Category: revision of Duodenal Switch
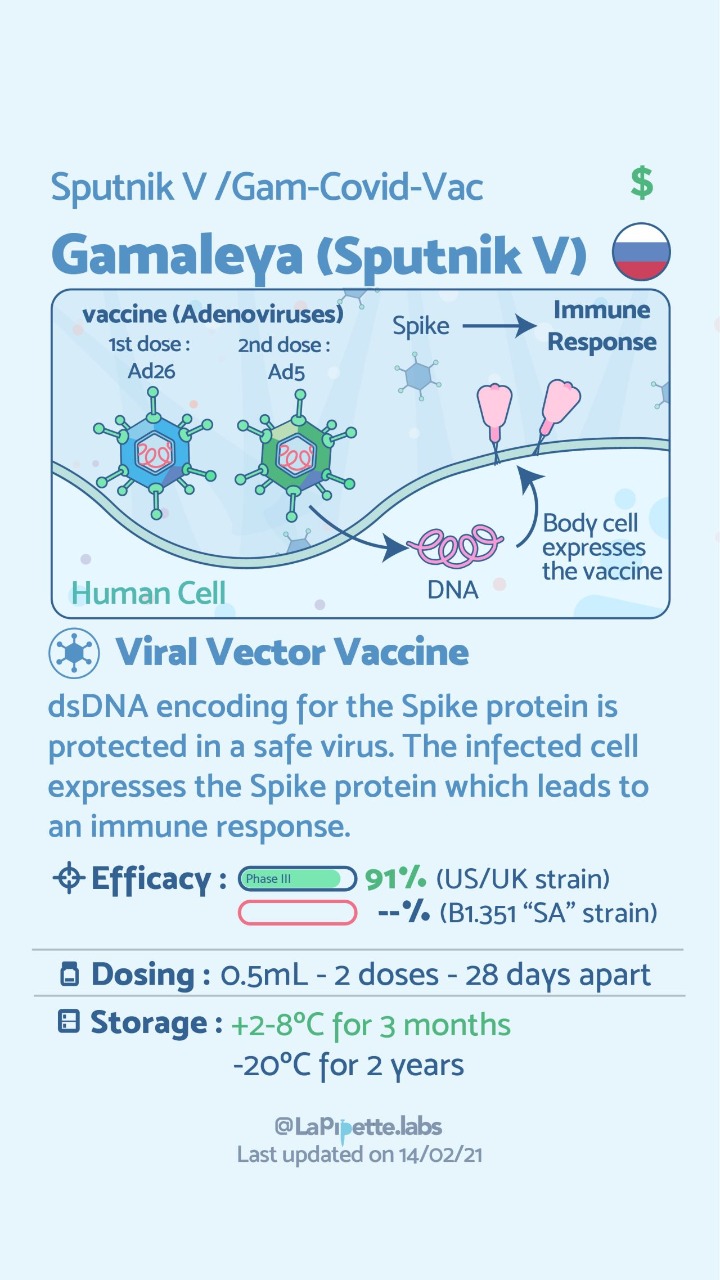
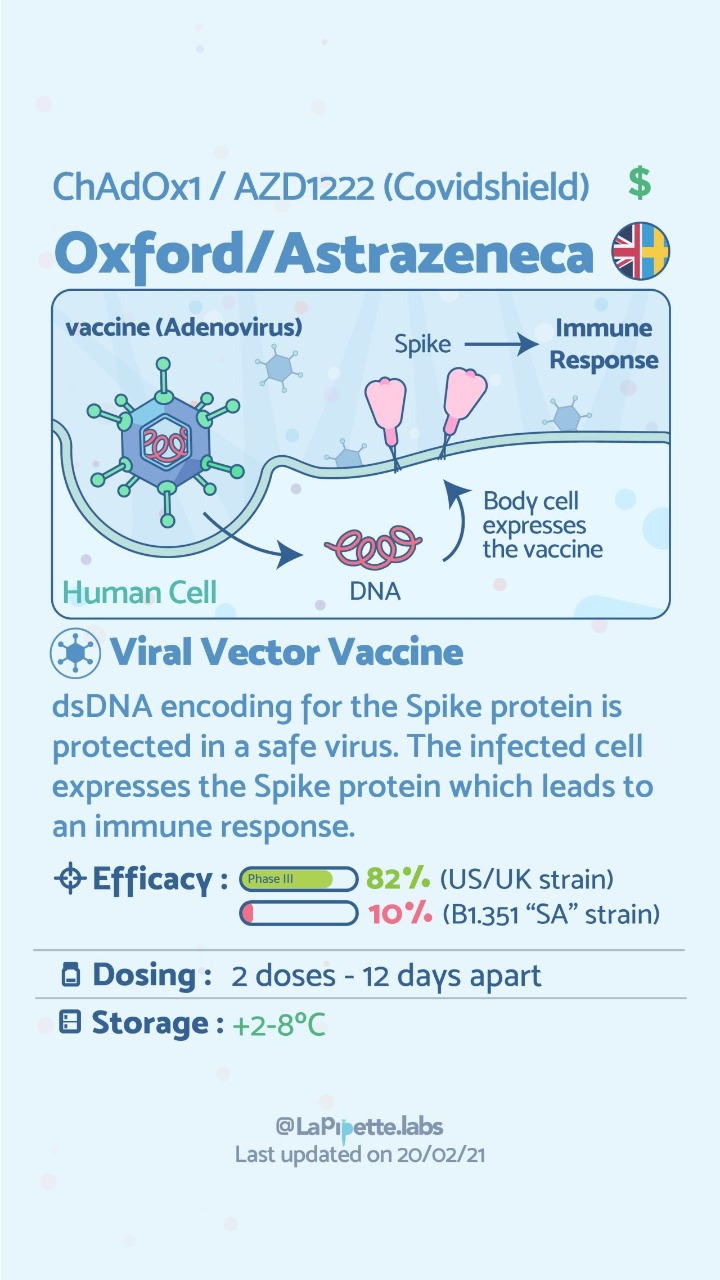
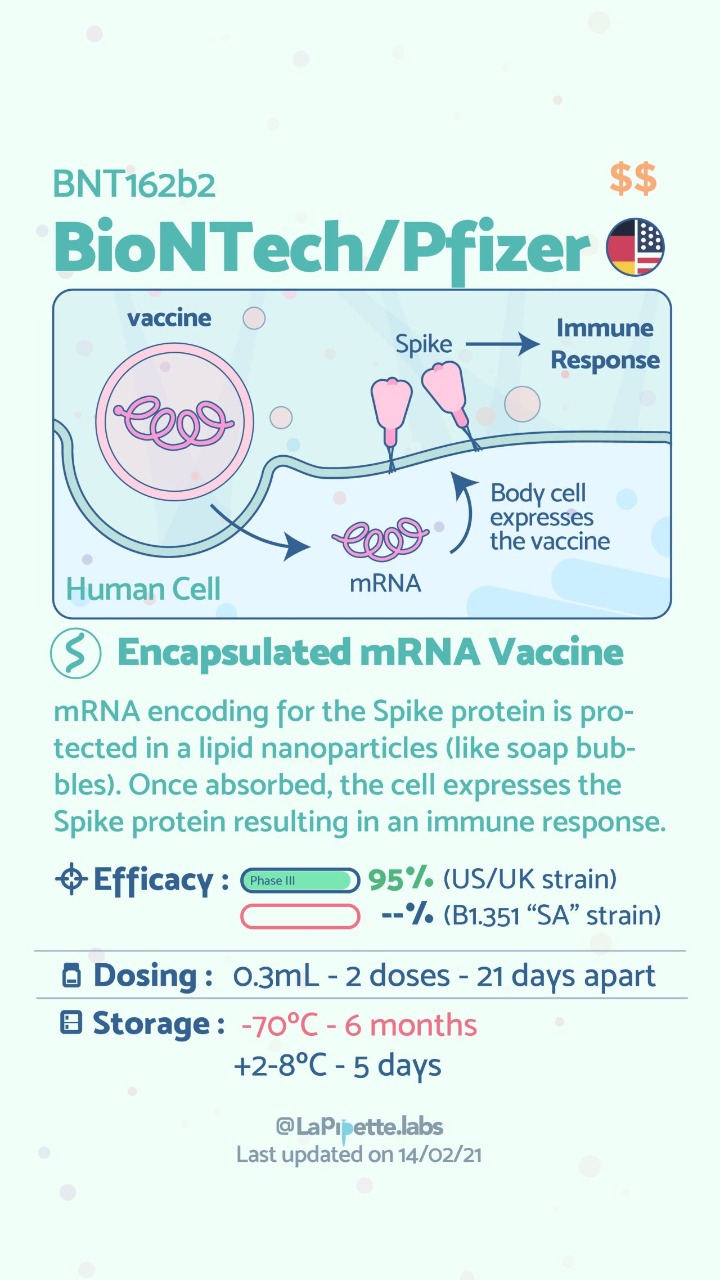
