Category: PTH
Types of HyperParathyroidism
February 20, 2026 4:05 pm
There are 4 parathyroid glands which are located behind the thyroid gland, among other functions, are the main regulators of calcium, phosphorous, and magnesium in the blood. Elevations of parathyroid hormone (hyperparathyroidism) can be: 1-Primary, 2-Secondary, 3-Tertiary

Primary hyperparathyroidism means the parathyroid glands themselves are hyperactive. This may involve only one of the four glands: a) an adenoma, a benign tumor that needs surgical removal, or b) hyperplasia, when all 4 glands are hyperactive and/or enlarged, and in some cases, most of the 4 glands need to be removed.
Secondary hyperparathyroidism means that the elevated PTH level is caused by an external regulatory stimulus, such as low calcium, which itself may be due to low vitamin D, low calcium intake, or other causes.
Tertiary hyperparathyroidism is seen only in specific renal failure and transplant patients.
Regardless of the type of hyperparathyroidism, the end result is the same. Because the parathyroid gland aims to maintain normal calcium levels, it will do everything to achieve them. This includes increasing calcium absorption from the GI tract, breaking down bone to increase the blood calcium supply, and increasing calcium reabsorption from the urine.
Distinguishing between primary and secondary is critical, as primary is more likely than not a surgical problem that needs to be addressed. Secondly, it may be responding to metabolic deficiencies (low CA, low Vitamin D) that need to be corrected and take some time.
Not all cases require surgical intervention, as labs (vitamin D, calcium, and alkaline phosphatase) and imaging studies, such as neck ultrasound, CT scan, and Sestamibi scan, provide the information needed to dictate the treatment plan. Please stay up to date with your yearly lab results to catch changes sooner rather than later.
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
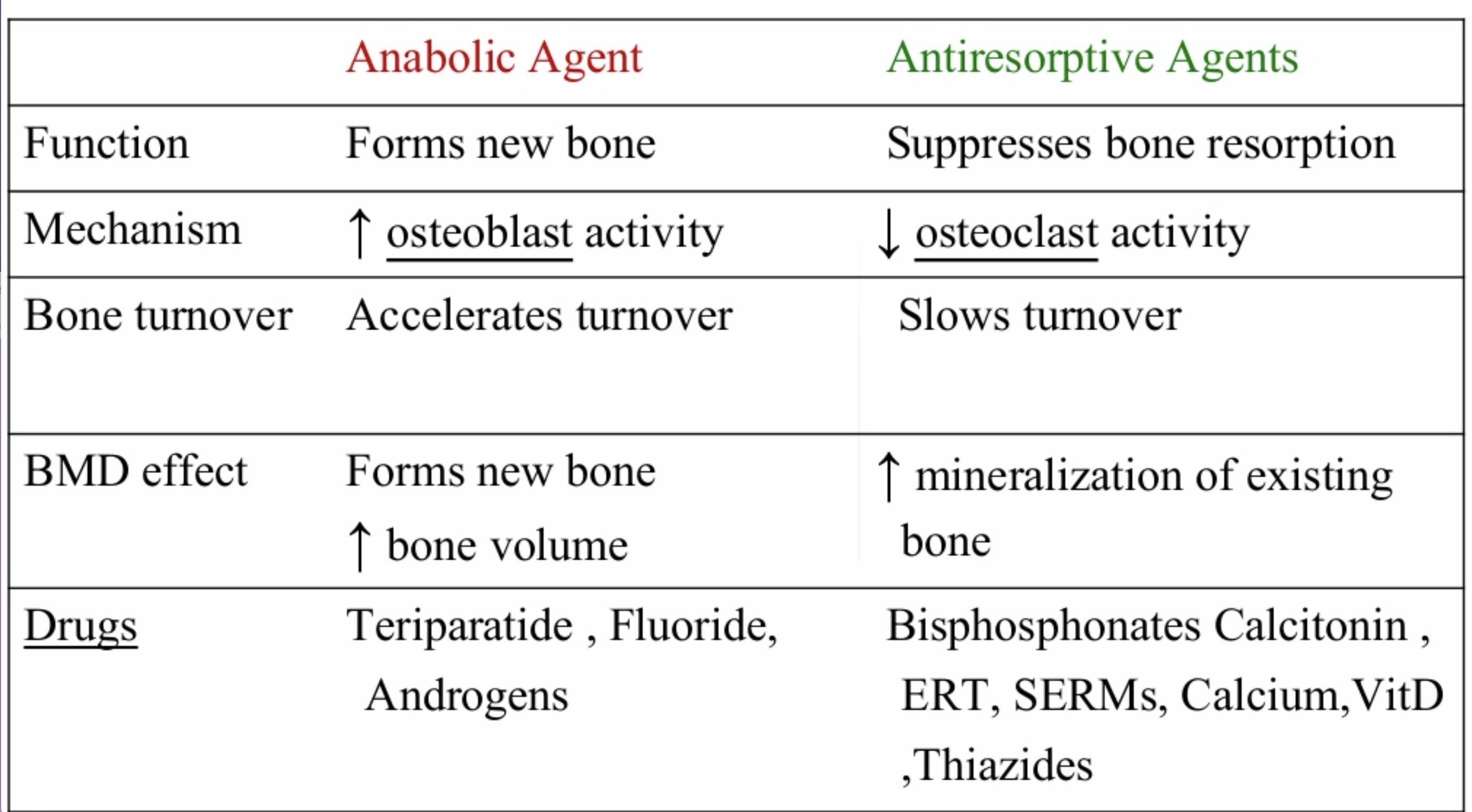
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
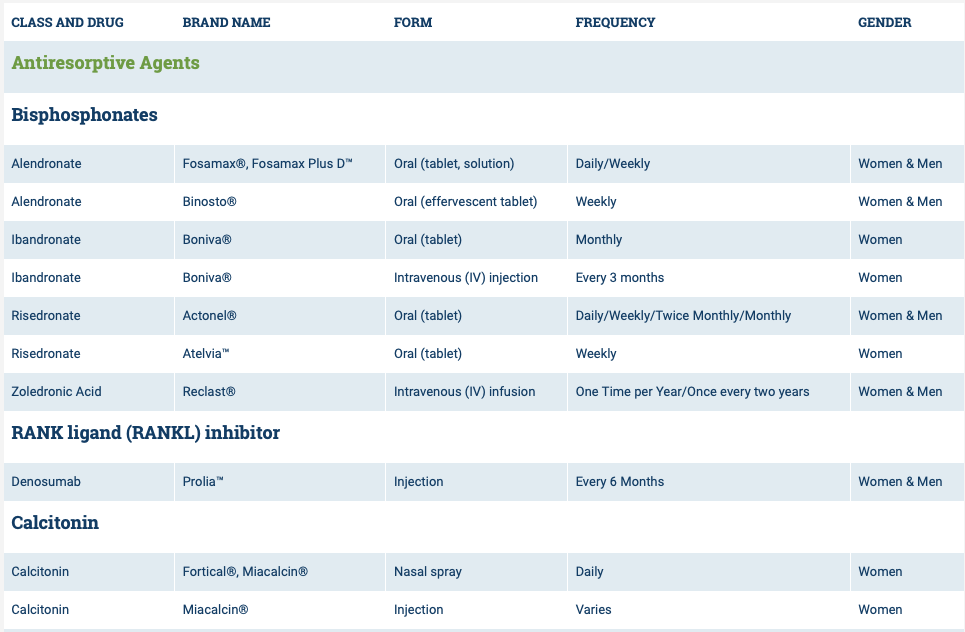
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

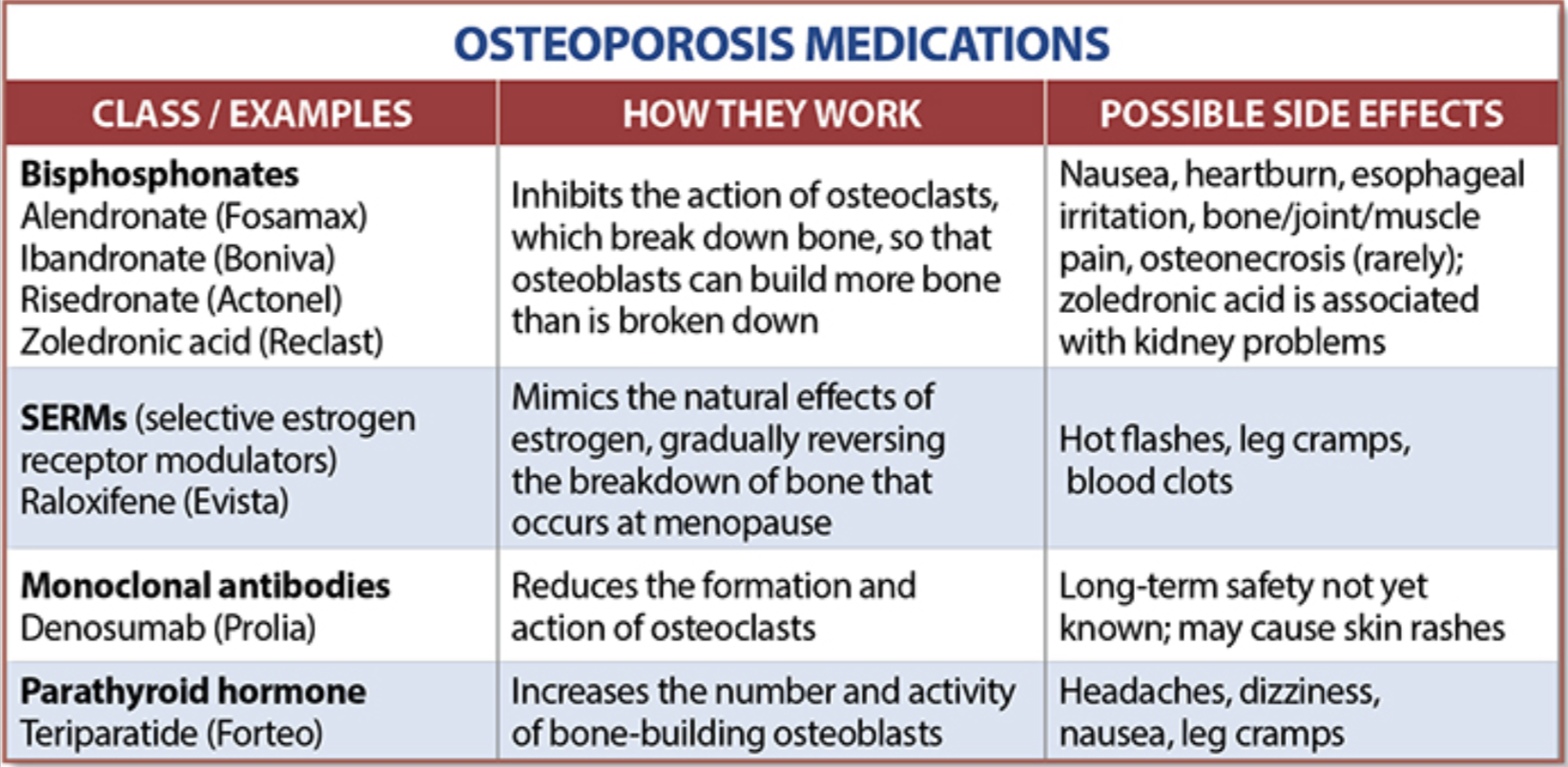
The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium
Magnesium Questions
May 11, 2016 6:07 am
Since our Webinar on Magnesium, I have received several Magnesium Questions recently regarding Magnesium deficiency. There is some evidence that calcium deficiency can not be corrected with an underlying magnesium deficiency. This may be due to the fact that magnesium is essential to converting Vitamin D to it’s active form and more information here. The active form of Vitamin D is needed to actively transport Calcium within the cell. This may be the confusion that calcium absorption needs magnesium. It is not needed directly but rather indirectly via Vitamin D.
Other cofactors needed in Vitamin D metabolism are:
Zinc (high doses antagonist with Magnesium and Copper)
Boron (raises Magnesium blood levels)
Vitamin K2
Vitamin A in small amounts
Further information regarding bone health and nutrients here.

Some important facts about Magnesium are:
- It is Absorbed in the distal Jejunum and Ileum (small intestines) and to some degree the colon.
- Plays an important role in Parathyroid Hormone synthesis which is also acted upon by Vitamin D
- Vitamin D increases Magnesium absorption
- All enzymes that metabolize Vitamin D require Magnesium
- Magnesium has a positive effect on Vitamin D deficiency.
