Tag: Duodenal Switch
Sphincter of Oddi Dysfunction
April 26, 2026 8:43 am
Description:
Sphincter of Oddi Dysfunction (SOD) is a clinical syndrome characterized by biliary/ pancreatic pain from abnormal function or obstruction of the.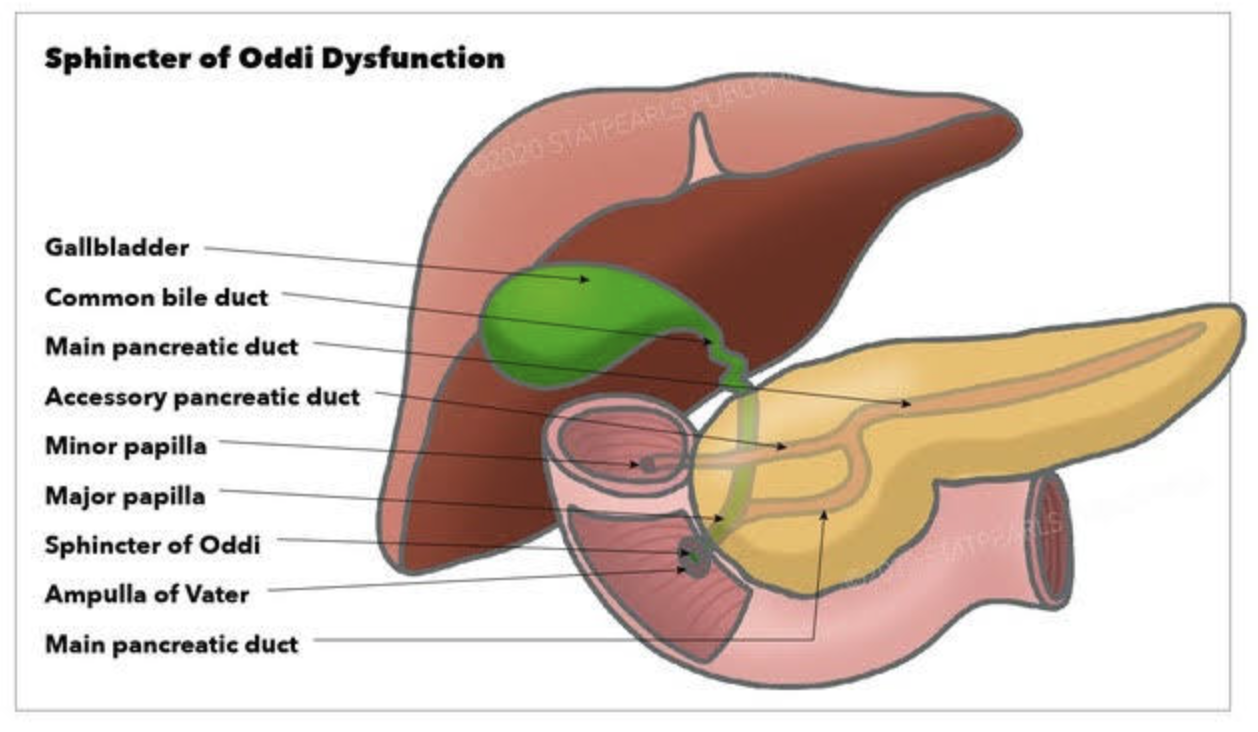
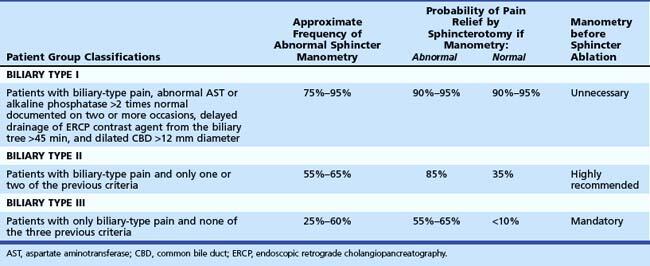
Diagnostic and classification
- The SOD spectrum includes biliary, pancreatic, or combined sphincter dysfunction, with symptoms driven by dyskinesia or mechanical obstruction. The term SOD encompasses both functional motility disorders (biliary or pancreatic sphincter dysfunction) and mechanical obstructions such as papillary stenosis.
- SOM has been considered the gold standard for diagnosing elevated basal sphincter pressure. It is invasive and carries complications, including pancreatitis. SOM can also not be done in those who have had gastric bypass or duodenal switch operations. Sphincterotomy outcome is not uniform. Consequently, many centers have moved toward empiric endoscopic therapy for appropriately selected patients and toward noninvasive or less invasive diagnostic approaches for others.
Treatment approaches
- Endoscopic biliary sphincterotomy (EST) is the most established nonpharmacologic treatment for biliary SOD, particularly in type I and many type II patients with objective ductal dilation and/or enzyme elevation.
- In type II SOD, outcomes after EST correlate with objective evidence of obstruction or sphincter hypertension on SOM. Empiric sphincterotomy without manometry is controversial.
- Type III SOD has emerged as predominantly functional pain rather than a mechanical obstacle. Alternative management emphasizes risk stratification, noninvasive strategies, and multidisciplinary approaches.
- Medical and non-sphincterotomy options (calcium-channel blockers, nitrates, antidepressants, and lifestyle modifications) have been discussed as potential adjuncts or alternatives.
Summary
- SOD is a multifactorial biliary and pancreatic sphincter disorder with a spectrum from mechanical obstruction to pure dyskinesia. Type I and II retain treatment relevance, particularly EST for biliary obstruction. Type II management requires clear identification of the cause.
- SOM is a diagnostic tool with significant limitations.
- Endoscopic sphincterotomy offers meaningful symptom relief in type I and select type II with objective obstruction. It carries a risk of complications, including pancreatitis; risk mitigation strategies are integral to practice. In type III SOD, sphincterotomy generally has limited benefit, necessitating a move toward noninvasive management and careful patient counseling. Patients post- gastric bypass, or duodenal switch, can not have ERCP or SOM done.
Types of HyperParathyroidism
February 20, 2026 4:05 pm
There are 4 parathyroid glands which are located behind the thyroid gland, among other functions, are the main regulators of calcium, phosphorous, and magnesium in the blood. Elevations of parathyroid hormone (hyperparathyroidism) can be: 1-Primary, 2-Secondary, 3-Tertiary

