Category: Weight loss surgery. duodenal switch
Vitamin D level and Liver Function Test (LFT) elevation
February 08, 2026 11:21 am
After weight-loss surgery, some patients may experience a transient elevation in liver function tests that resolves over time. We have previously reported on this. IT is essential to distinguish between the Duodenal switch and the SIPS/SADI procedure, where some patients are led to believe they are identical. These procedures differ physiologically, and their weight loss and metabolic behaviours vary significantly.
Other than the stress of the weight loss, obesity, and comorbidities of obesity, there may be other anatomical post-surgical causes for elevated liver function test. This has also been discussed extensively.
A recent literature review supports the protective effects of vitamin D supplementation.
Elevated liver enzymes may be caused by many factors, including nutritional deficiencies, excessive supplementation (turmeric), medications, alcohol, adhesions causing partial bowel obstruction, and increased enterohepatic bile reabsorption . I would be very cautious about associating vitamin D supplementation with elevated liver function test results, even if the vitamin D level is in the very high normal range, regardless of the daily dose (much less frequent with injectable).
Vitamin D, as a fat-soluble vitamin, however, protects the liver and improves liver function test even in very high serum level . In rare cases, prolonged, elevated vitamin D levels may strain the liver. In Fact, the association of the vitamin D level and liver disease, including cirrhosis, leads to hepatocellular carcinoma (HCC) and dea h. Vitamin D protects the liver from HCC but cannot reduce the risk of cirrhosis.
Vitamin Toxicity
December 17, 2024 1:36 pm
Patients are frequently asked to explain why they take high fat- or water-soluble vitamin doses. They are have often been scared by their well meaning healthcare providers that their higher levels of vitamin supplements will end up with vitamin toxicity.
Let’s clarify one point: there is such a thing as too much vitamin.
However, the point that is often overlooked in teaching within professional schools (medical, nursing, pharmacy, etc.) and drug manufacturers is that recommendations are based on “how much to take” and not how much is needed to keep a patient’s blood level in the normal range.

This table highlights how toxicity is described and what requirements are recommended. Vitamin toxicity is seen rarely in post-weight loss surgical patients who take them proactively in as many doses as needed to get their blood levels in the normal range. I see more patients in the office who suffer from low vitamin levels, such as vitamin D and A levels (duodenal switch and sleeve), than any patient with high or toxic levels of any vitamins.
Here is an example of critical vitamin A deficiency and night blindness and how, with aggressive large-dose supplementation, her condition was corrected.
A patient story: Lap Band complication and Wegovy
October 24, 2024 4:30 pm
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wegovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
- Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
- Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
- GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
- GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
- I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
- There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
- A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity

Radiology film of normal position and a slipped LapBand

SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
https://www.dssurgery.com/wp-content/uploads/2024/09/P000008S017b.pdf
https://www.dssurgery.com/wp-content/uploads/2024/09/20-year-all-procdure-metaanalysis.pdf
https://www.dssurgery.com/weight-loss-injection/
https://www.dssurgery.com/glp-1/
https://www.dssurgery.com/weight-loss-medications-compared-to-surgery/
https://www.dssurgery.com/articles/glp-1-agonists-a…agency-clinicians/
https://www.dssurgery.com/articles/managing-the-gas…clinical-practice/SIPS-SADI and ASMBS
December 31, 2023 1:21 pm
Weight Loss Injection
May 10, 2023 1:06 pm
Semaglutide (Ozempic, Rybelsus, Wegovy, Saxenda) and tripeptide (Mounjaro) treat type II diabetes. They work thru several complex pathways. An observed side effect that has been noted in diabetic patients has been weight loss.
Some have been advocating using the class of medications for weight loss. However, Wegovy is the only medication approved for weight loss in non-diabetic patients.
There is a lot to be discussed here:
1-the use of the medications for weight loss is an off-label use (except Wegovy)- meaning that the FDA did not approve the medication as a weight loss drug.
The practical implication is that the medication’s safety and complication profile in non-diabetic patients looking to lose weight may be unknown and has not been studied.
