Tag: Reflux
Three Different Problems: Gastritis, Gastroesophageal Reflux, and Bile reflux Gastritis
June 05, 2025 4:52 am
Gastritis is a general term used for the description of symptoms associated with several very different physical conditions and require different treatments based on their ideology . Gastritis, gastroesophageal reflux, and bile reflux gastritis
Gastritis may be caused by excess acid or bile in the stomach. Some patients may have gastroesophageal reflux due to a hiatal hernia, which needs to be treated surgically with Nissen fundoplication, regardless of the size of the hernia, contrary to what gastroenterologists recommend by prescribing antacids for an extended period. I have seen patients who have had one cm hiatal hernia and have been very symptomatic, and others who have had larger hiatal hernias and have been asymptomatic. Size should not be a determinant of whether the patient has had or will have a hernia repair or not.
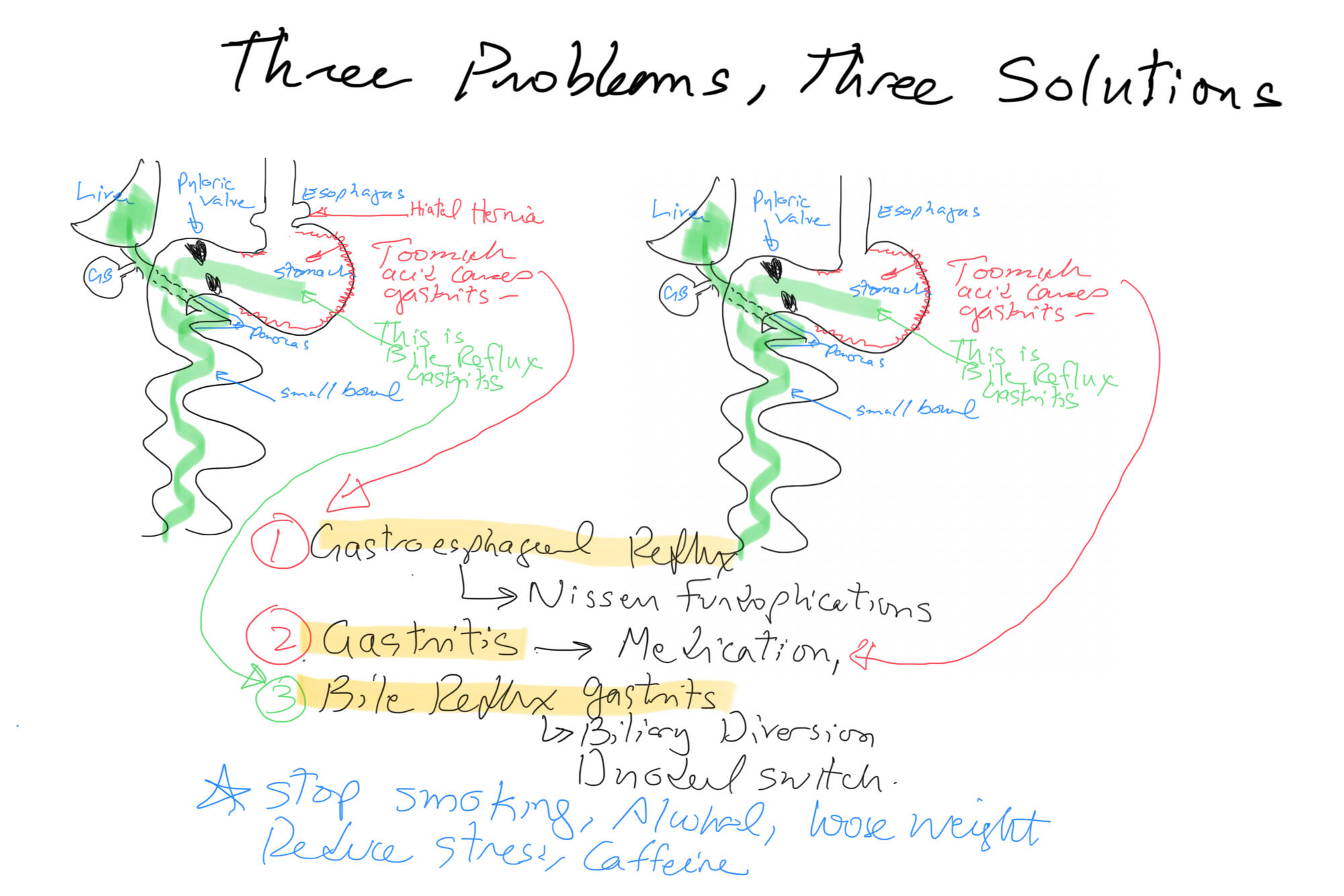
Billiary Diversion is the definitive surgical procedure for Bile Reflux Gastritis.
