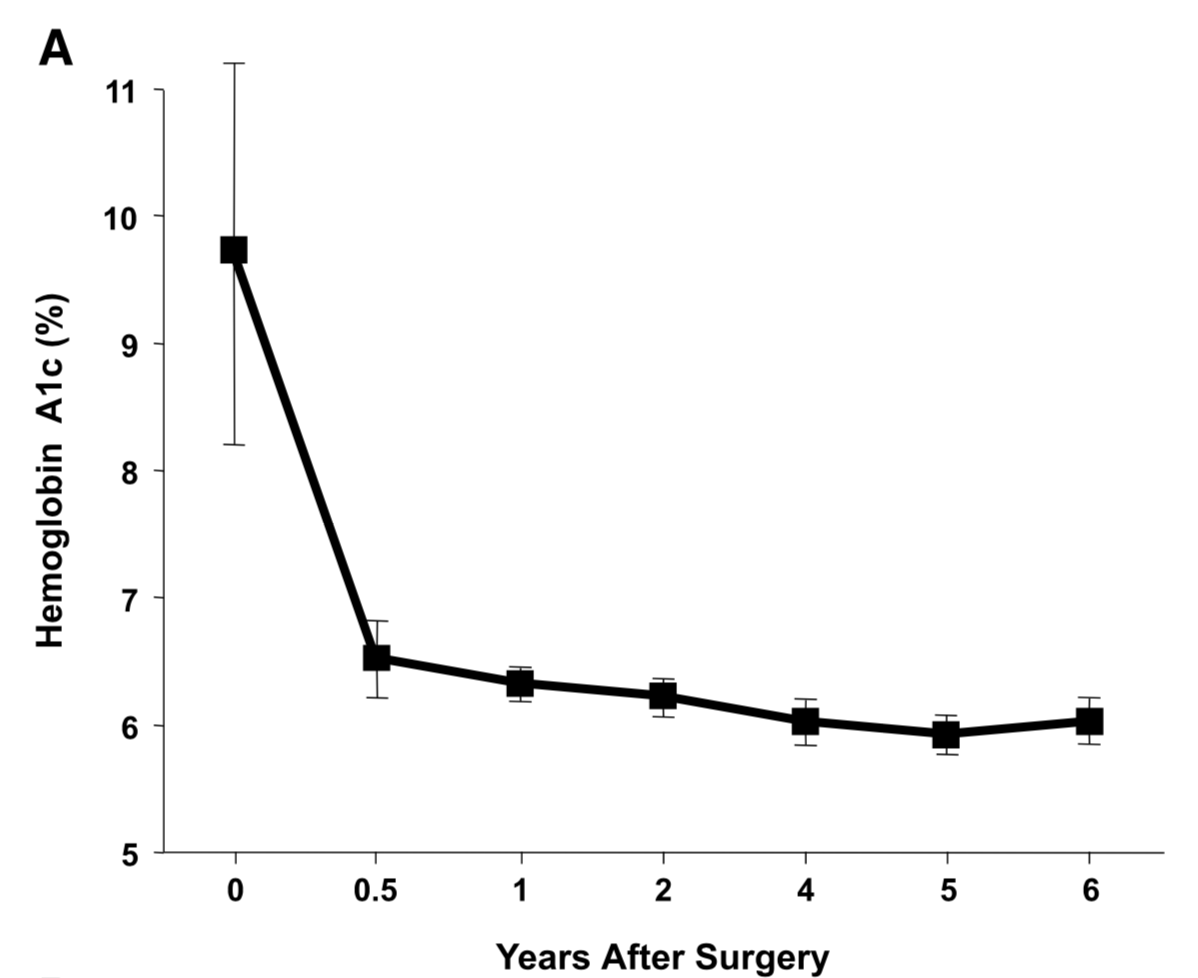
Jans et.al. , in November of 2019 showed that the patients who had NOT been on Insulin, and had metabolic surgery had the highest long term success for resolution and remission of the diabetes. This identifies that having a patient be proactive in their care by having metabolic surgery improves success rates.