2-The medication has become available thru compounding pharmacies. It is crucial to appreciate that compounding medications do not meet the same rigor and standards and may, in fact, not be the same formula as the FDA has stated.. This also means that a compounding pharmacy does not approve the medications in several states.
3-The most critical issue for me is the lack of a “long-term plan.” It is not clear what would happen when the patient stopped the medication. Will the patient experience weight regain? Will the patient require higher doses of the medication to maintain the weight loss, or will the medication stop working altogether? Unfortunately, we do not have these answers. For those skeptical about my questions, let me remind you that phentermine has significant side effects, and almost all patients experience weight gain when they have to stop the medication because of the cardiovascular complication of medication.
Vitamin D Metabolism and Deficiency file
March 28, 2020 8:17 am
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
In some cases, patients may need injectable Vitamin A or D to improve vitamin levels.
Click the links to view the information below and within the comments of this file:
Vitamin D3 50 by Biotech: Amazon
directly from BioTech:
Many DS surgeon’s do not recommend Children’s vitamins or chewable vitamins unless there is a specific reason or need for them.
DS Surgeon Blog on Vitamin D:
Webinar on Vitamin D metabolism:
Medications that effect Bone health:
This does not constitute medical advice, diagnosis or prescribing. It is simply a compiled list of gathered information. If you are in doubt or have questions please contact your medical healthcare professional.
Length of Bowel : Hess or No Hess
March 22, 2020 5:58 pm
“…What is the length of my common channel” is probably one of the frequently asked questions about the duodenal switch operation in the office. This usually comes up at the initial consult when patients repost credible sources such as Dr. Google and Dr. Facebook for patient with different bowel length have done well or not so after duodenal switch operation. Dr. Hess described the Duodenal Switch by using total bowel length measurements and creating the common channel as a percentage of the total small bowel length. However, it seems that this is being done less and less.
This leads to my explanation that is on the website
Hess calculator : Bowel Length Calculator
How the actual measurements matters: Bowel length video link
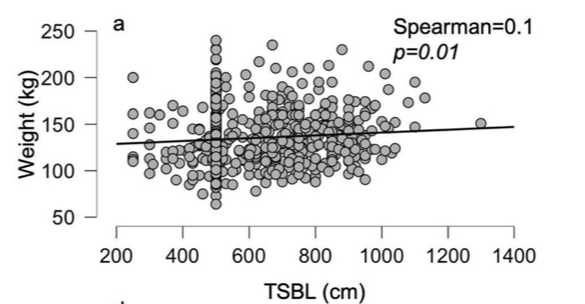
In 2019, Bekheit et.al published a very interesting study comparing total small bowel length (TSBL) to a number of variables such as height, weight, sex and BMI. They identified a few loose correlations. Male patient have longer TBSL than females. There was correlation between TSBL and height stronger in males than females but not statistically significant.
In Conclusion they reported ” Despite statistical significance of the correlation between the TSBL and the height and weight of the included participants, the correlation seems to have no clinical meaning since the effect size is negligible. ”
As I have previously discussed this Making the common and alimentary length standard for every duodenal switch patient will make some loose too much and other not enough weight.
Figure 1 shows TSBL on the horizontal axis, and height, weight, BMI and Age on the vertical axis. For the most part what they all show is that one can not predict how long a patients bowel is by any of the measures that we take in the office as a part of the routine exam.
