Tag: diabetes
Bile Reflux Gastritis
May 19, 2026 4:13 pm
Hello, it’s best to clarify a few points:
- The difference between prevalence and incidence.
- Incidence means new cases over
- Prevalence refers to existing cases at any time
- The difference between causation, coexistence, and correlation
- Causation refers to a condition causing an effect.
- Coincidence refers to two conditions present together at the same time, with neither causing the other.
- Correlation refers to two conditions that may occur together, with no causation.
- Study size refers to the research data on which the information is based. The larger the population size studied, the better the sample data and the more conclusive the results.
- Confounding factors.
Diabetes and Weight Loss Surgery
April 06, 2020 5:51 am
The scientific literature is riddled with evidence pointing to the benefit of early metabolic surgery as a superior treatment, remission and possible cure option for diabetes. Unfortunately, the medical education, pharmaceutical companies, primary care healthcare delivery systems and third party payers (health insurance companies) have not caught up with the published data. The American Diabetes Association has changed their guidelines to reflected the benefit for combating diabetes with weight loss surgery.
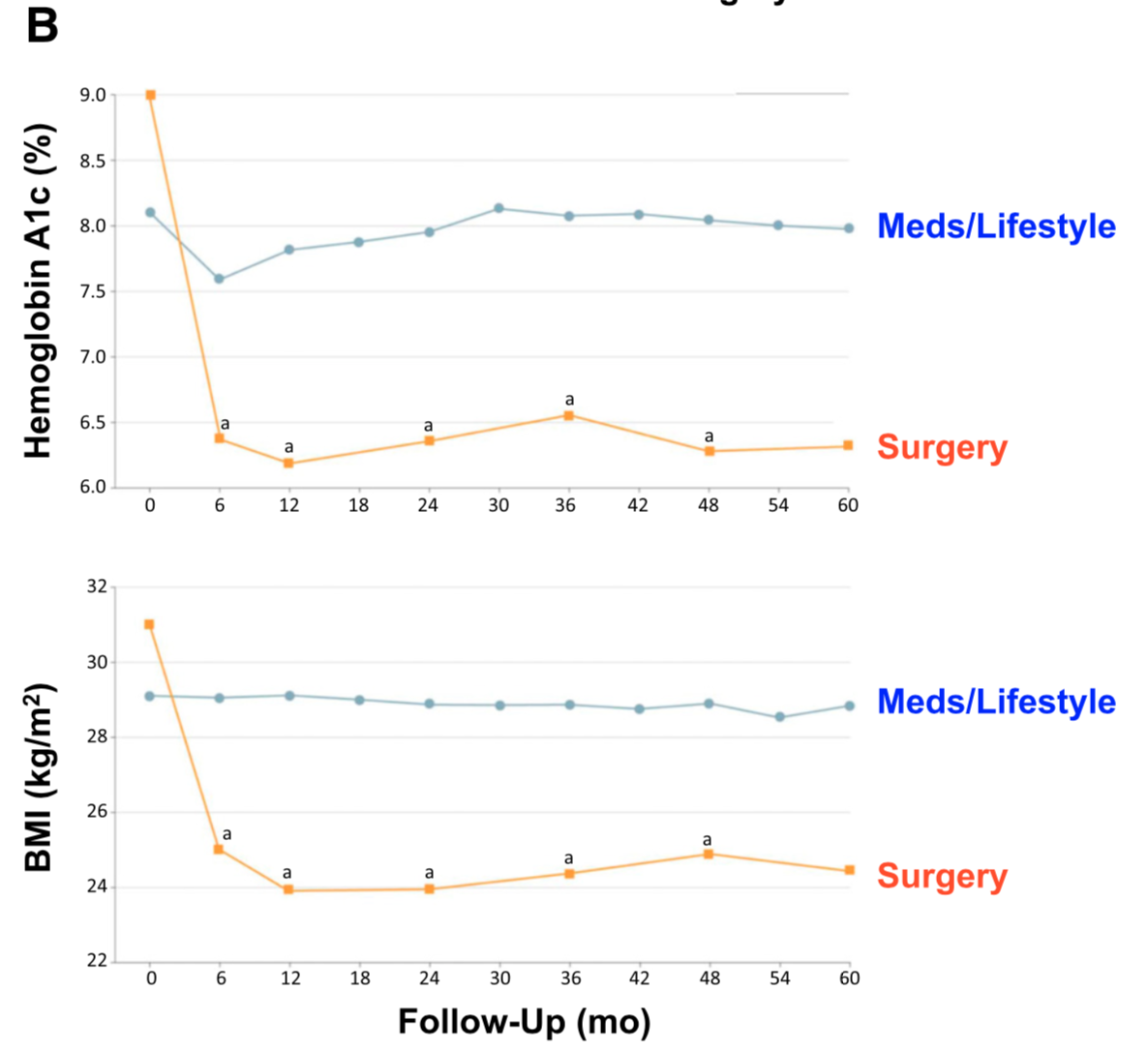
There is ample evidence of the superior outcome of surgery as a treatment option for diabetes when compared to medical managment. Cummings et.al, in a published article in Diabetes Care, showed sustained stabilization of the Hemoglobin A1C six years after surgery. In contrast, there was no significant changes noted in the non-surgical group.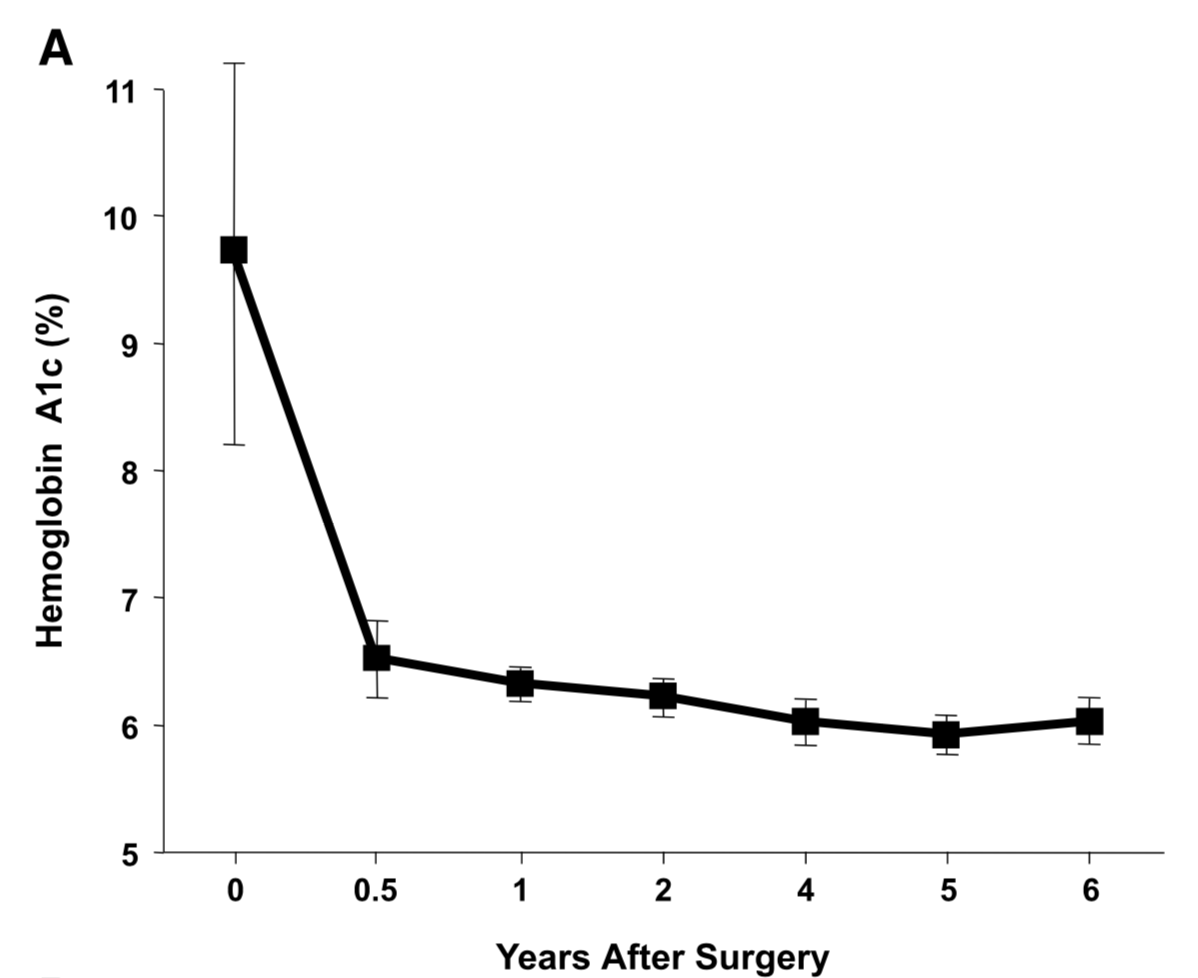
Jans et.al. , in November of 2019 showed that the patients who had NOT been on Insulin, and had metabolic surgery had the highest long term success for resolution and remission of the diabetes. This identifies that having a patient be proactive in their care by having metabolic surgery improves success rates.
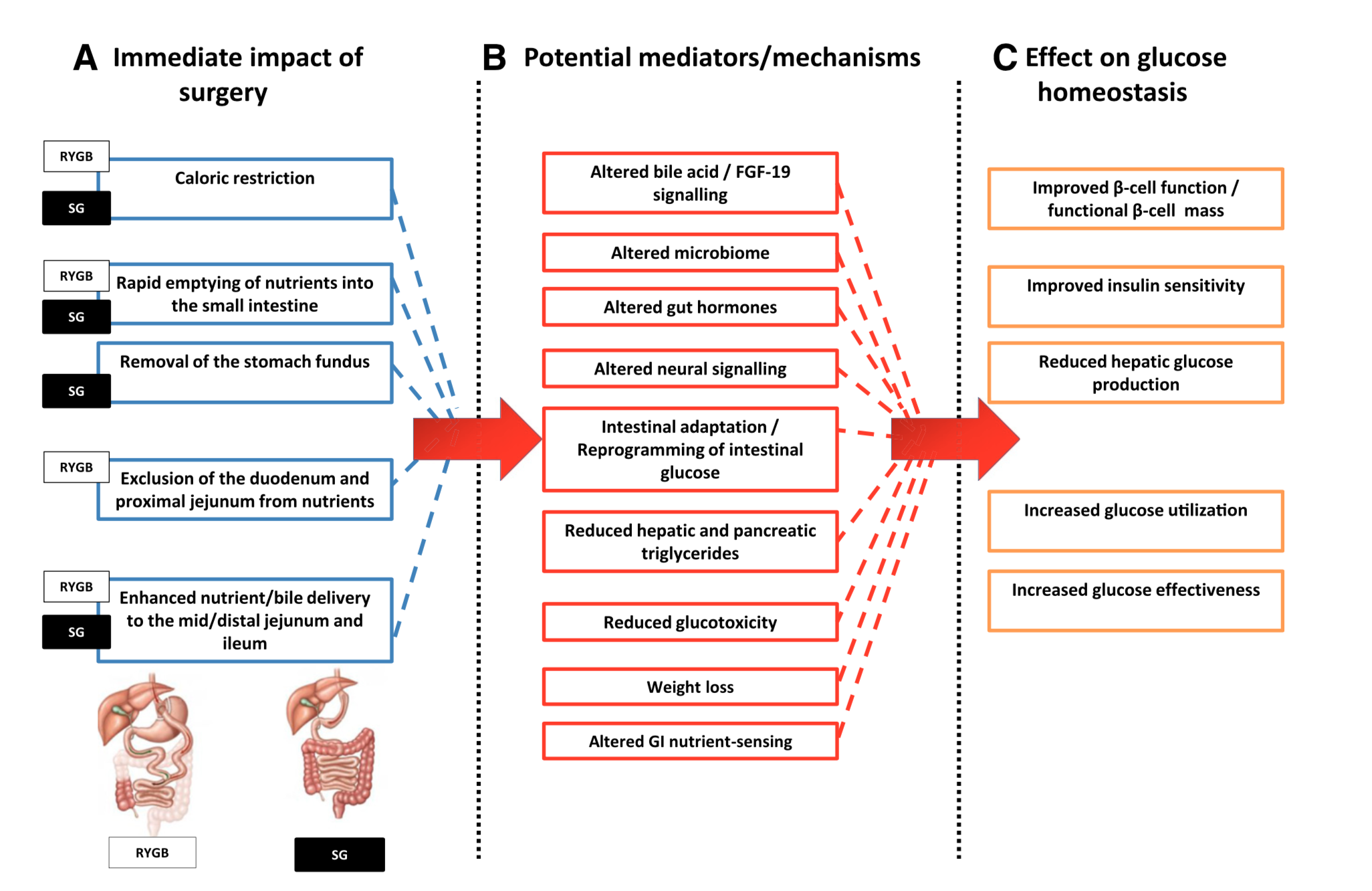
The exact mechanism by which the diabetes is resolved is unclear. The weight loss may play a role. There are numerous hormones and neuroendocrine modulators which control the complex metabolic pathways. Batterham et.al., in Diabetes Care (2016), published a summary overview of the possible mechanism involved in diabetes improvement following metabolic surgery.

There are a number of overlapping and sequential layers for possible reasons why diabetes resolves after weight loss/metabolic surgery. These may be directly related to surgery and the reduction of the calorie intake or absorption. It may also involve the neuroendocrine modulators.