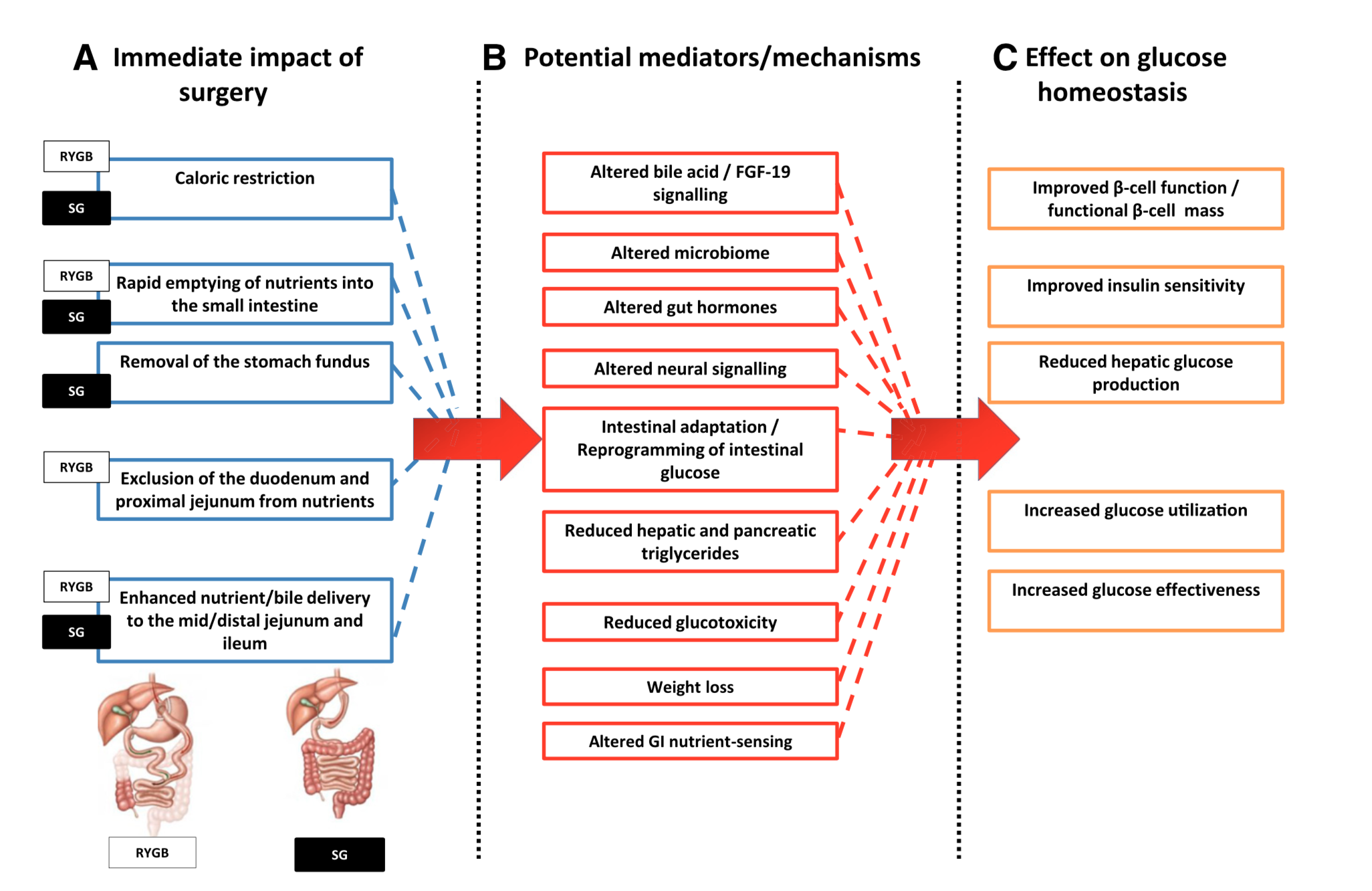
The exact mechanism by which the diabetes is resolved is unclear. The weight loss may play a role. There are numerous hormones and neuroendocrine modulators which control the complex metabolic pathways. Batterham et.al., in Diabetes Care (2016), published a summary overview of the possible mechanism involved in diabetes improvement following metabolic surgery.

There are a number of overlapping and sequential layers for possible reasons why diabetes resolves after weight loss/metabolic surgery. These may be directly related to surgery and the reduction of the calorie intake or absorption. It may also involve the neuroendocrine modulators.
What can be said definitively is that early surgical intervention is best and most likely the only permanent solution to type II diabetic resolution. There is no medical justification in not considering metabolic surgery in diabetic patients who may also have difficulty with meaning a BMI< 35.