COVID Vaccines
March 05, 2021 3:50 pm
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
Stapled Anastomosis
December 30, 2019 11:23 am
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
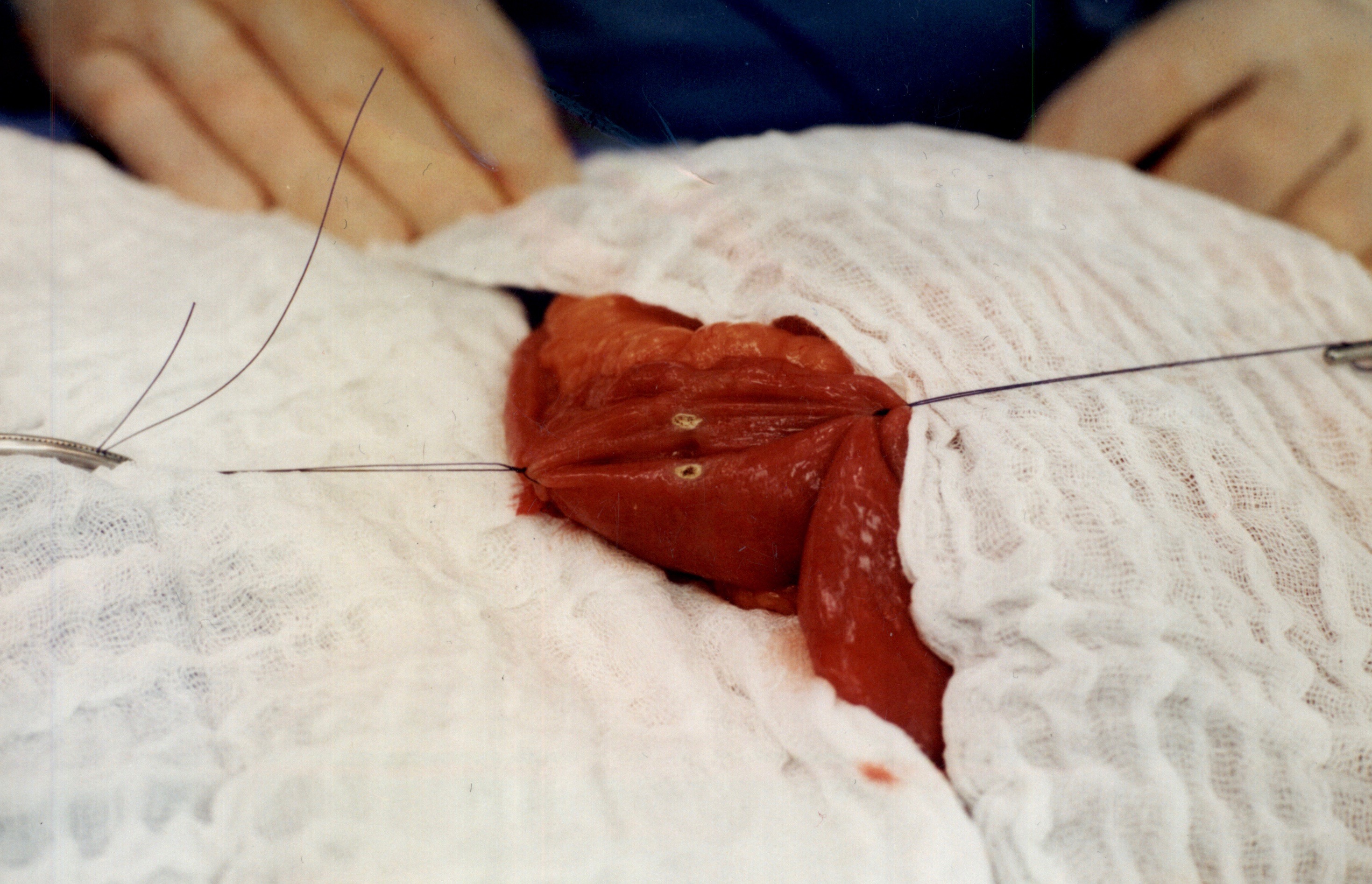
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
