Category: Achalasia
Cholangitis
May 24, 2026 11:33 am
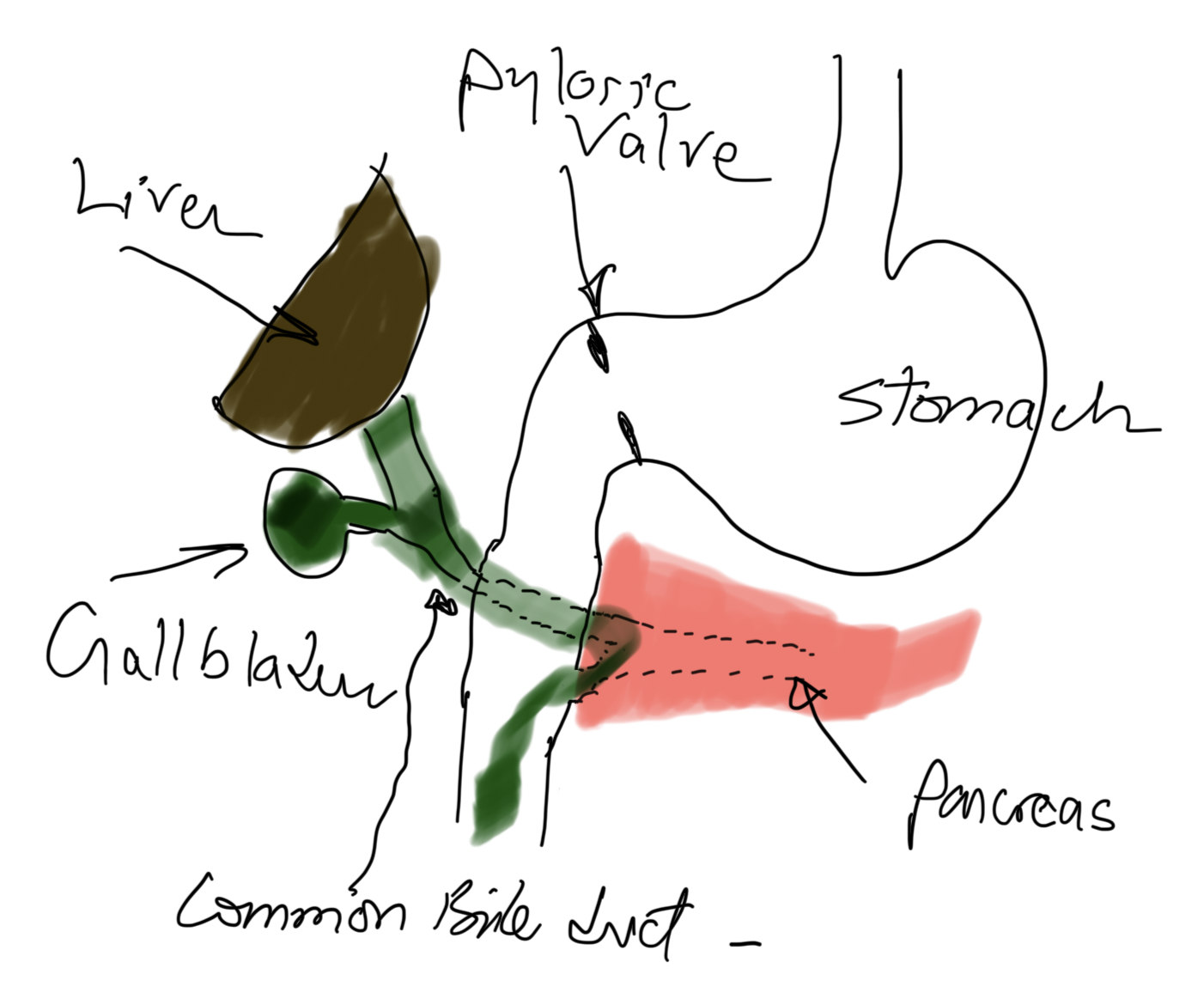
Cholangitis refers to infection and inflammation of the bile ducts because of obstruction and introduction of bacteria or other pathogens from the GI tract.
- Hydration with IV fluids,
- Broad coverage with IV antibiotics administration and
- Drainage procedure (ERCP, papillotomy, Stent placement, Cholecystectomy with common duct exploration, and T-tube placement)
These steps are almost all taking place concurrently and urgently. This is not something a patient waits and sees how it goes- it only goes one direction, from bad to worse. This is not to sound alarmist; a correct diagnosis is critical.