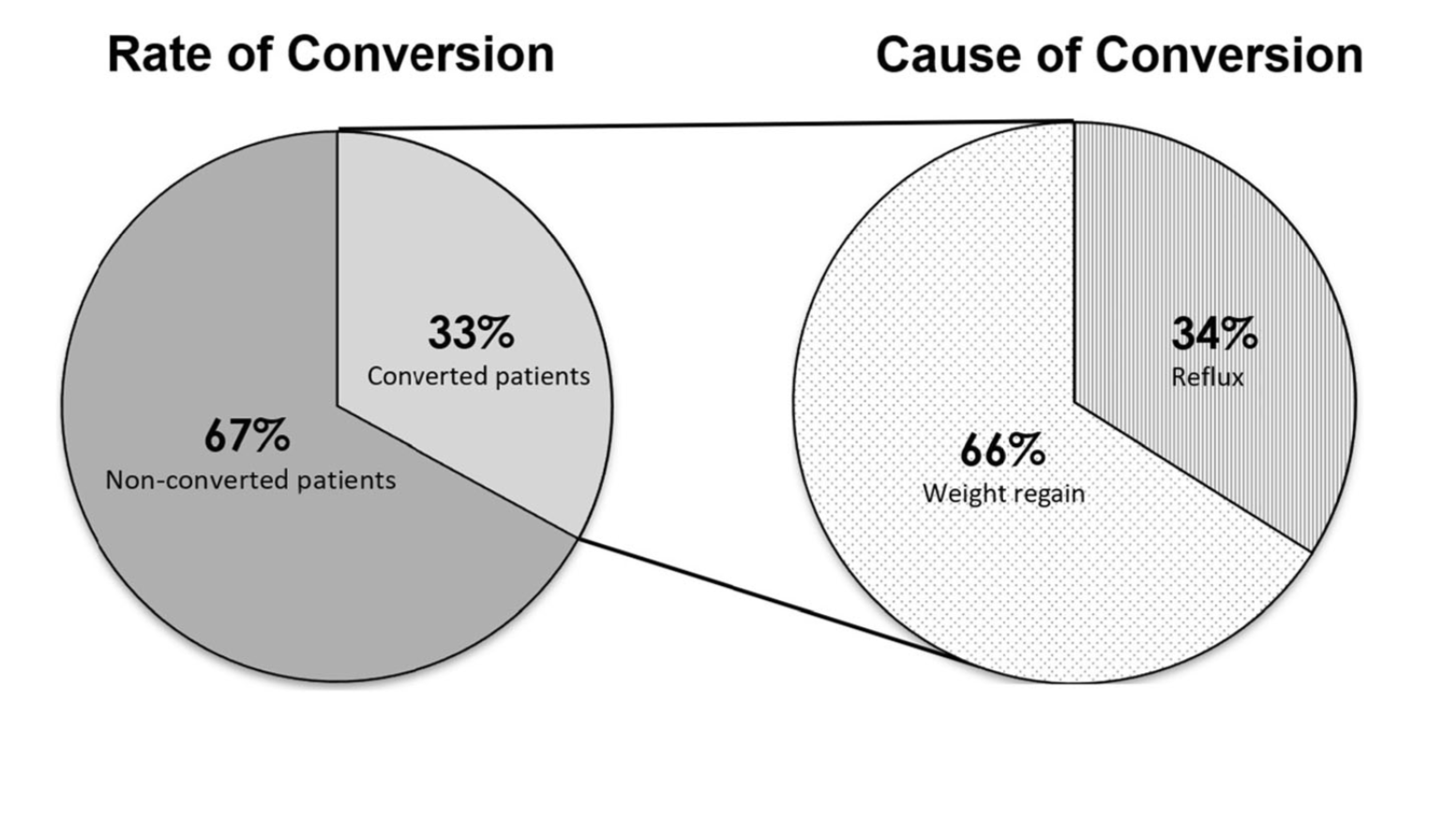
Sleeve And Weight Regain
July 22, 2019 9:50 am
Shared Success- Samantha had a Sleeve to Duodenal Switch Revision
July 14, 2017 9:30 am
After struggling with obesity for most of my life I was finally fed up. I had heard about weight loss surgeries before but was always under the common misconception that it was for people who wanted the “easy” way out of a hard situation. I had been working out and reducing calories and tried every popular diet and trainer you could think of. I was still huge and each time I would stop one of these extreme programs I would only end up larger than I was before.