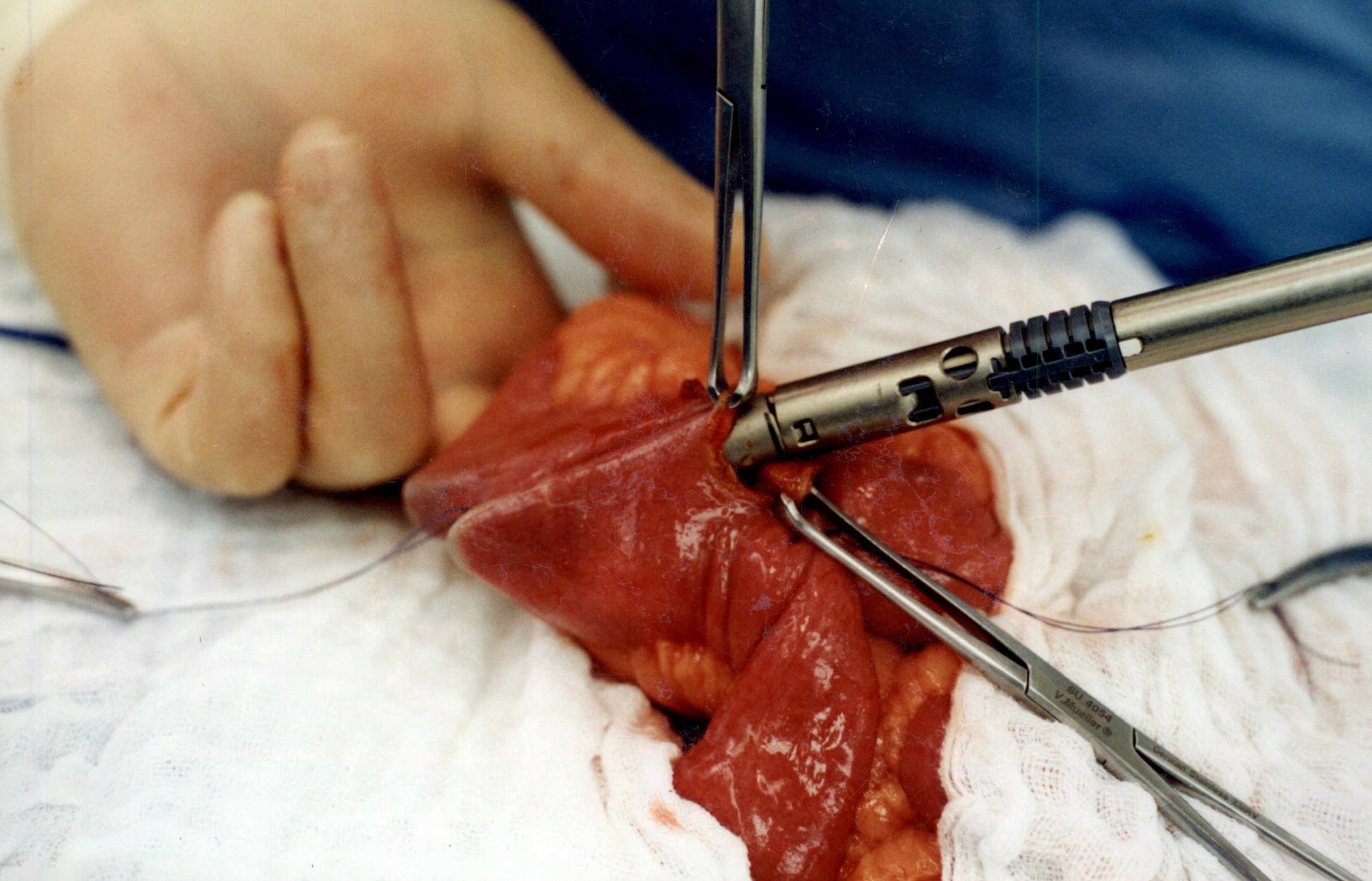
When the stapler is fired in opposite direction, a very wide anastomosis is created.