Sleeve And Weight Regain
July 22, 2019 9:50 am
2018 Back on Track
January 28, 2018 11:38 am
Join our 2018 Back on Track challenge and let’s get back on track for 2018! The holidays were wonderful but if you find yourself with a few extra souvenirs don’t feel alone. The average American gains between 1-8 pounds during the holiday season and I am no exception. Let’s get back on track 2018 together.
Time to clear out the kitchen! Disposing of temptations and high trigger foods is the first step to getting back on track. Throw it all away and don’t allow them back in. If foods are difficult to acquired then they are less likely to be consumed.
Stock up on high protein and whole, unprocessed foods that are low carbohydrate and nutrient dense. When quality foods are easily available we are more likely to stay on track with the types of foods we should be eating. Simple sugars/carbohydrates are the biggest culprit of holiday weight gain. We need to go back to the basics of hydration, high protein, low carbohydrate/sugar, vitamin/mineral supplements and exercise. Simple sugars and carbohydrates are easy for our bodies to use and absorb. Cutting them out can jump start your weight loss. Each individual needs to identify the daily carbohydrate intake that works for them. Some people stay under 50 grams of carbohydrates daily and some can tolerate more daily grams. You may also need to look at your protein and fat intake. All excess nutrients absorbed have the potential to turn into fat mass and inhibit weight loss. Metabolism video.
Hydration is an important ways to start getting back on track. Water is essential to life functions. The brain is 85% water, blood is 80% and muscle is about 70% water. Hydration aids in digestion, eliminating waste, byproducts and toxins. It also can decrease the feeling of hunger. Lack of hydration can increase fatigue which can lead to craving high carbohydrate foods to increase energy.
Protein’s importance in almost every bodily function and muscle mass can not be ignored. High quality complete Protein sustains muscle mass during weight loss, aids immunity, antioxidant function, and enhances leptin and insulin function. Filling up on protein first will help with carbohydrate carvings and give a sustained satisfied feeling. A prior blog post gives additional information on the importance of protein and the effects of protein malnutrition. WLS makes daily protein intake important but especially after Duodenal Switch, protein is a necessity of daily life.
Vitamins, minerals and supplements will ensure the body has the nutrients it needs to function adequately and can keep cravings at bay. Deficiencies in vitamins and minerals can cause cravings for foods. Vitamin and minerals are essential to muscle function, red blood cell production, bone health, and numerous other physiologic functions. We may all slack off on our supplements occasionally but now is the time to get back into the habit of daily vitamins and mineral supplements. A daily vitamin, mineral, and supplement routine is a lifetime commitment after Duodenal Switch or any WLS. Here is a list of commonly used supplements. If you haven’t kept up with your minimum yearly laboratory studies, now is the time to be seen and have your labs done.
Exercise can increase weight loss, overall well being, mental well being, mood, alertness, improve digestion, improve sleep, and increases energy levels. Exercise does not have to be a daunting task. Simply adding 15-30 minutes of activity can give added benefits. Yoga, walking, dancing, lifting weights, hiking, and sports activities can be included or added to more traditional forms of exercise. There are many free online videos for all types of exercise available. This year we are teamed up with The Kinesis Centre to offer a 4 week training program that can be accessed from anywhere. A 4 week training program will be included in our 2018 Back On Track Grand prize.
Finding a new hobby can keep both your hands and mind busy, curbing the unconscious eating of foods that are high in sugar and carbohydrates. Adult coloring books, drawing, painting, knitting, crocheting, sewing, dance lessons, gardening, learning to play an instrument and many others are great ways to use your time and expand your quality of life and brain function. New hobbies can also help establish new coping skills. Our previous post on Coping Skills After Bariatric Surgery can be found here. There are a whole host of online videos for “how to” on new hobbies.


Teaming up with others can also help increase weight loss and compliance. Support from friends, family and other groups will assist you. There is a whole gamut of support group online and in person. If you have fallen out of the habit of attending our support group or webinars get back to them. You can find our schedule and announcements regarding webinars here. Our Central Valley Bariatric Facebook page also gives daily inspirational messages, protein recipes and articles and any new information or research available. There is also our Duodenal Switch Facebook Group. Anything that increases accountability is a benefit and motivates us to stay on track.
Experiment with new recipes and flavors that are bariatric friendly and within your dietary needs. There are so many options for quick and easy meals that are whole foods, high protein, and low carbohydrate. We have several recipes on our page for all stages following weight loss surgery and Duodenal Switch. However, there are endless option on the internet in Paleo, low carb, and high protein type recipes.