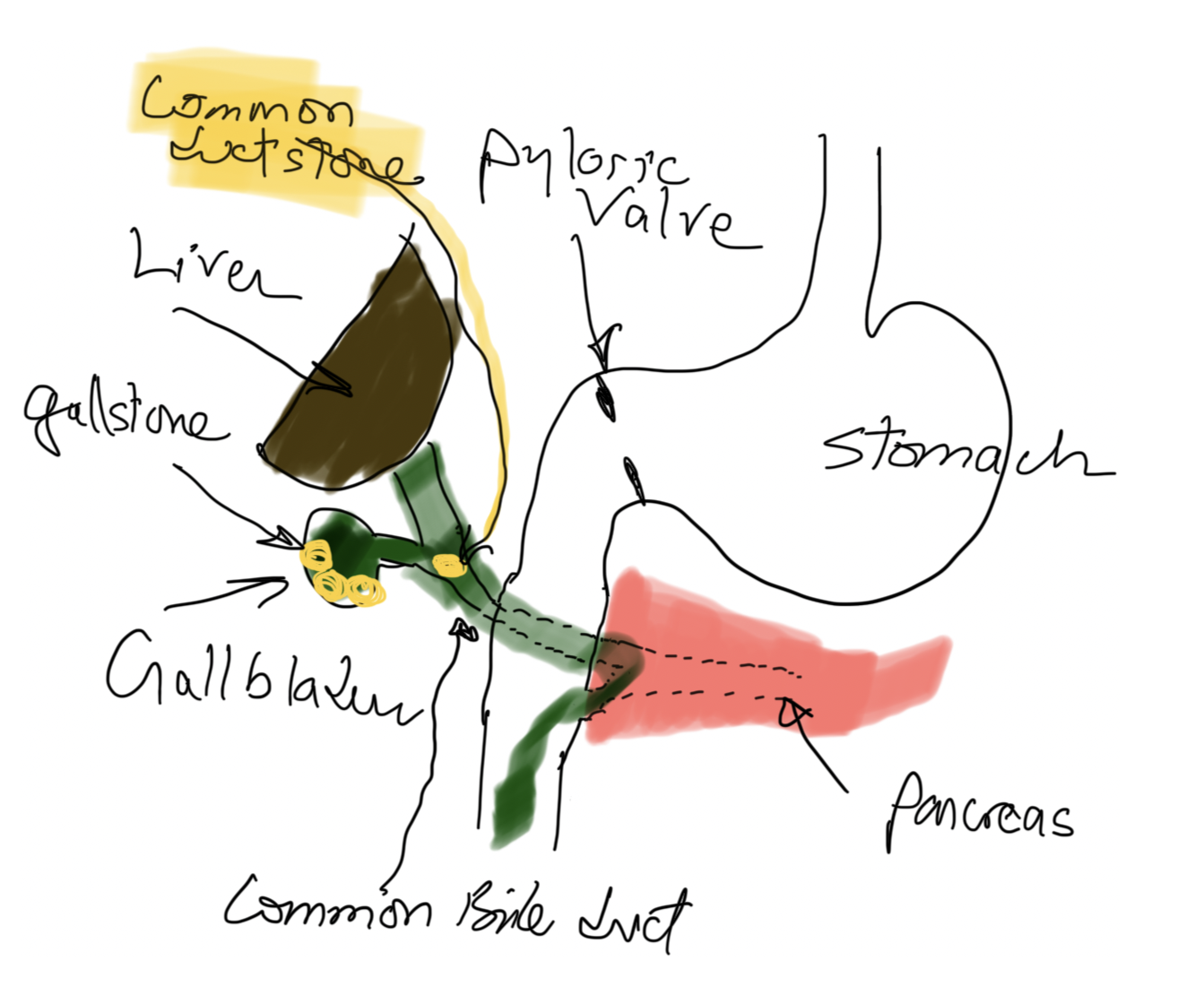
Risk factors for cholangitis may include gallstones that travel down the bile duct and cause jaundice, pancreatitis if passed, immunosuppression, malnutrition, and diabetes, to name a few.