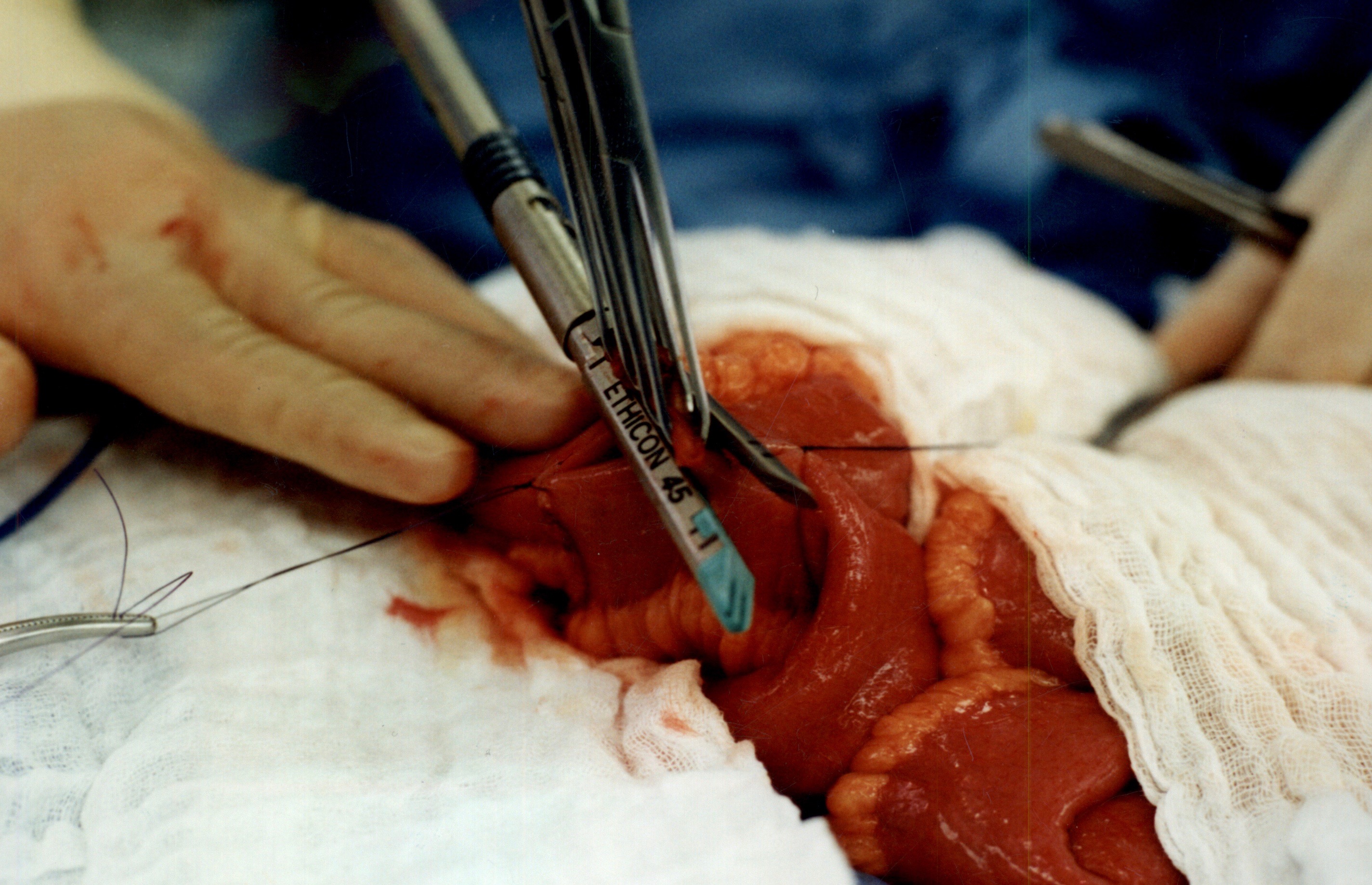
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Dr. Facebook
March 22, 2019 8:24 am
We have become reliant on the information that we obtain from the internet, specifically platforms such as Facebook. In our practice we have to continuously correct information that patients have obtained from other patients, unmonitored sites, blogs, and postings. Most of this information is based on individual experiences that has become gospel. “Fat is good for you” is one of them. To clarify, some health fat (olive oil, avocado, Omega 3) is healthy and needed for all patients. We do not recommend “fat bombs” as a part of ones daily dietary intake.