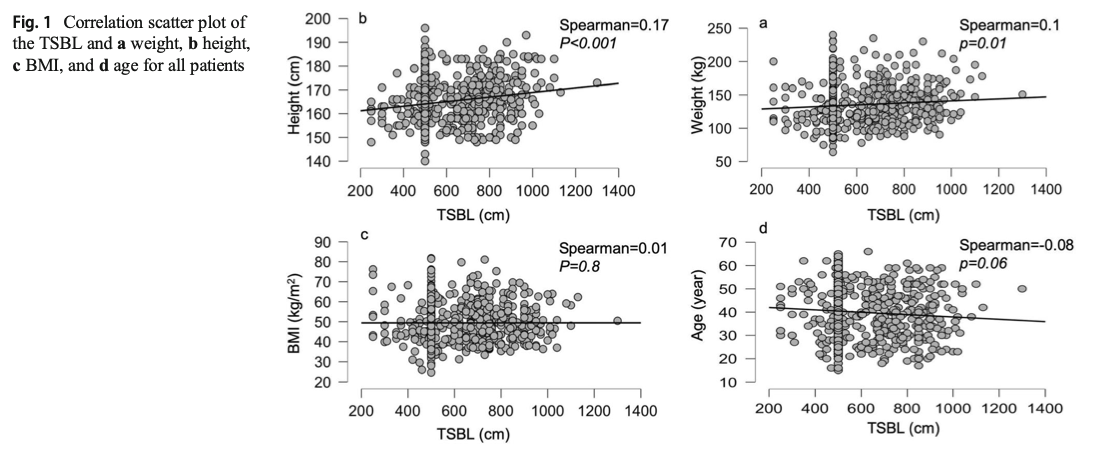
This raises, the concerns that I had raised previously. How could two similar patients who have the same weight, age, sex and BMI have the same surgery and expect the same result if one of them has TSBL of 400 cm and the other one 800cm?
Stapled Anastomosis
December 30, 2019 11:23 am
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
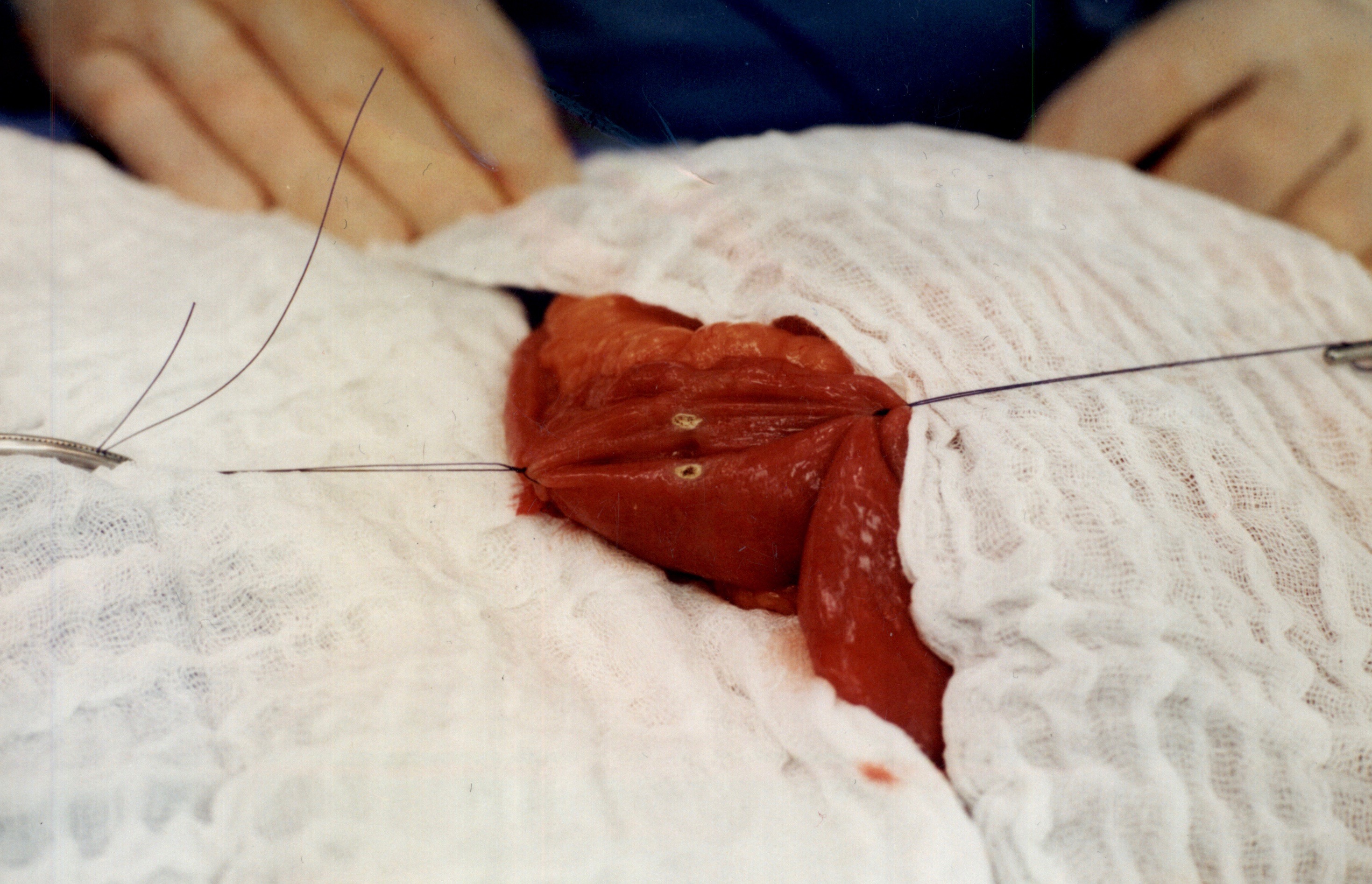
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
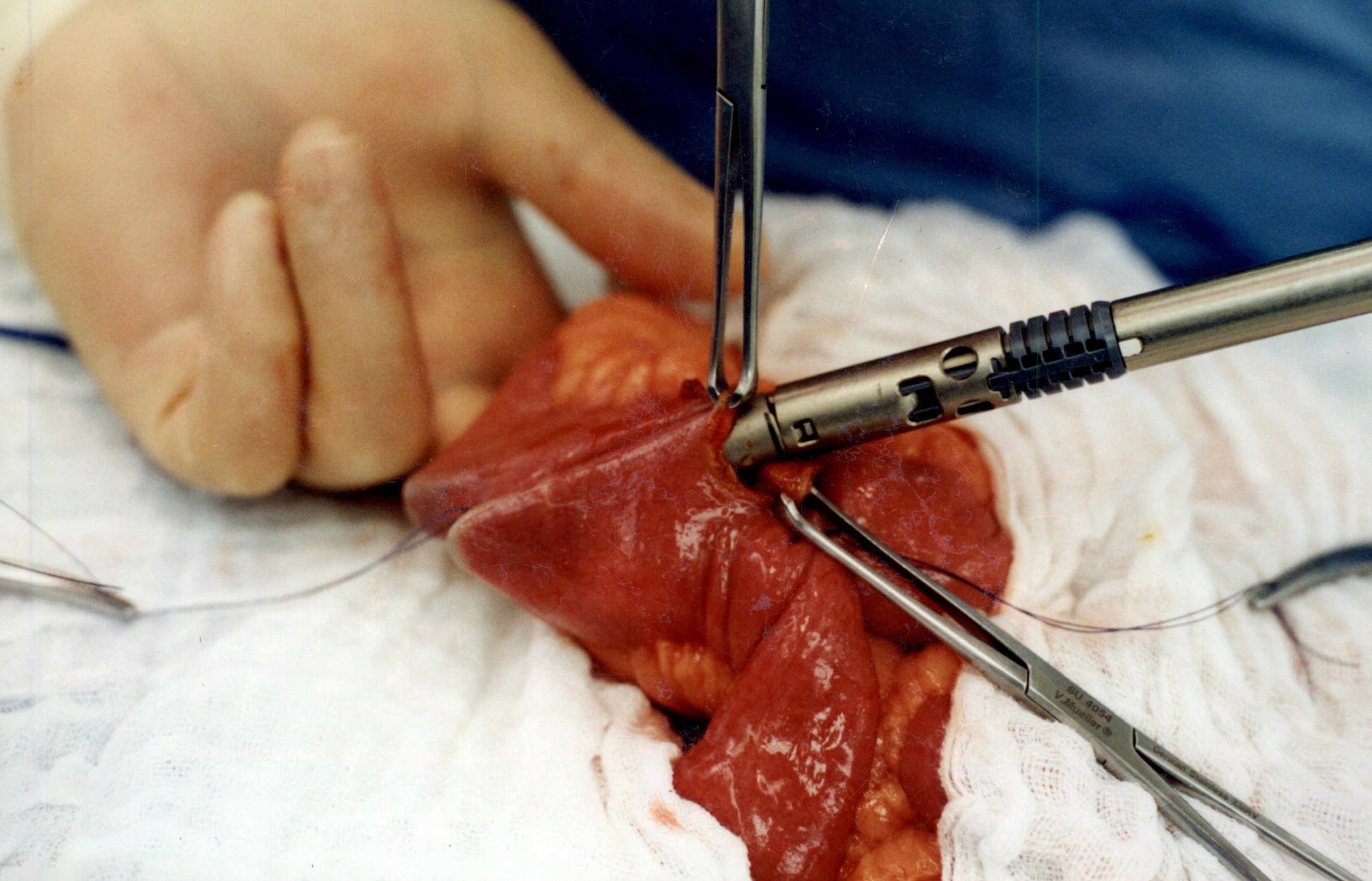
When the stapler is fired in opposite direction, a very wide anastomosis is created.
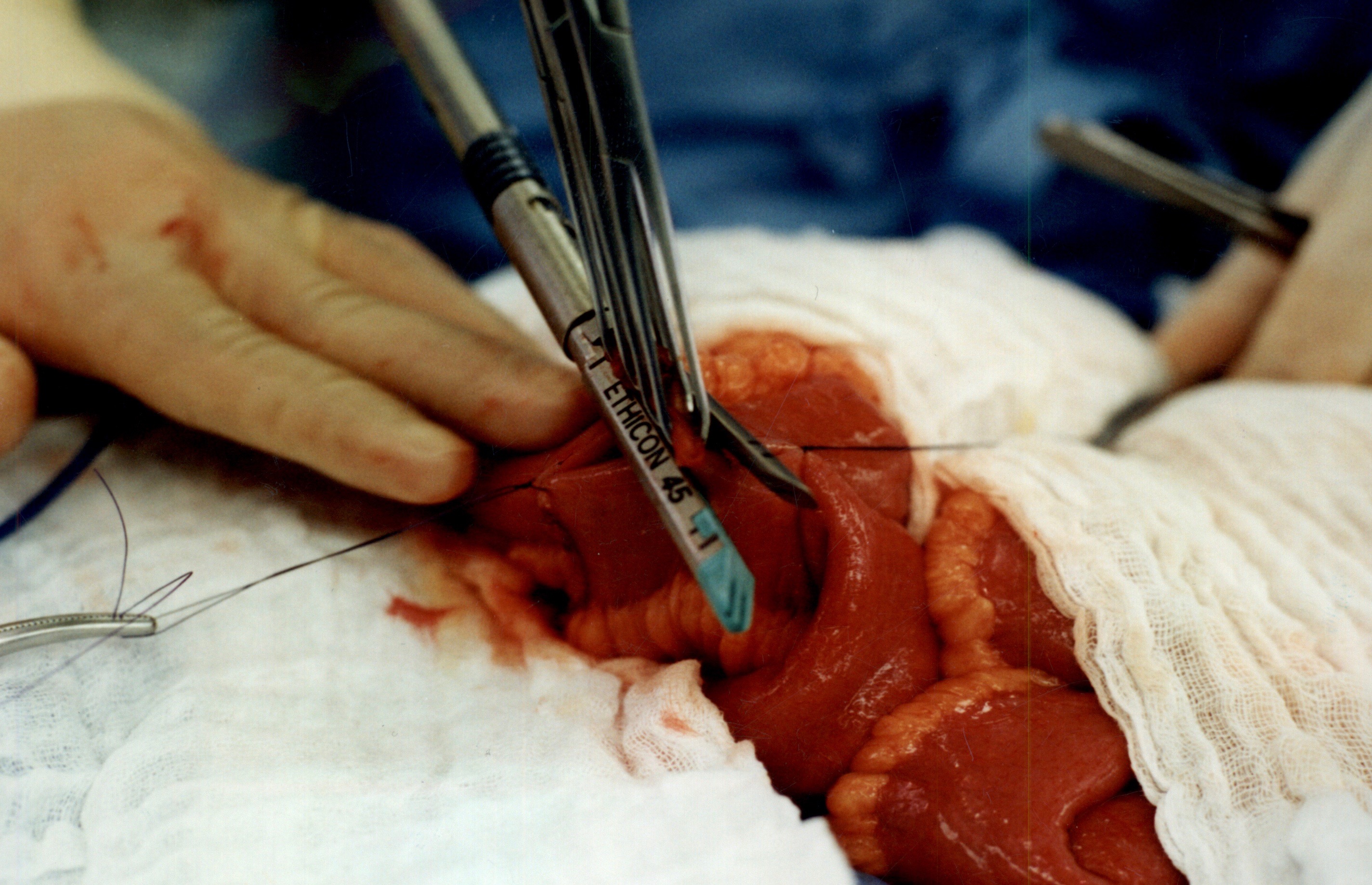
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Vitamin A, Absorption, and Wound Healing
September 25, 2019 8:39 am