Primary hyperparathyroidism means the parathyroid glands themselves are hyperactive. This may involve only one of the four glands: a) an adenoma, a benign tumor that needs surgical removal, or b) hyperplasia, when all 4 glands are hyperactive and/or enlarged, and in some cases, most of the 4 glands need to be removed.
Secondary hyperparathyroidism means that the elevated PTH level is caused by an external regulatory stimulus, such as low calcium, which itself may be due to low vitamin D, low calcium intake, or other causes.
Tertiary hyperparathyroidism is seen only in specific renal failure and transplant patients.
Regardless of the type of hyperparathyroidism, the end result is the same. Because the parathyroid gland aims to maintain normal calcium levels, it will do everything to achieve them. This includes increasing calcium absorption from the GI tract, breaking down bone to increase the blood calcium supply, and increasing calcium reabsorption from the urine.
Distinguishing between primary and secondary is critical, as primary is more likely than not a surgical problem that needs to be addressed. Secondly, it may be responding to metabolic deficiencies (low CA, low Vitamin D) that need to be corrected and take some time.
Not all cases require surgical intervention, as labs (vitamin D, calcium, and alkaline phosphatase) and imaging studies, such as neck ultrasound, CT scan, and Sestamibi scan, provide the information needed to dictate the treatment plan. Please stay up to date with your yearly lab results to catch changes sooner rather than later.
Bile Reflux Gastritis and Cholecystectomy
May 21, 2025 2:41 pm
Bile reflux gastritis is not a the result of the cholecystectomy but may be seen in a subset of patient with other confounding conditions. Bile is produced in the liver and stored in the gallbladder. In response to high fat and protein in the stomach, the gallbladder contracts to ” squeeze” the bile stored in the gallbladder into the small bowel to help absorb the fat and protein.

With the gallbladder removed, the bile produced by the liver cannot be stored and goes directly to the small bowel via the biliary tree.

It is possible and likely that some of the bile will find its way back to the stomach. In some patients, due to compounding circumstances, the bile may collect and cause gastritis. We need to dissect this a little for it to make sense.
- Not every patient after cholecystectomy will have bile in their stomach.
- Not every patient with bile in the stomach has gastritis.
To appreciate this, let’s remember that for bile to get from the small bowel to the stomach, it needs to:
- Go upstream, against the peristalsis of the small bowel, and do not be washed down by the flow of the gastric
- juices coming out of the stomach.
- Go through the pyloric valve.
- If it reaches the stomach, the acid in the stomach does not neutralize it, causing gastritis.