My husband’s cousin had the sleeve surgery and she raved about it. Watching her success is what started to open my mind to surgery, but I was only considering the sleeve gastrectomy. I went to a center in another state that offers Duodenal switch, lapband, RNY and the sleeve. The surgeon I met with strongly suggested RNY to me, but I was stuck on the sleeve. I didn’t want my intestines touched period. I had the sleeve surgery on October 9, 2013.
My high weight was 402 lbs and I weighed 343 on the day of my sleeve surgery. I actually did well with the sleeve and was able to get down to 218 as my lowest. However it was still much like dieting. It was so stressful. After a while my body wouldn’t drop the weight regardless of how little I ate and exercised. I was eating 800-1200 calories a day and low fat meals and working out and kept slowly gaining weight. I was frustrated and honestly I gave up. My reflux wouldn’t go away so I visited a bariatric surgeon in my area who suggested that we essentially re-do the sleeve surgery to make my sleeve small again so that I would eat less and lose weight again. I got a second opinion and that surgeon suggested I revise to RNY. I went to obesity help’s website to explain my situation and a lot of people with much more experience than me HIGHLY urged me to see Dr Keshishian before making a decision. He was said to be an expert in revision weight loss surgery. I almost cancelled my appointment and didn’t have hope with this doctor either, but since I was in a dead end I went anyway. Dr Keshishian told me it wasn’t my fault. WHAT!? I had never heard that before. I usually get the shame from doctors who assume I must not be trying or that I am secretly eating something wrong. He ordered tests and told me it was “simply science” and I just LOVED him! I had a stricture in my Sleeve that needed to be repaired so since I needed surgery anyway I decided to go ahead and revise to a surgery that has the highest success rate, Duodenal Switch.


I was so scared of my intestines being cut and Dr. Keshishian eased my fears. I wish I had went that route the first time but then I might not appreciate it like I do now. Duodenal switch is the ONLY surgery I would recommend to anyone. As Dr K says it’s simple numbers. It’s the surgery with the highest percent of excess weight lost and kept off. I was 252 before my revision from Sleeve to Duodenal Switch and I am just at a year out and today I weigh in the low 190’s and I am still losing. Dr K’s goal for me was about 180. My goal is about 175. I eat more fat now than I ever did even when I was 400 lbs. I enjoy what I eat and I enjoy exercising and most of all I get to enjoy seeing results from my hard work. Food no longer causes me stress and anxiety. I know with 100% certainty that I made the right decision. Thank you Dr. K for your great skill and I don’t mean just with the knife but with the way you are able to make a high anxiety situation seem like no big deal.


