Category: Birth control
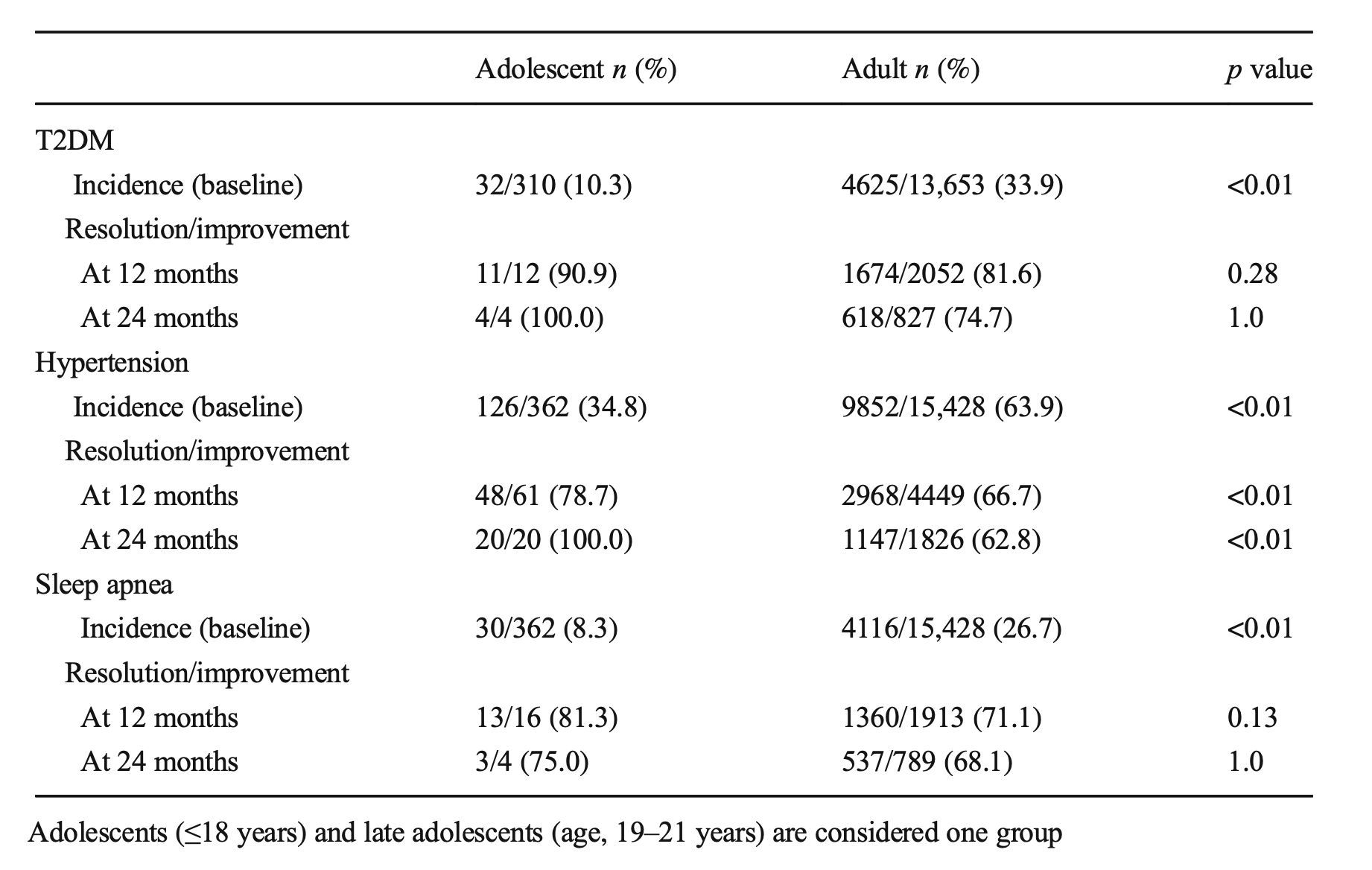
Sleeve Gastrectomy in Adolescent patients
September 23, 2020 5:44 am
PolyCystic Ovarian Syndrome PCOS
September 04, 2018 9:58 am
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.

Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
Bariatric Surgery can improve PCOS in those individuals with Type 2 Diabetes Mellitus. Further information on weight loss surgery and its effect on PCOS here.
Pregnancy And Weight Loss Surgery
November 21, 2015 5:34 pm
This is not a substitution for formal medical advise that should be given to any patient by their bariatric surgeon and and OB/GYN familiar and experienced in the care of female patients with history of weight loss surgery. This is information that we provide our patients when we are notified of their pregnancy.
We recommend and instruct to take all precautions to avoid getting pregnant within the first 18 to 24 months following weight loss surgery. There is a significant amount of information about preferable birth controls, those to avoid, and additional pertinent information on our website.
Women who become pregnant after Weight Loss Surgery (WLS) should receive specific attention from their obstetrician because of the high risk nature of their pregnancy. Please make sure that you share this information with your OB/GYN. Many patients have become pregnant and delivered health babies after Duodenal switch (DS) without difficulty, but you do need to be watched more closely. The scientific study favor patients getting pregnant after DS when their weight loss , and nutritional markers have stabilized (18 months or longer) and not before. You also need to make sure you are taking all necessary vitamins, minerals and protein.
The first trimester is a very important time in the development of the fetus. Most organs and structures of the fetus are formed in the first trimester and therefore it is imperative that you pay close attention to your nutrition and your nutritional supplements.
You should continue to take your general multivitamins, other vitamins, minerals and your calcium as you were taking prior to getting pregnant. In addition, you should also take what will be prescribed by your OB/GYN. Do not substitute your prenatal vitamin and any other supplements that you are prescribed by your OB/GYN with what you were prescribed by our office. Each patient’s situation is individualized and additional changes or supplementations may be needed based on the advice of your surgeon and OB/GYN. Multiple fetus pregnancies require additional vitamin, mineral and protein needs.
A good prenatal vitamin should contain these:
Vitamin C – is essential for tissue repair, wound and bone healing and increases the body’s resistance to infection. For mother and baby this vitamin is essential daily as it is the agent that holds newly formed cells together. Helps baby to grow and builds strong bones and teeth. It is also instrumental in the body’s ability to absorb iron.
Vitamin D – promotes general growth. It maintains proper levels of calcium and phosphorus thus helping to build baby’s bones and teeth.
B Vitamins (thiamine, vitamin B6, riboflavin) – Thiamine converts carbohydrates into energy for mother and baby and is essential for baby’s brain development. It also aids in normal functioning of the nervous system and heart. If deficient during pregnancy, a baby is at risk for beriberi, a serious heart ailment. Vitamin B6 is also vital to develop your baby’s brain and nervous system. Riboflavin helps the body to produce energy. It promotes growth, good vision and healthy skin for mom and is important for the development of the baby’s bone, muscle and nervous system.
Folic Acid – is one of the B Vitamins that is needed to produce red blood cells. It helps synthesize DNA, is conducive to normal brain functions and is a critical part of spinal fluid, thus making it one of the few nutrients known to prevent neural tube defects such as spina bifida.
Calcium – your developing baby needs this mineral to grow strong bones and teeth, healthy nerves and muscles and to develop normal heart rhythm and blood clotting.
Potassium – is a mineral that helps maintain fluid balance in the body. This mineral helps regulate blood pressure, nerve impulses and muscle contractions.
Vitamin A – is important for cell growth, healthy skin and mucous membranes, and resistance to infections. It benefits red blood cell production in both mother and baby. This vitamin is essential for postpartum tissue repair.
Copper – a trace mineral found in all plant and animal tissues; it’s essential for forming red blood cells-a key process during pregnancy, when your blood supply doubles. Copper also aids tissue growth, glucose metabolism, and growth of healthy hair. It also helps form a baby’s heart, skeletal and nervous systems, arteries, and blood vessels.