The following article was written on the accuracy of nutritional posts in support groups on Facebook.
Koalall et. all in SAORD, December 2018 Volume 14, Issue 12, Pages 1897–1902 published
“Content and accuracy of nutrition-related posts in bariatric surgery Facebook support groups”
The conclusion, as suspected, that “Over half of the posts contained inaccurate content or information that was too ambiguous to determine accuracy..:”

It is our recommendation before any dietary recommendations are taken from facebook and the like, the source of the information should be verified. As I have stated in the past, a frequent flier passenger is probably not qualified to fly a
commercial airplane, any more than a previous weight loss surgical patient providing medical and nutritional advice. We realize that there is significant value to the forum for exchange of information and sharing of experiences with other weight loss surgical patients as long as the information is well sourced and verified.

Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP
PolyCystic Ovarian Syndrome PCOS
September 04, 2018 9:58 am
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.

Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
Bariatric Surgery can improve PCOS in those individuals with Type 2 Diabetes Mellitus. Further information on weight loss surgery and its effect on PCOS here.
Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

New Pasadena Office Map and Parking
August 12, 2017 8:35 am
We’ve created a helpful map and parking diagram for our new Pasadena, CA office location. It also has a general layout of the Huntington Memorial Hospital Campus and Pre-operative intake and testing area. We hope that you find it helpful on your next visit to see Dr. Ara Keshishian, General and Bariatric Surgeon.

Dr. Ara Keshishian has performed more than 2,000 Duodenal Switch procedures, thousands of Sleeve Gastrectomies and more than 500 revisions from other Weight Loss Surgeries such as RNY Gastric Bypass, Adjustable Gastric Band, and Sleeve Gastrectomy to Duodenal Switch as well as General Surgical cases over the last 18 years of private practice.
Review & Update Giveaway!
August 31, 2016 6:27 pm


The Prize winners are Jo and Kimberly! Congratulations ladies and enjoy the Obesity Help National Conference! Thank you to all that participated in the Giveaway!
We are holding a review and update giveaway for two different prizes! Thank you for your
participation!
One Prize and One Grand Prize
Prize: two tickets to Obestiy Help National Conference Sept. 30-Oct 1, 2016
Grand Prize: two tickets to Obesity Help National Conference and one night
hotel stay October 1, 2016
Conference: 11999 Harbor Boulevard Garden Grove, California 92840 Event link here
Hotel Prize: SHERATON GARDEN GROVE – ANAHEIM SOUTH HOTEL
12221 Harbor Boulevard
Garden Grove, California
Official Rules:
How to Enter and eligibility: All entrants and winners must be 18 years of age or older at the time of entry. Up to 5 entries per person.
- Write a review of Dr. Ara Keshishian on one or all of the sites below or do an update on your profile on Obesity Help between now and Sept. 8, 2016 at 5:00 PM
2. Take a screen shot of the review or update with your username and date.
3. E-mail the screenshot to [email protected] with your contact information (name, phone number, e-mail, and mailing address )
4. Entries must be a verifiable patient of Dr. Ara Keshishian in Glendale, CA.
Promotion Timing:
The Review & Update Giveaway begins September 1, 2016 and ends September 8, 2016 at 5:00pm PST
How Winners are Chosen:
Winners will be chosen by random draw. Odds of winning vary upon the number of entries received for the giveaway.
Winner Notification and the Claiming of Prizes:
Winners will be notified via the email provided at time of entry and also published on our blog comments www.dssurgery.com/blog and on our FaceBook page. The winner will have 72 hours to respond to the winning notification email or the prize will be forfeited. The prizes have no cash value. The prizes are non-transferable and must be accepted as awarded. No changes may be made to the prizes. There is no cash value for the prizes.