Reflux and Hiatal Hernia
April 17, 2017 9:41 am
One of the leading reasons for Gastro-esophageal reflux disease (GERD) is a physical defect called a Hiatal hernia. The esophageal Hiatus is the opening in the diaphragm where the esophagus enters from chest cavity allowing the esophagus to pass into the abdominal space. If the opening in the diaphragm is much larger than the esophagus, it will result in reflux of the stomach secretions and food from the stomach into esophagus. *Note: Graphic surgical pictures below
Hiatal Hernia Causes:
- heavy lifting
- coughing
- obesity
- injury
- persistent vomiting
- age related
Reflux and Hernia Symptoms:
- sour taste
- reflux
- heartburn
- belching
- chest or abdominal pain
- difficulty swallowing
- vomiting
- no symptoms


The treatment includes dietary changes, medication and in those who do not improve surgery.
Hiatal hernia repair includes tightening of the dilated opening of the esophageal hiatus by re-appoximating the separated muscle fibers of the right and the left crus. This tightens the defect in the diaphragm and helps prevent part of the stomach or stomach contents from entering the chest cavity.
You can find further information and dietary changes regarding Hiatal Hernia and GERD here, including information unique to weight loss surgery and Hiatal Hernia. You can also find further surgical information, as well as a surgical video here.
Hiatal Hernia Treatment
February 13, 2016 4:45 pm
Hiatal Hernia may be one reason for developing symptoms of GERD (Gastroesophageal reflux disease). As we have discussed previously, the treatment for reflux should not be long-term use of the “purple pill”, or all PPI’s, as advertised on TV. There is a large population who are delaying definitive care and probably increasing their chance of esophageal cancer by taming the symptoms of the reflux with over the counter or prescription medication. However, it is important to note that taming the symptoms isn’t necessarily stopping the effects. Be proactive and request to be sent to a surgeon to fix any issues if you are being recommended to “….take the medication and come back again for another endoscopy again ….”
Types of Hiatal Hernia:

This is an example of a patient who had been told to take the medication and just keep and eye on it with repetitive endoscopies. He had to have hiatal hernia repair with Nissen fundoplication for progressively worsening symptoms even on maximum treatment.

This is another example of a hiatal hernia repair procedure of a patient with a previous history of sleeve gastrectomy. In this patient, mesh had to be placed in order to fix the hiatal hernia.
Failure of Anti-Reflux Procedures
September 28, 2015 7:13 am
A recent study Published in JAMA Surgery, quoted rate of 10-20% of patients who have had anti-reflux surgical procedures will have recurrence of his symptoms within the research data. There are numerous studies that have identified predictive factors leading to return of the symptoms after surgical intervention. Some of these predictive factors are improper diagnosis, inadequate work up and technical issues.
Due to the significant rise of sleeve gastrectomy as well as a high failure rate of the lap band, we have seen several patients presenting with significant reflux disease after weight loss surgery. There is a little scientific data regarding the failure of anti-reflux procedures in patients who have had previous weight loss surgical operations. In our practice, however, we have extensive experience with anti-reflux operations in patient who have had previous weight loss surgeries including Gastric Bypass, Adjustable Gastric Banding, Sleeve Gastrectomy and Duodenal Switch operation.
Improper diagnosis, inadequate work up, and technical issues have been cited as possible causes for recurrence of symptoms in patients who have not had weight loss surgery. One could assume that those variables are still a factor in addition to other factors resulting from a previous weight loss surgery. The complications of a previous weight loss surgery can not be under-estimated; an example would be a patient with significant esophageal motility issues directly related to an Adjustable Gastric Band. Other situations that exacerbate symptoms of reflux are an hour glass shaped sleeve or a stricture mid stomach post Sleeve Gastrectomy or Duodenal Switch.


In our experience, some patients have responded well with anti-reflux surgical procedures and mesh placement if indicated after a compete work up with has included and upper endoscopy, upper GI series, manometry and Ph studies. Any patient with symptoms of reflux after weight loss surgery, should be evaluated, and a complete work up should be performed to establish the proper treatment options. It is not wise to have patients be treated with proton pump inhibitors as a default treatment without a complete work up for any patient with reflux. These class of medications have significant side effects associated with them. Furthermore, prolonged reflux is a factor in development of Barret’s Esophagus, a pre-cancerous condition.