In the spirit of new starts and getting back on track 2018, we are having a giveaway with the basics to get back into the swing of things. This year we are looking for before and after weight loss surgical journeys for our Grand Prize. Share your weight loss journey! Don’t be shy, your journey can inspire others and/or motivate yourself. To enter the Back on Track 2018 Giveaway, please submit your weight loss surgical journey with before and after pictures to [email protected] or you can also post your before and after pictures on our Facebook page. You will also need to sign a release for the use of your story on our website. We will draw 2 names from those that enter by announcing it on our FaceBook page or by e-mail on February 14, 2018. You must submit your mailing information to [email protected] in order to claim the prize. You must be a verifiable patient of Dr. Ara Keshishian.
We are also doing 3 prizes of a 4 week training with the Kinesis Centre if you share an achievement picture on our FaceBook page . This achievement picture can be a milestone in your journey, something you’ve haven’t done before, a non-scale victory, a goal that you reached, anything that you are proud of achieving. Let’s do this 2018 Back on Track challenge!
Please remember that medications, health status, age, bowel motility, genetics, and diet all play a role in weight and weight maintenance. Please have a physician review your health history and medications.
*NOTE: Giveaway items may or may not be identical to the pictured items.
We are not affiliated with any of the products nor do we endorse any one type of product. There is no cash value to the prizes.
Revision from failed AGB to Duodenal Switch
January 10, 2018 2:10 pm
A few times a month during consultation for weight loss surgery , I’m ask as to why I do not offer the adjustable gastric banding as an alternative to the patients. As I have said over the years when a patient considers an weight loss surgery the totality of the risk should be considered. This includes the operative, immediate postoperative course, the maintenance and the follow-ups needed. The potential complications of the procedure in addition to the long-term success off each operation should also be taken into account.
Unfortunately, some patients are led to believe that any perceived benefit in the short operative time and the ease of the adjustable gastric banding also translates to a better outcome. This is in fact the opposite of what the published data have shown, a recent study published in April 2017 by Vinzes et.al, shows that 71% of patient lost their band by 10 years out.




What is also interesting that more patients underwent revision from failed AGB to the duodenal switch than the sleeve gastrectomy (Fig 1.). This is what I also recommend.