Vitamin A is one of the 4 fat soluble vitamins along with vitamin D, Vitamin E and Vitamin K. It is multifunctional and essential which means that it is not produced by the body. In this article we will touch on aspects of Vitamin A absorption and it’s effect on wound healing as well as its metabolism.
We often think of Vitamin A as the critical vitamin for vision, however it has several other roles that related to immune function, protein synthesis, and cellular communication. Vitamin A deficiency is a concern world wide because of the natural of the side effects. Vitamin A deficiency is the leading cause of preventable childhood blindness in the world according to UNICEF and sometimes it may be undetected until there is irreversible damage.
There are 2 chemical forms of vitamin A in diet:
Retinoids (Preformed vitamin A) This group include retinol, retinyl esters, and retinal they are mostly found in animal sources like liver, egg yolk or fish oils.
Carotenoids (Provitamin A) This group includes beta-carotene, alpha-carotene and lycopene, mainly found in plant sources like leafy vegetables or yellow/orange vegetables and fruits.
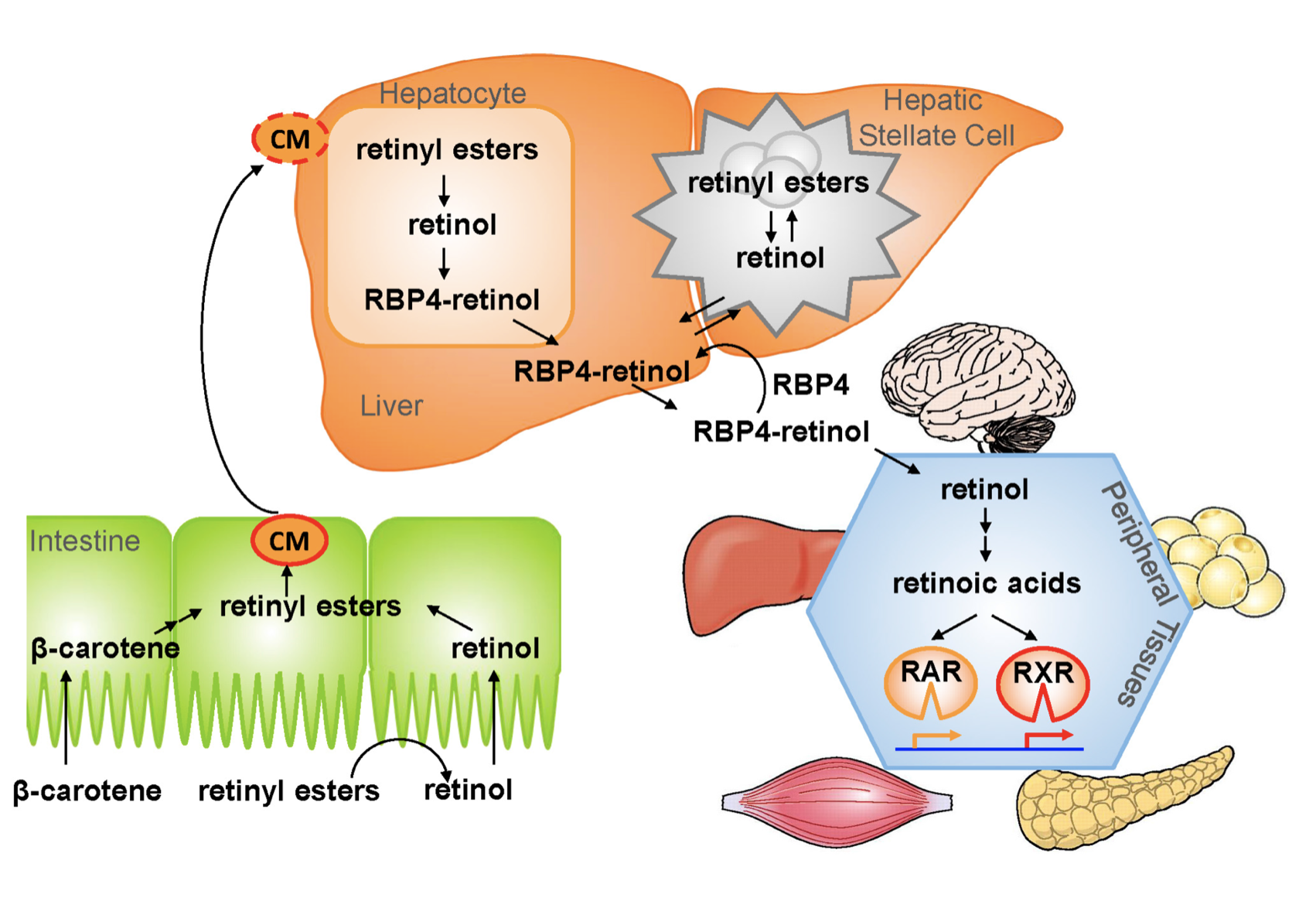
The Physiology of the Vitamin A is as follows:
1.- Ingested food is digested in the stomach where retinyl palmitates (esters) are released from proteins. Retinol and beta-carotene are absorbed directly into the small intestine where retinyl esters and betacarotene are transformed into retinol . Retinol is the most easily absorbed form of vitamin A.
2.-That retinol absorbed by the enterocytes in the ileum (small intestine) along with bile is then transported to the liver with the help of chylomicrons a protein that transports fat.