As I’m sure we all appreciate, other contributing factors besides cholecystectomy may cause bile reflux and bile reflux gastritis. This is why it’s also emphasized that bile in the stomach alone does not confirm biliary reflux gastritis. It is also why we always state that bile reflux gastritis is a disease of exclusion, where other conditions such as gastroparesis, acid reflux, and hiatal hernia (regardless of size, as some patients are unfortunately told that since the hernia is small it does not need to be fixed, which is incorrect) must be considered. Further information on Bile Reflux.
Billary Diversion is the only definitive surgical procedure for Bile Reflux Gastritis.
Staples Used in Gastrointestinal Surgery
February 11, 2025 11:23 am
I have frequently been asking what staples are used in sleeve gastrectomy. A stapling device is used with sleeve gastrectomy. This device comes in different shapes and sizes for different bowel thicknesses and applications. However, they all function the same way. The staple cartridges (the part of the stapler that is replaced after each use with a new one) are selected based on the thickness of the segment of the bowel that needs to be stapled and divided.
The stapling and dividing take place simultaneously. The sampler deploys six rows of staples and cuts between them, leaving three rows on one side and three on the opposite side. With the sleeve gastrectomy, this means that the sleeve stomach that is left has three rows of staples, and the segment of the stomach that is removed also has three rows of staples.

1-Can I have a CT or an MRI done? Yes, The titanium staples are safe for both CT and MRI.
2-What are they made from? The staples are made of titanium and alloys, which are non-reactive and safe.
3-How big are the staples? Different staples are of different sizes, mainly in the mm range; see the tip of the pencil in the image for the relative size.
Video of stapler demonstation here

Feeding Tube with Duodenal Switch
February 03, 2025 9:53 am
The surgical changes following the revision of the failed gastric bypass to the duodenal switch or a primary duodenal switch require an evident appreciation and understanding of the anatomy and physiology of placing a feeding tube and managing the nutritional status. There are different places where a feeding tube can be placed.
1-A feeding gastrostomy tube endoscopically cannot be placed because of the transected post-pyloric duodenum (The image viewed on a desktop or a laptop allows the scroller on the image to move)
2-An orogastric or nasogastric tube should only use an elemental feeding formula. This is because the food in the stomach is prevented from mixing with the biliopancreatic juices, which will not be adequately absorbed.
3-A feeding Jejunostomy can only be insured surgical post ligament of traits. This cannot be done endoscopically because duodenal switch transaction post pyloric small bowel to prevent mixing of the biliopancreatic secretion.
Additional informationVitamin Toxicity
December 17, 2024 1:36 pm
Patients are frequently asked to explain why they take high fat- or water-soluble vitamin doses. They are have often been scared by their well meaning healthcare providers that their higher levels of vitamin supplements will end up with vitamin toxicity.
Let’s clarify one point: there is such a thing as too much vitamin.
However, the point that is often overlooked in teaching within professional schools (medical, nursing, pharmacy, etc.) and drug manufacturers is that recommendations are based on “how much to take” and not how much is needed to keep a patient’s blood level in the normal range.

This table highlights how toxicity is described and what requirements are recommended. Vitamin toxicity is seen rarely in post-weight loss surgical patients who take them proactively in as many doses as needed to get their blood levels in the normal range. I see more patients in the office who suffer from low vitamin levels, such as vitamin D and A levels (duodenal switch and sleeve), than any patient with high or toxic levels of any vitamins.
Here is an example of critical vitamin A deficiency and night blindness and how, with aggressive large-dose supplementation, her condition was corrected.
A patient story: Lap Band complication and Wegovy
October 24, 2024 4:30 pm
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wegovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
- Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
- Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
- GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
- GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
- I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
- There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
- A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity

Radiology film of normal position and a slipped LapBand

SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
https://www.dssurgery.com/wp-content/uploads/2024/09/P000008S017b.pdf
https://www.dssurgery.com/wp-content/uploads/2024/09/20-year-all-procdure-metaanalysis.pdf
https://www.dssurgery.com/weight-loss-injection/
https://www.dssurgery.com/glp-1/
https://www.dssurgery.com/weight-loss-medications-compared-to-surgery/
https://www.dssurgery.com/articles/glp-1-agonists-a…agency-clinicians/
https://www.dssurgery.com/articles/managing-the-gas…clinical-practice/Should Adjustable Gastric Banding (Lap Band) be done?
October 06, 2024 9:17 pm
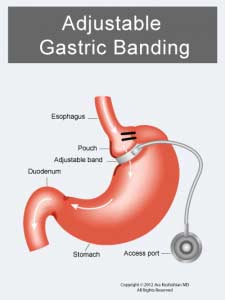

- The Lap Band does not result in long-term sustained weight loss.
- Lap band has significant complications, some of which may not be reversible.
- The lap band can be removed, but eroding the banc to the stomach is not easy.