More importantly, The patients who underwent a revision from failed AGB to the duodenal switch operation had the best long term results of all patients (Fig 2.) note the “rBPD” line that is the highest of %EBMIL.
Complication’s were broad and frequent (Table 3.)
Further information on revision from failed AGB to Duodenal Switch or other failed weight loss surgeries can be found here.
Resistance Exercise BandsExclusive Member Content
July 19, 2017 12:47 pm
Standard Common Channel In Duodenal Switch Will Result In Weight Regain.
December 16, 2016 1:57 pm
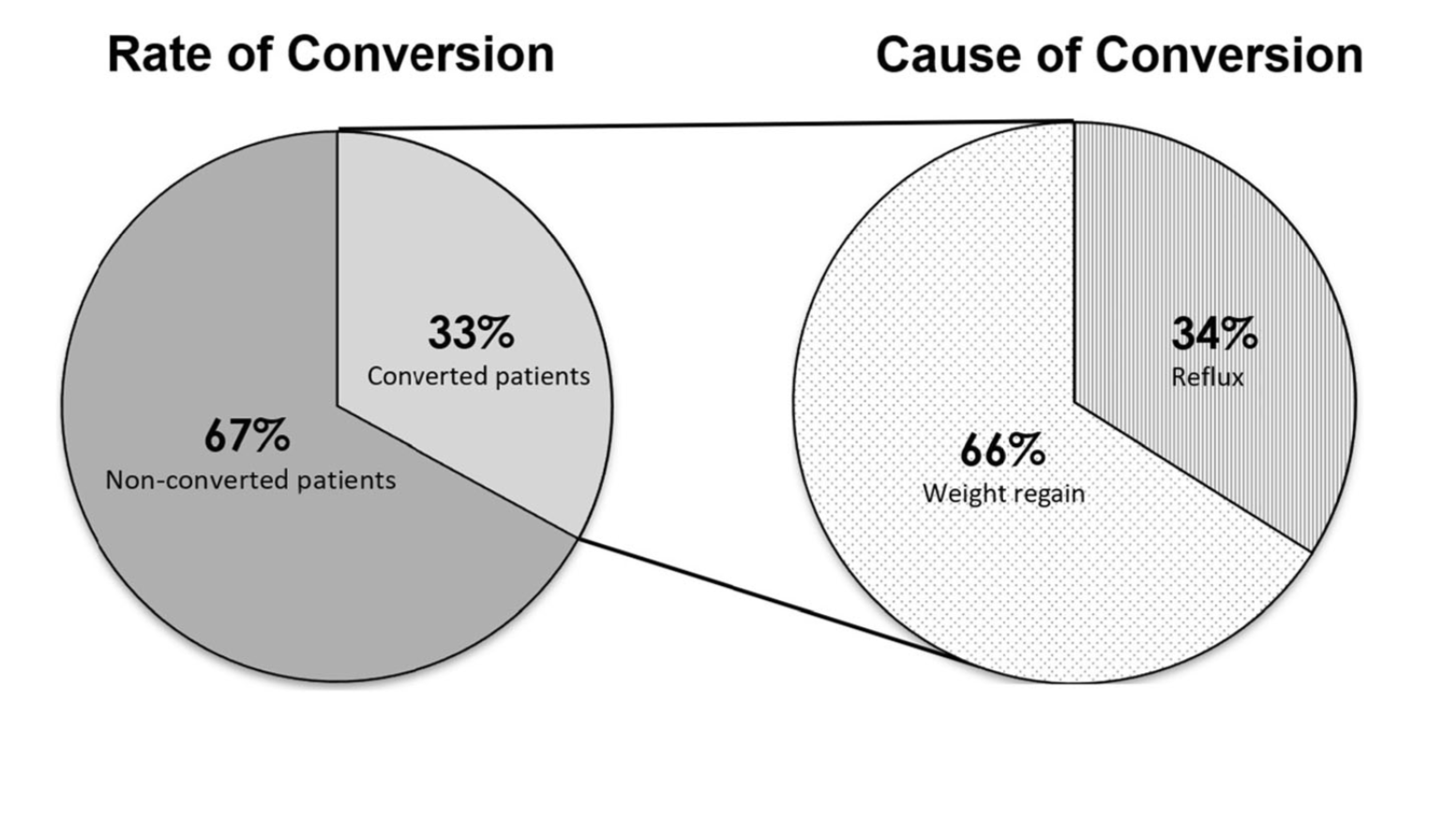
Stéfane Lebel, M.D.*, Geneviève Dion, M.D., Simon Marceau, M.D., Simon Biron, M.D., M.Sc., Maud Robert, M.D., Laurent Biertho, M.D. earlier this year released a research article comparing patients undergoing standard common channel of 100cm and standard common channel 200cm. The conclusion of this article was: “In this population, BPD-DS with a 200-cm common channel offered similar remission rate of co-morbidities compared with standard BPD-DS. It was associated with similar weight loss at nadir, followed by a more significant weight regain. It might yield a lower rate of nutritional complications. Long-term randomized data are needed to detect other potential advantages.”
Our Experience:
One of the most dreaded outcomes of any weight loss surgical procedure is weight regain. This is assuming that initial adequate weight was lost to result in resolution of the co-morbidities in the first place. As the weight loss surgical field has changed over the years so has been the cases of regain that we have seen.
There was a time when Lap bands were being revised for inadequate weight loss and weight regain. Not to mention the complications of reflux, difficulty swallowing and persistent Nausea and vomiting. Then as more Gastric bypass procedures “aged” the number of patients that started looking for revision for weight regain increased. The latest fad is the Vertical Sleeve Gastrectomy that are done with false sense of expectation and results. The long term outcome of Vertical Sleeve Gastrectomy is no where close to that of the Duodenal Switch, independent of the size of the sleeve. In fact, more surgeons are trying to get a little more weight loss by making the sleeve too tight. All they are doing is creating a significant and debilitating set of problems such as reflux, nausea, and solid intolerance.
The ideal revisional procedure for these patients should be the Duodenal Switch. Some surgeons, however, have started advocating “single anastomosis” knock off the duodenal switch. Others do “standard length common channel” rather than a Hess method Duodenal Switch. I have always performed a traditional Hess method Duodenal Switch. The Hess method Duodenal Switch has held the largest and longest excess weight loss maintenance for 28 years, going into 29 years. Here is a past blog regarding small bowel length.