Pantothenic Acid – is a trace mineral that regulates the body’s adrenal activity, antibody production, and the growth and metabolism of protein and fats. If you are deficient in this vitamin during pregnancy your baby’s growth may be slowed. This trace mineral is required for many essential functions, including growth, appetite regulation, digestion, wound healing, and the maintenance of collagen and elastin which may explain why some doctors think it may also help prevent stretch marks, one of the banes of pregnancy.
Iron – makes red blood cells, supplies oxygen to cells for energy and growth and builds bones and teeth. In pregnancy this mineral is so crucial because the body must produce extra blood to support the growing baby. During pregnancy you will need double the recommended daily allowance of iron to insure your health and that of your baby’s.
More often than not, many expectant mothers find taking a prenatal vitamin increases nausea in early pregnancy and sometimes beyond. If this happens, ask your doctor or midwife to change your formula or it may help to change how and when you take your vitamin. It is sometimes helpful to take your prenatal vitamins before you go to bed at night. If swallowing a large pill is difficult, cut it in half. In any event just like your mother said all those years, don’t forget to take your vitamin.
The following are important vitamin and nutritional components throughout the pregnancy but in particular the first trimester.
- Folic Acid: one of the B vitamins has been found to prevent neural tube defects (NTD). Increased intake of folic acid reduces the risk of NTDs such as anencephaly and spina bifida (open spine) by as much as 50 to 70% if women take enough before conception and in the early months of pregnancy. Take your general multivitamin and prenatal vitamin every day.
- Vitamin A: important to prevent blindness in the fetus. Vitamin A levels should be drawn and monitored prior to becoming pregnant and during the pregnancy to ensure adequate intake. You may need to take additional Vitamin A in a Dry water-soluble form such as Biotech Vitamin A 25. Please contact your surgeons office if your Vitamin A levels are below normal, or have not been drawn recently.
- Vitamin D: important for bone growth and formation. Vitamin D levels should be drawn prior to becoming pregnant and during the pregnancy to ensure adequate intake. Dry water-soluble form of Vitamin D3 such as Biotech D3 50. There is some research that adequate Vitamin D levels help protect against pre-term labor and an increase in preeclampsia risk.
- Protein: necessary in all structural formation of the fetus and the mother needs to increase protein intake by a minimum of 30 grams daily. Protein is need in nearly all fetal tissue formation.
The second and third trimesters are important in the growth, development and formation of bone structure and the overall growth of the fetus. It is important at this point to continue taking a minimum of 1500 mg Calcium (or what was prescribed by your surgeon), increased protein intake, your multivitamin, prenatal vitamin and any other supplements prescribed by your OB/GYN or surgeon. You may also need to increase your calorie intake with nutritious foods included in a healthy, well balance diet.
If you have any questions please contact your surgeon or the OBGYN. Your surgeon should also be willing to discuss any concerns that you or your OB/GYN may have with them.
Here is an discussion about the outcome of pregnancy after weight loss surgery.
In general we also advice against certain types of birth control because of the associated weight gain reported by the manufacturers. This is a decision that needs to be made after considering all potential side effects including the potential weight related issues. Ease of use should not be the only variable.
As indicated at the beginning of this blog, the information provided here is not a substitute for your nutritional evaluation by your bariatric surgeon or an experienced OB/GYN.
“Depo” Shot and Weight Gain
September 16, 2013 4:14 pm
Female patients having weight loss surgery should use two forms of Birth control for 18 months after weight loss surgery. Depo shots are suppose to prevent ovulation for a prolonged period of time. An attractive aspect of it is once a patient get the injection, there is not need to worry about birth control till the next injection is due.
There have been a number of studies that have associated Depo shots with weight gain.
Below are three citations from pubmed and the ACOG website.

Weight Gain