What can be said definitively is that early surgical intervention is best and most likely the only permanent solution to type II diabetic resolution. There is no medical justification in not considering metabolic surgery in diabetic patients who may also have difficulty with meaning a BMI< 35.
PolyCystic Ovarian Syndrome PCOS
September 04, 2018 9:58 am
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.

Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
Bariatric Surgery can improve PCOS in those individuals with Type 2 Diabetes Mellitus. Further information on weight loss surgery and its effect on PCOS here.
Liver Injury and Obesity
April 30, 2018 11:36 am
Liver is a vital organ. It has many roles in the physiologic pathways including protein productions, clotting function, iron metabolism, production of bile and cholesterol, etc. as well as metabolism and filtering of waste products. We should think of it as a refinery, for conversion of raw material from food to energy used by our body, in addition to a processing and distribution center for mineral, and nutrients. Liver injury can have devistating effects and long term ramifications if unchecked.
Liver is also very resilient and forgiving to stressors and injury. The liver will tolerate repeated insults caused by Medication (both prescription and over the counter) , obesity, Diabetes, alcohol, and herbal supplements, to name a few, but only if care is taken and the offending stressor is removed. During the injury phase, however, the liver may have a difficult time keeping up with bodily function needs due to loss of fully function cells.
The anatomy of liver can change from normal (both visually to the naked eye and under microscope) to mild inflammation and reverse back to normal if the underlying causes of injury are removed. IF, however, the anatomy of the liver changes with fibrosis, it crosses to an irreversible range where it can only be prevented from progressing rather than reversing.



In the obese population, Non-alcoholic Fatty Liver Disease (NAFLD) causes inflammation and a slowly diminishing functionality of the liver. NAFLD is the leading cause of liver disease in the U.S. Unchecked or untreated NAFLD can progress to NASH (Non-Alcoholic Steatohepatitis. NAFLD, or “fatty” liver disease, is an accumulation of fat within the liver. NASH is a progression that can lead to inflammation of the liver cells or advance to fibrosis and cirrhosis. In addition to liver injury, there is some evidence that NAFLD also correlates with cardiovascular disease.