The predetermined standard common channel results in weight regain. Study
Don’t lose your Pyloric Valve over a Failed Gastric Sleeve
June 22, 2016 9:32 am
In my opinion, there are very few reasons to lose your Pyloric Valve after sleeve gastrectomy. Recently, I am hearing of people who have had regain due to a failed Sleeve Gastrectomy being revised to Gastric Bypass RNY and then seeking a Duodenal Switch due to regain from Gastric Bypass RNY. A better option is to go from Sleeve Gastrectomy to Duodenal Switch, due to the long term excess weight loss maintenance of Duodenal Switch. The benefit of the pyloric valve can not be taken lightly.
Let’s start by reminding ourselves as to how the Sleeve Gastrectomy has gained popularity. In the quest for a simple solution to the complex problem of obesity, adjustable gastric banding gained popularity only fail to deliver anything close with the results that were promoted and heavily marketed. The focus was then changed to another seemingly simple procedure, laparoscopic sleeve gastrectomy. For some surgeons this is a new procedure. Surgeons that had been doing the duodenal switch operation for decades, sleeve gastrectomy has not been a new procedure. Surgeons that just started doing sleeve gastrectomy as a stand alone procedure started experiencing complications of the sleeve gastrectomy, such as regain and are now looking for another option for these patients. This complication are even more frequent when they’re done following a failed adjustable gastric band procedures due to the metabolic issues after revising one weight loss surgery to another. A similar short sighted approach is also being promoted with SIPS/SADI procedures, which is significantly simpler to perform than the duodenal switch operation.


Laparoscopic sleeve gastrectomy has a predictable profile for weight loss. It will not have as good on the long-term success rate as a duodenal switch operation. Complications of the sleeve gastrectomy including reflux, stricture, fistula, inadequate weight loss which may warrant evaluation and possible intervention. In my opinion, as a surgeon who does the duodenal switch operation routinely, a sleeve gastrectomy requiring revision should almost never be revised to a gastric bypass. I have seen number of patient’s who have had an adjustable gastric banding which was revised to the sleeve gastrectomy then to a gastric bypass. We are contacted for a possible revision to Duodenal Switch operation because of the weight regain. One can argue that the patient should not have had the sleeve gastrectomy or gastric bypass. It is critical that the complexity of the disease of the obesity is clearly appreciated that it purely restrictive procedure will not yield the desirable outcome long-term.
Benefits of the Pyloric Valve:
The pylorus is the valve located at the end of the stomach. It controls the release of the liquid mixture of food from the stomach into the small intestine.
The body naturally regulates the passage of food, so food will stay in the stomach for a certain period of time. We believe it is very important to continue that feeling of fullness in between meals. As a result, one of the principle functions of the pyloric valve is to regulate the amount of food products released into the small intestine where they are absorbed. This helps prevent dumping syndrome and ulceration.
The bodies natural diameter of stomach, pyloric valve and small intestine is left intact. This elevates stretching of the stomas created by RNY Gastric Bypass.
Summary
These failed Sleeve Gastrectomies should be revised to Duodenal Switch unless there are overwhelming health issues that would require another option. I always suggest several opinions from different Bariatric Surgeon’s who do a variety of Weight Loss Surgeries before deciding which type of revision to proceed with.
Shared Success Story Update- Cyndi RNY to Duodenal Switch
June 06, 2016 6:37 am
Three Years Out Cyndi E … RNY to Duodenal Switch Revision
The Journey to get to the three year mark, has been amazing! And truly, The JOY is in the JOURNEY.
I am a JOYFUL “Third Time’s the Charm Revisionista”…. This is my new title…. And I say this proudly!!
For too many years (like 45! at least) I carried the shame and blame of being overweight and beat myself up on the inside. I tried everything, from age 13. I tried every diet, every program, and yes, I will say it, I have had THREE, yes THREE surgeries. And then, I let others convince me, and I bought into this, that I was a failure… BUT, I am not a failure. Surgery fails. For a long time, I could not say that, again with the SHAME word. BUT, I am done with shame, and I am done with blame. I no longer blame myself and I no longer shame myself or my body, because now, she and I, my body and I, are friends, and we are nice to each other.