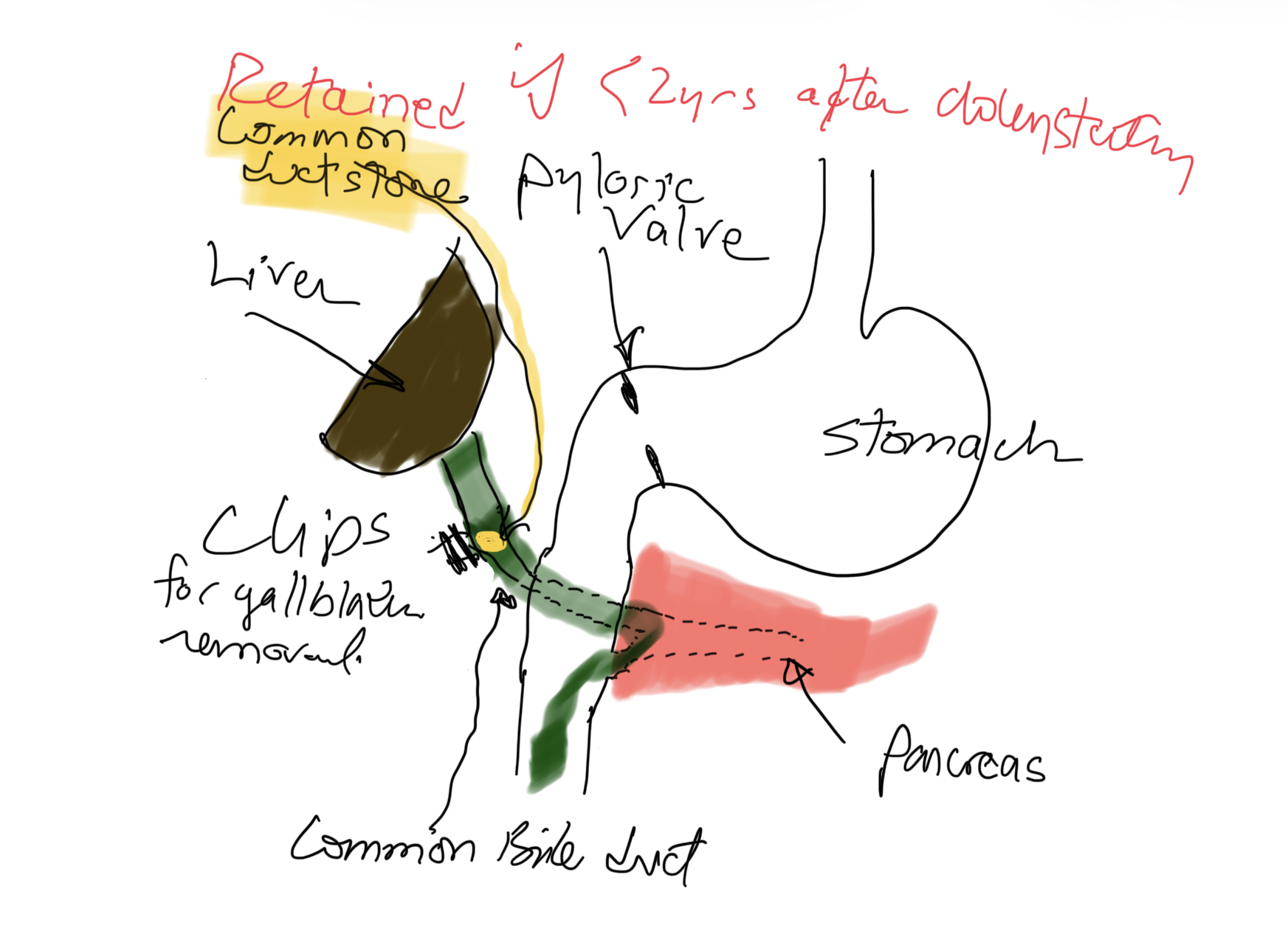
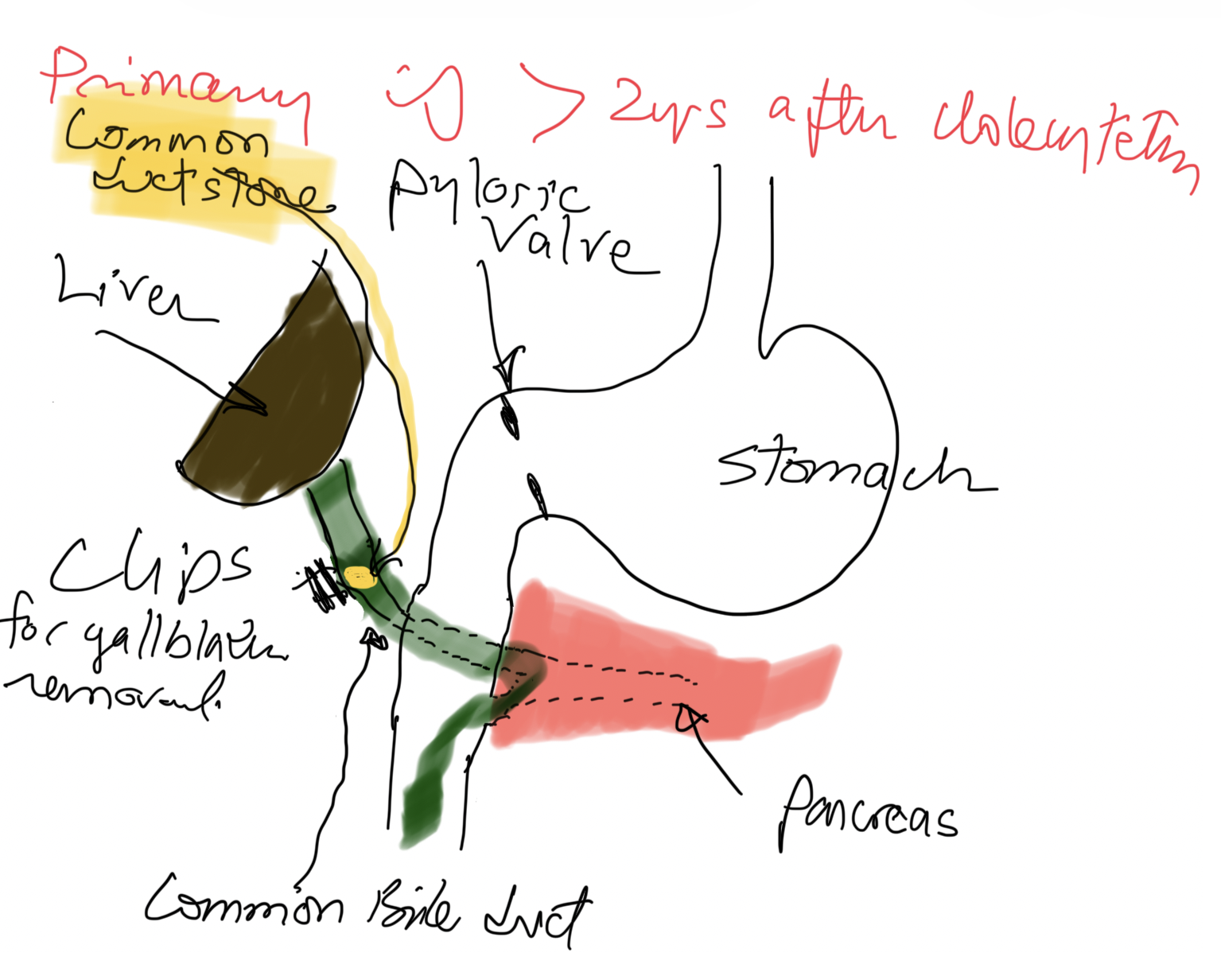
If a patient has gallstones in the bile duct less than 2 years after cholecystectomy, it is a Retained Stone(s), meaning there was a small stone that was not in the gallbladder and was not seen on US, intraoperative cholangiogram, or ERCP (if performed before surgery).
Three Different Problems: Gastritis, Gastroesophageal Reflux, and Bile reflux Gastritis
June 05, 2025 4:52 am
Gastritis is a general term used for the description of symptoms associated with several very different physical conditions and require different treatments based on their ideology . Gastritis, gastroesophageal reflux, and bile reflux gastritis
Gastritis may be caused by excess acid or bile in the stomach. Some patients may have gastroesophageal reflux due to a hiatal hernia, which needs to be treated surgically with Nissen fundoplication, regardless of the size of the hernia, contrary to what gastroenterologists recommend by prescribing antacids for an extended period. I have seen patients who have had one cm hiatal hernia and have been very symptomatic, and others who have had larger hiatal hernias and have been asymptomatic. Size should not be a determinant of whether the patient has had or will have a hernia repair or not.