Causes of NAFLD:
- Obesity
- Type 2 Diabetes Mellitus
- Hypertension
- High cholesterol
- Sedentary lifestyle
Symptoms may include fatigue, right upper quadrant pain, and liver enzyme elevation.
During bariatric or weight loss surgery, we visualize and occasionally biopsy the liver to define the degree of injury, if identified. Following weight loss surgical procedures, a rise in liver function enzymes may be expected due to the processing of waste products following fat mass loss. However, long-term bariatric procedures can significantly improve NAFLD and NASH. Bariatric procedures require adherence to protein and supplement requirements and regular physician visits—the past blog of liver disease.
Weight loss surgical procedures improve liver function abnormalities.
Resistance Exercise BandsExclusive Member Content
July 19, 2017 12:47 pm
Less Invasive, Easier?
July 20, 2016 11:02 am
There is a continuous desire for a “less invasive”, “easier” procedure for the treatment of obesity and its associated co-morbidities. We have been very clear when discussing the benefits and long term outcome of the procedures. Let’s remind ourselves that “less invasive” does not mean a better option. In almost all cases a less invasive weight loss surgery means less weight loss, lower incidence of resolution of co-morbidities, and in some cases higher complications rate. Have we forgotten the adjustable gastric banding that was advocated to be the cure all for all obesity? All we hear now are the complications, the long term sequel of the reflux, hiatal hernia, irreversible esophageal injury, in addition to inadequate weight loss or weight regain.




Unfortunately, the same is to be said about the Sleeve Gastrectomy. We have said, as supported by the scientific literature, that the long term outcome of the sleeve gastrectomy is not as good as that of the Duodenal Switch procedure. This is true for the amount of weight loss as well as the resolution of the co-morbidities. We see quite a few patients who have gained their weight back after sleeve, never lost enough weight, and/or did not achieve resolution of their co-morbidities, such as diabetes, and are having their procedure revised to Duodenal Switch procedure.
Here is a recent publication that discusses this.
Along with the same argument, this is why I caution patients when having the SIPS or SADI procedures. There is a chance that when the long term data for SIPS/SADI is available there may be some benefits procedure. However, as it stands at this point in time, these procedures are not the same as the Duodenal Switch procedure. So in short, less invasive, easier isn’t better.
Weight loss Surgery for Treatment of Diabetes
May 25, 2016 7:21 am
New guidelines and recommendation are coming out of the second Diabetes Surgery Summit in the Fall of 2015. One major change is Metabolic or Weight Loss Surgery for the treatment of Diabetes. With all the advances made in newer classes of medication for treatment of diabetes, the majority of patients who are being treated fail to get to achieve the desired results of lowered blood glucose level. This is in contrast where weight loss surgical procedures such as Duodenal Switch can results in >95% cure rate of type II diabetes.
The American Diabetes Association has made the recommendation for weight loss surgical procedures be considered as a treatment option for type II diabetes.
Summarizing their criteria “According to the new Guidelines, metabolic surgery should be recommended to treat type 2 diabetes in patients with Class III obesity (BMI greater than or equal to 40 kg/m2), as well as in those with Class II obesity (BMI between 35 and 39.9 kg/m2) when hyperglycemia is inadequately controlled by lifestyle and medical therapy. It should also be considered for patients with type 2 diabetes who have a BMI between 30 and 34.9 kg/m2 if hyperglycemia is inadequately controlled, the authors agreed. The Consensus S

tatement also recognizes that BMI thresholds in Asian patients, who develop type 2 diabetes at lower BMI than other populations, should be lowered 2.5 kg/m2 for each of these categories. ”
This is a remarkable change in thought and policy on diabetic treatment and long term strategies that can only improve patient outcomes. Stabilization and blood glucose hemostasis can only improve patient health, health care utilization and health care costs.