General Conditions:
By entering the Giveaway, entrants agree to abide by and be bound by these Official Rules and the decisions of the Sponsor, which are final and binding in all matters relating to the Giveaway, and release and hold harmless Sponsor and its affiliates, directors, officers, employees and assigns from and against any liability, claims, lawsuits, judgments, losses, damages of any kind, injuries, death, property damage, costs and expenses, arising from, resulting from or in connection with the Giveaway, the participation in the Giveaway, or the receipt, possession, use or misuse of any prize. Sponsor is not responsible for lost, late, incomplete, inaccurate, stolen, delayed, misdirected, undelivered or illegible entries or for lost or stolen entry boxes or other errors or difficulties of any kind whether human, mechanical, electronic, typographical, printing or otherwise relating to or in connection with the Giveaway, including, without limitation, errors or difficulties which may occur in connection with the administration of the Giveaway, the processing of entries, the announcement of the prizes, or in any Giveaway-related materials. Sponsor is not responsible for technical, hardware, software or telephone malfunctions of any kind, lost or unavailable network connections, or failed, incorrect, incomplete, inaccurate, garbled or delayed electronic communications caused by the user or by any of the equipment or programming associated with or utilized in the Giveaway. Persons who tamper with or abuse any aspect of the Giveaway or who are in violation of these Official Rules, as solely determined by Sponsor, will be disqualified and all associated entries will be void. The Sponsor reserves the right, at its sole discretion, to cancel, terminate, modify or suspend the Giveaway if, in Sponsor’s opinion, it is not capable of running as planned, including, but not limited to, due to tampering, unauthorized intervention, fraud, technical or phone line failures or any other problems beyond the control of the Sponsor, and select the winners for affected drawing(s) from among all eligible entries timely received for such affected drawing(s) prior to cancellation.
Inadequate Weight loss and Weight Regain
May 24, 2016 7:56 am
There were numerous causes for the inadequate weight loss and or weight regain after weight loss surgery.
These factors may include:
1-Type of the surgery: Duodenal Switch, RNY, Adjustable Gastric Banding, Intragastric Balloon, etc.
2-Patients metabolic state (age, activity level, hormones state etc)
3-Co-morbidities
4-Patient compliance
5-Other
Each and every one of these may be an independent factor or may be a contributing cause.
In our experience, patients non-compliance is not as common as others believe. Frequently, we see patients in our office where they have been told that the poor outcome of the surgery is “their fault”
We see this with RNY, and Band patients as well as some of the duodenal switch patients who are seeking advice for weight regain or inadequate weight loss.
I would like to talk about the issues of inadequate weight loss or regain post Duodenal Switch specifically. Duodenal switch operation as described by Dr. Hess, outlined the division of the small bowel lengths to be proportional to each and every patients own total bowel lengths. This meant that two patients with the same BMI and weight will end up with two different lengths for common and alimentary limbs if there total length of the bowel is different. Unfortunately, too often patients are given a “standard” or “set” ( not clear what that word means, since there is no established standard in the literature) length for common channels and alimentary channels regardless of the total small bowel length. In some patients, those lengths may result in acceptable weight loss. However, quite frequently a patient with a preselected length for the common and alimentary limbs will end up either loosing too much weight and have nutritional problems or not loose adequate weight. As with all practices, we have over the years had patients who have had nutritional deficiencies and excessive weight loss or have had inadequate weight loss. Looking at the raw numbers however, we have had more patient from other practices that have come to us for revisions and corrections of lengths of the bowel lengths from other practices that our own patients have required.
Another level of the confusion is the improper interchanging of the “SIPS and SADI” procedures with the duodenal switch operation. As I have said in the past repeatedly, SIPS and SAID are not the same as the duodenal switch- and attempt to call these different procedures the same is misleading to say the least.
The other category of weight regain or inadequate weight loss includes medications and new health issues. Discussed in a previous blog, there are many medications that can influence weight gain. It is important to work with your health care provider to find medications that have a positive effect on symptoms without added side effects whenever possible.
In summary, weight re-gain or inadequate weight loss can have many facets. However, surgical technique can provide an advantage. Each aspect should be addressed and identified.