- Magnesium and calcium are antagonist to each other on a cellular level (work against each other) They use an overlapping transport system for reabsorption within the kidneys and thereby compete with each other. Magnesium may also bind to calcium binding sites and intracellular protein binding sites due to their similarity.
- Calcium supplements can decrease Magnesium absorption.
- It Activates digestive enzymes for protein, fat and carbohydrate metabolism.
- Essential for protein synthesis
- Stores and moves energy acquired from digestion.
- Regulates Calcium via Vitamin D and increasing urinary excretion of calcium
Factors inhibiting Magnesium absorption:
- PPI
- Fiber
- Phytates
- Excessive unabsorbed fatty acids
- Calcium
- Phosphorus
- Protein

In summary, post Bariatric patients are at risk for magnesium deficiency and it plays an important role in overall health and bone health. Our practice recommends Magnesium Glycinate as the form for supplementation in at least a 2:1 ration with calcium. An example is: Calcium 2000mg daily to Magnesium Glycinate 1000mg daily. (Supplement based on your laboratory studies) We hope that this blog has answered some of your Magnesium Questions.
Hyperparathyroidism and Weight Loss Surgery
March 13, 2015 5:57 pm
Hypoparathyroidism refers to elevated level of parathyroid hormone levels (elevated or high PTH). Parathyroid glands are two small glands that are located behind the thyroid gland. The primary function is regulation of the calcium level in the bloodstream. Parathyroid levels may be abnormally elevated for a number of reasons.
1-Primary Hyperparathyroidism
There may be abnormalities within the parathyroid glands themselves including benign and malignant tumors. Laboratory studies to assist in identifying Parathyroid hyperplasia are calcium, phosphorus, magnesium, PTH (parathyroid hormone), Vitamin D and possibly a 24 hour urine, kidney x-ray, and Dexa scan. The calcium levels in parathyroid hyperplasia are usually elevated and Vitamin D levels low. Patients can present with hypercalcemia symptoms such as kidney stones, nausea, vomiting, peptic ulcer, constipation, bone pain, bone weakness, depression, lethargy, fatigue. There are two types of Primary Hyperparathyroidism parathyroid hyperplasia and parathyroid adenomas. These both can at times be genetically linked.
Once the cause of elevated parathyroid hormone has been identified as primary hyperparathyroidism, the treatment involves surgical removal of one or more of the adenoma(s) or removal of 3.5 off all of the parathyroid glands if hyperplasia is diagnosed.
Parathyroid hyperplasia: When the growth involves all 4 of the glands. These may effect either one of the glands or all 4 of them. Majority of these are benign.
Parathyroid adenoma(s) refers to the abnormality or benign growth of one or more of the parathyroid glands.
2- Secondary Hyperparathyroidism
This is probably the most common cause of hyperparathyroidism imposed on a weight loss surgical patient. The elevated parathyroid hormone is the physiologic response all of the parathyroid glands to low calcium level. The parathyroid hormone is elevated in order to favor bone breakdown and make available for calcium to be circulating in the bloodstream. Parathyroid hormone also facilitates reabsorption of the calcium from the urine and improve absorption of the calcium from the GI tract.
The most common causes of secondary hyperparathyroidism is Vitamin D deficiency, weight loss surgery, kidney failure, Celiac or Crohn’s Disease. Lower levels of Vitamin D decrease the intestinal calcium absorption and thereby increasing PTH secretion. Vitamin D is the transport molecule for calcium. Symptoms may include bone or joint pain, muscle weakness, osteomalacia, low to normal blood calcium levels. The treatment of secondary hyperparathyroidism is correction of the underlying low calcium, low vitamin D levels. We have our Duodenal Switch patients take calcium citrate and dry water miscible type of Vitamin D3. Some people may require vitamin D injection in order to overcome deficiencies. You can find a list of supplements on our website and/or our starting point supplement recommendation in our patient workbook

Articles on Secondary Hyperparathyroidism following Weight Loss Surgery:
https://www.ncbi.nlm.nih.gov/pubmed/23015268
https://www.ncbi.nlm.nih.gov/pubmed/16354517