3.-Fifty to 80% of the vitamin A is stored in the liver and the remaining is deposited into adipose tissue, lungs and kidneys.
4.-When stored retinol is released from the liver into the circulation to target organs, it is bound to plasma retinol-binding protein (RBP4) a transporting protein produced by the liver that requires ZINC, which is synthesized by the liver; This complex is stabilized by transthyretin (TTR), which reduces renal excretion.
Retinol is a crucial component for reproduction, embryological development, cellular differentiation, growth, protein synthesis, and immunity in the form of retinoic acid and vision in the form of retinal.
One of Vitamin A additional roles is in epithelial health of skin and mucous membranes. It increases epithelial turnover which is crucial during would healing. It also has anti-oxidative effects which prevent cell damage and can prevent or reverse the effects of other damaging agents. In addition to these benefits it has also been associated with increasing collagen, fibronectin, keratinocytes and fibroblast, all important in wound tissue structure. There have been some studies that suggest giving higher doses of Vitamin A in patients with non or slow healing wounds.
It is important to remember that we have documents delayed diagnosis of adult vitamin A deficiency leading to significant night blindness in adults. It is critical that the patients and their primary care physicians are acutely aware of this possibility. In majority of the patients with low vitamin A, post weight loss surgery, aggressive supplementations, including injections need to be considered as a part of the treatment regimen.
We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here