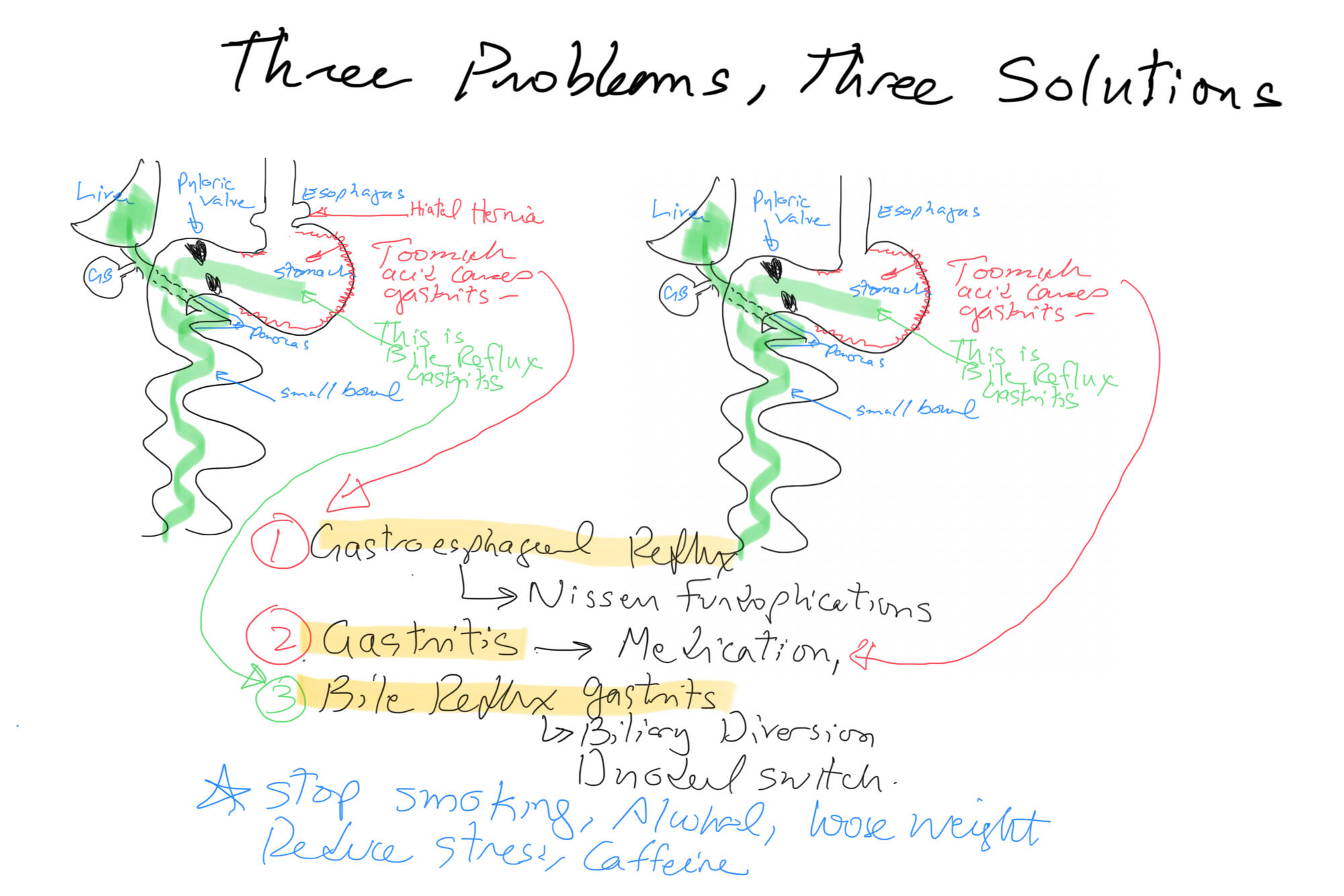
Billiary Diversion is the definitive surgical procedure for Bile Reflux Gastritis.
Gastroesophageal Reflux: Bile Vs. Acid
May 14, 2019 12:52 pm
Gastroesophageal (GE) reflux is the condition when the stomach contents are able to “reflux” back through an incompetent lower esophageal sphincter (LES) into the esophagus.
Gastroesophageal reflux Disease (GERD) is a clinical condition caused by long-standing reflux that results in microscopic and visible changes to the inner lining of the esophagus and esophageal mucosa.
GERD is nondescript as to the cause of the condition. It only states that the stomach contents have been irritating the lining of the esophagus on a chronic basis. This can be caused by an anatomical abnormality of the GE junction (hiatal hernia) or may be related to dysfunction of the LES. Other possible causes of GERD may be infection (H. Pylori), environmental (stress), and dietary (nicotine, alcohol, caffeine, spicy food) in origin.
So far, we have not clarified the chemical nature of the refluxed content.