Thankfully for me, I was in the right place at the right time, and met Dr. Ara Keshishian… My story with Dr. Keshishian, is simple. Dr. K was the first Doctor that did not blame me for my weight. He explained that each weight loss surgery has different measures of success, and percentages by weight loss surgery and outcomes. He educated me. He did not blame or shame me, he encouraged me. He also did an Endoscopy and found that I has a Gastro-Gastric Fistula. Simply put, this was an abnormal connection between the bypassed stomach and the small pouch created by the RNY Gastric Bypass surgery. Food could travel two ways, thus rendering the Gastric Bypass ineffective causing weight gain.



Dr. Keshishian performed my revision from RNY to Duodenal Switch on May 31, 2013. The procedure corrected my anatomy, enabling me to lose weight and regain my health. I have no complications, no issues post surgery.
Today, being a “Three Year Old” RNY to Duodenal Switch revisionista, I have a better perspective as a relative “newbie”. I am not a prisoner of my weight. I have lost 125-130 pounds, I am 5’12” (6 feet lol) 61 years old and for the first time in my life at a NORMAL WEIGHT! I do not fear, any longer, that I will gain my weight back. I am, however, mindful that I am consistent in my new habits and patterns that I have put in place, that keep me on track. I am also accountable. To myself, also to my Weight Loss Support Group, here in Paso Robles, to some fellow DS girlfriends that
I talk with about challenges, and with Dr. Keshishian. I am not held captive by my limitations, or my weight, and now I live with the possibilities each day brings and the fun challenges I put in front of me to conquer.
To the “newbies” I say, please take your time, treat yourself kindly, with your inner voice. This is not a race, this is a journey. Don’t rush, it’s ok to take it slow, listen to your body. And do not compare your journey to anyone else. You are you! You do you! You can do this well, one day at a time. Listen to the sage advice of those who went before you. We too have learned by trial and error. Be willing to sacrifice in the short term, for the gift of the long term life. Your DS is forgiving, you be forgiving as well!!!
Remember: WATER, PROTEIN, SUPPLEMENTS, EVERYTHING ELSE, EAT CLOSE TO THE DIRT, ELMO DIET
With JOY, Cyndi
Inadequate Weight loss and Weight Regain
May 24, 2016 7:56 am
There were numerous causes for the inadequate weight loss and or weight regain after weight loss surgery.
These factors may include:
1-Type of the surgery: Duodenal Switch, RNY, Adjustable Gastric Banding, Intragastric Balloon, etc.
2-Patients metabolic state (age, activity level, hormones state etc)
3-Co-morbidities
4-Patient compliance
5-Other
Each and every one of these may be an independent factor or may be a contributing cause.
In our experience, patients non-compliance is not as common as others believe. Frequently, we see patients in our office where they have been told that the poor outcome of the surgery is “their fault”
We see this with RNY, and Band patients as well as some of the duodenal switch patients who are seeking advice for weight regain or inadequate weight loss.
I would like to talk about the issues of inadequate weight loss or regain post Duodenal Switch specifically. Duodenal switch operation as described by Dr. Hess, outlined the division of the small bowel lengths to be proportional to each and every patients own total bowel lengths. This meant that two patients with the same BMI and weight will end up with two different lengths for common and alimentary limbs if there total length of the bowel is different. Unfortunately, too often patients are given a “standard” or “set” ( not clear what that word means, since there is no established standard in the literature) length for common channels and alimentary channels regardless of the total small bowel length. In some patients, those lengths may result in acceptable weight loss. However, quite frequently a patient with a preselected length for the common and alimentary limbs will end up either loosing too much weight and have nutritional problems or not loose adequate weight. As with all practices, we have over the years had patients who have had nutritional deficiencies and excessive weight loss or have had inadequate weight loss. Looking at the raw numbers however, we have had more patient from other practices that have come to us for revisions and corrections of lengths of the bowel lengths from other practices that our own patients have required.
Another level of the confusion is the improper interchanging of the “SIPS and SADI” procedures with the duodenal switch operation. As I have said in the past repeatedly, SIPS and SAID are not the same as the duodenal switch- and attempt to call these different procedures the same is misleading to say the least.
The other category of weight regain or inadequate weight loss includes medications and new health issues. Discussed in a previous blog, there are many medications that can influence weight gain. It is important to work with your health care provider to find medications that have a positive effect on symptoms without added side effects whenever possible.
In summary, weight re-gain or inadequate weight loss can have many facets. However, surgical technique can provide an advantage. Each aspect should be addressed and identified.
Metabolic Processes In Different TissuesExclusive Member Content
February 11, 2016 8:29 am