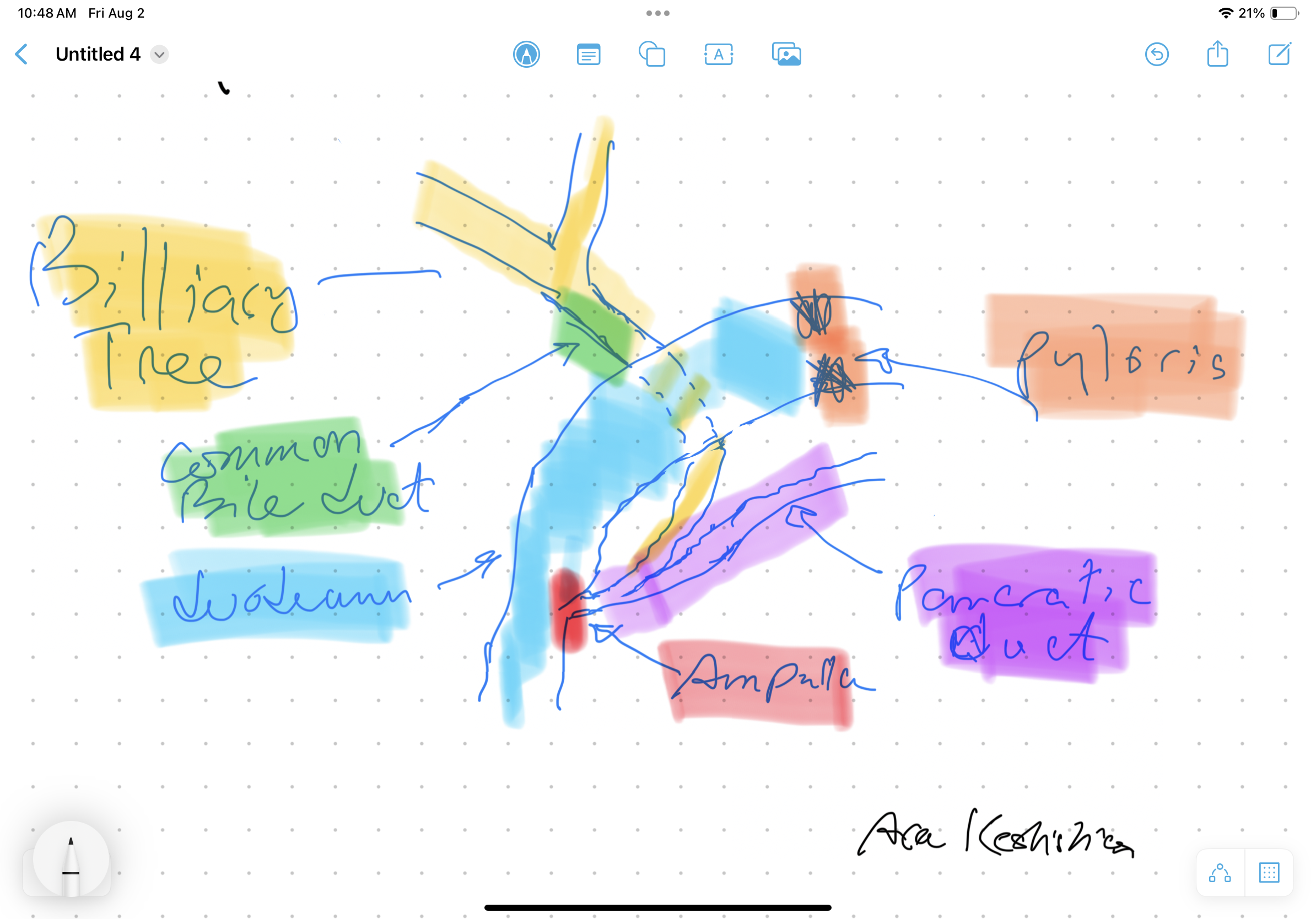
Bile Reflux Gastritis
August 02, 2024 10:53 am
Bile Reflux
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary tract flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or a tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis is reserved for cases with no alternatives.

SIPS-SADI and ASMBS
December 31, 2023 1:21 pm