In Acid Reflux, the relative acid overproduction of acidic secretion and the exposure of the esophageal mucosa need to be addressed. This is accomplished by acid suppression medications, anti-histamine (H2 blockers), and Proton pump inhibitors (PPIs). The physiology and the mechanism involving this condition are well understood. As a surgeon, however, I do see patients who should have had surgical intervention. The initial mode of therapy for a patient with documented acid reflux and or symptomatic hiatal hernia is placing them on medication. These patients are then recommended to have a related upper endoscopy. Patients who do not improve or where deterioration of the esophageal mucosa and the presence of precancerous cells are referred for surgical intervention.
Bile Reflux, contrary to acid reflux, may have tiny, if anything, to do with the LES. The symptoms experienced by the patient may be as after related to the excessive bile in the stomach, which is seen frequently
after cholecystectomy, or in those patients with a dysfunctional gallbladder (low EF on HIDA scan).
The treatment of Bile reflux is Duodenal Switch without the associated sleeve gastrectomy component in addition to repair of hiatal hernia if present. Ann Surg. 2007 Feb; 245(2): 247–253.
Achalasia
November 15, 2015 9:24 am
Achalasia is a motility disorder of the esophagus. The neuro-muscular mechanisms which is suppose to propel food down the esophagus after the initiation of swallowing does not work and this results is a narrowing of a segment of the esophagus, with significant dilation of the esophagus above.
The weight loss with achalasia is the result of dysphagia (inability to swallow) both solids and liquids. Patient with other esophageal motility disorders have primarily solid intolerance, but with proper positioning tolerate liquids well. This is because unlike other esophageal motility disorders (where the esophagus fails to push the food down after swallowing is initiated) in achalasia, the food is carried down to a certain level, but it gets stuck, because of non relaxation of muscles that form the lower esophageal. The key would be to make the proper diagnosis by manometry, endoscopy, and radiologic studies. The treatment for achalasia is very different-than that of an esophageal motility disorders.

In Achalasia, at the treatment includes nutritional support, and laparoscopic division of the muscle fiber that are wrapped around the esophagus to allow for gravity to help with the passage of the food down to the stomach. Additionally this operation should include steps and components to prevent reflux. This video shows segments of the operation.
Surgical Treatment of Esophageal Achalasia (Esophageal Motility Issue)
January 23, 2015 6:50 pm
Achalasia
October 08, 2010 7:05 pm
I was asked if a patient with achalasia could have the duodenal switch operation.
My first reaction was why would anyone with achalasia need to have any weight loss surgery? This is because an almost universal finding with achalasia patients is significant weight loss.
The weight loss with achalasia is the result of dysphagia (inability to swallow) both solids and liquids. Patient with other esophageal motility disorders have primarily solid intolerance, but with proper positioning tolerate liquids well. This is because unlike other esophageal motility disorders (where the esophagus fails to push the food down after swallowing is initiated) in achalasia, the food is carried down to a certain level, but it gets stuck, because of non relaxation of muscles that form the lower esophageal. The key would be to make the proper diagnosis by manometry, endoscopy, and radiologic studies. The treatment for achalasia is very different-than that of an esophageal motility disorders.
Now going back to the question of a patient with achalasia having duodenal switch… If the diagnosis is correct, then the patient will benefit from a procedure where the outer muscle layers of the esophagus are divided, without entering the lumen of the esophagus. As a part of the same procedure,
| Esophageal Motility | Achalasia | |
| Weight Loss | Some | Significant |
| Intolerance | Solids | Solids and liquids |
the patient then has to have a Nissen wrap to prevent reflux. In my
opinion, any procedure that increase the possibility reflux should be avoided. Any procedure that causes vomiting should be avoided. Additionally from a technical perspective, for a Nissen wrap to be done, the top part of the stomach should be left intact.
In my opinion, this rules out the possibility of Adjustable gastric banding or the gastric bypass. Both of these are restrictive procedures that slow passage of the food past the stomach pouch. This is recreating the problem more than solving it.
Duodenal switch operation will probably be the best option. A larger stomach sleeve can be done, with a warp to prevent reflux. The lengths of the common and alimentary limbs can be adjusted so that the patient looses weight. I would have to once again raise the issue of correct diagnosis, in that most achalasia patients have significant weight loss, and will probably not be in the need of any weight loss surgery.
An esophageal motility disorder however is something that I have seen as a complication of Adjustable gastric banding. In a quest for more weight loss, the band is continuously filled. There is a fairly large body of scientific published data (both case reports and small series) that talk about the problem of AGB causing esophageal motility disorders.The universal belief is however, that the conversion to alternative operations, Duodenal switch or gastric bypass will is at least some cases reverse the motility disorder.