Category: revision of sleeve gastrectomy
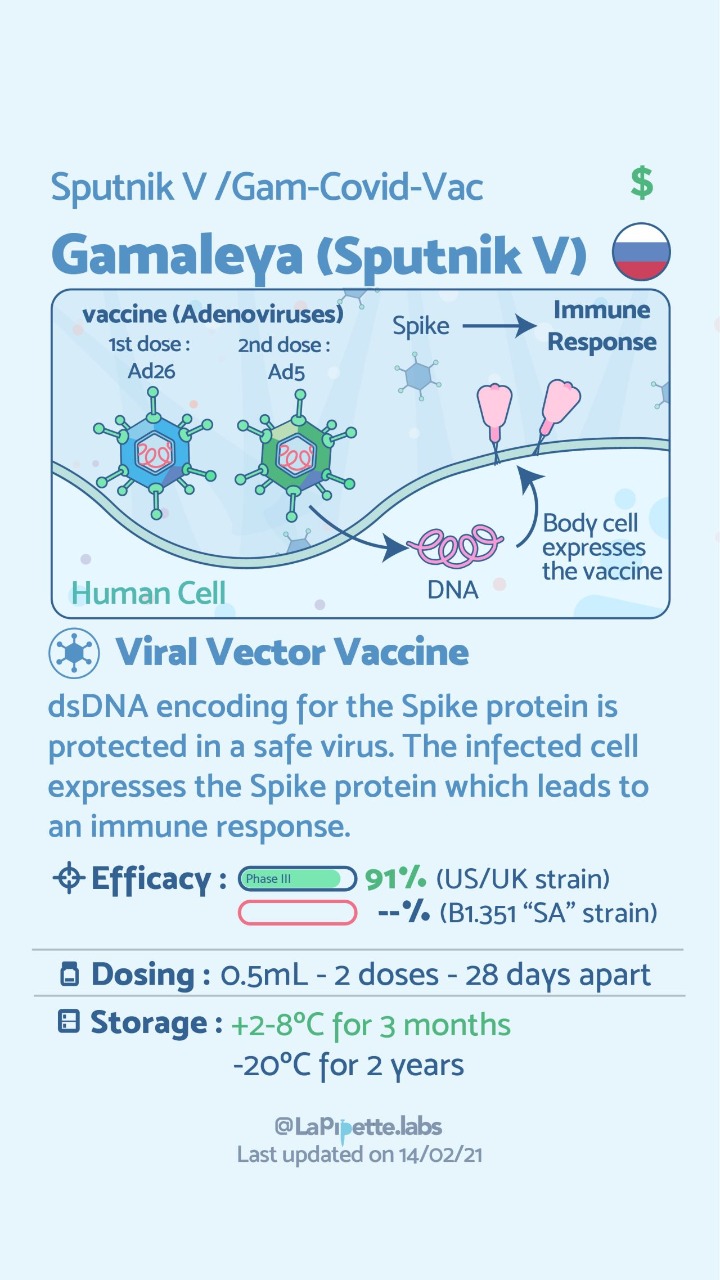
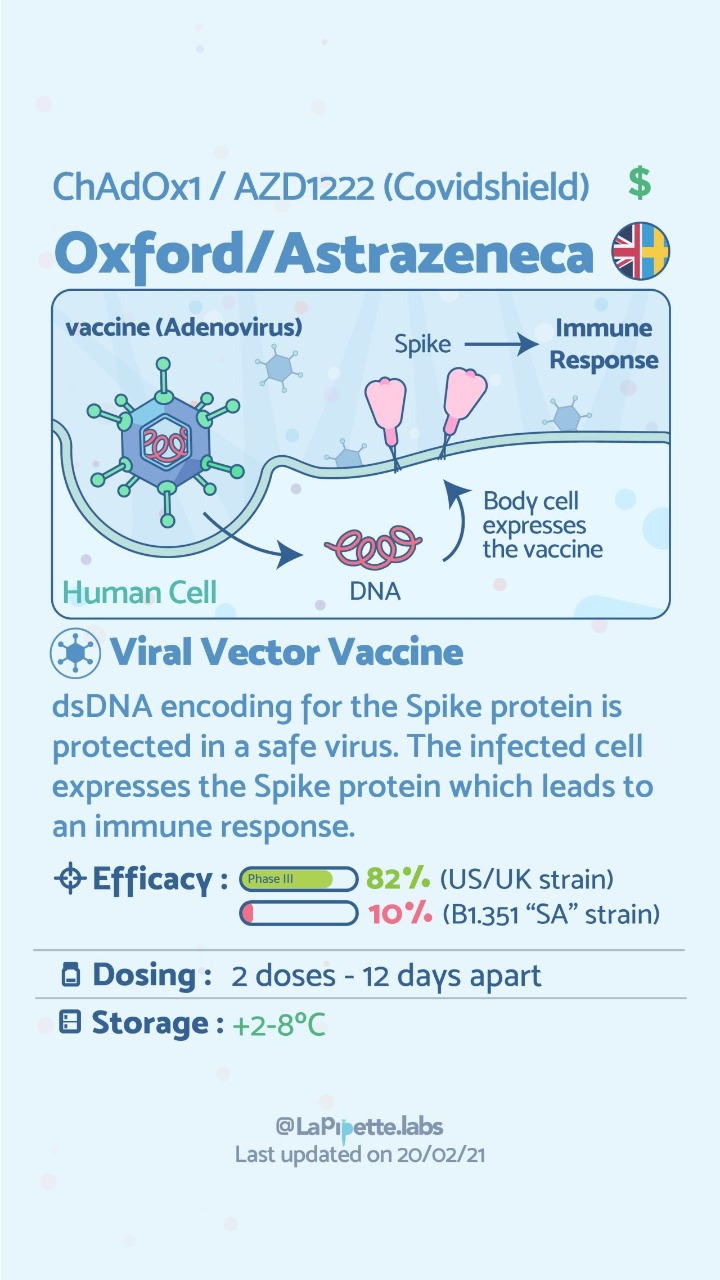
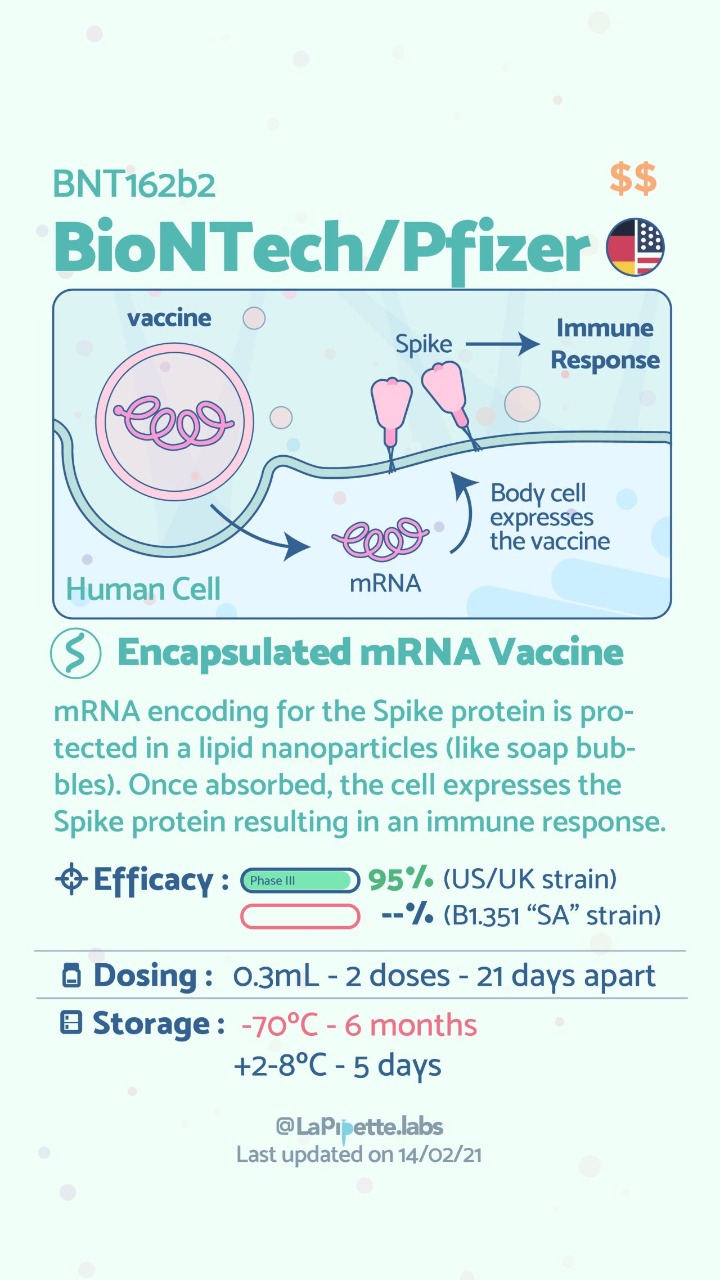
COVID Vaccines
March 05, 2021 3:50 pm
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
Sleeve And Weight Regain
July 22, 2019 9:50 am
Sleeve Gastrectomy Failure
May 07, 2019 12:53 pm
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
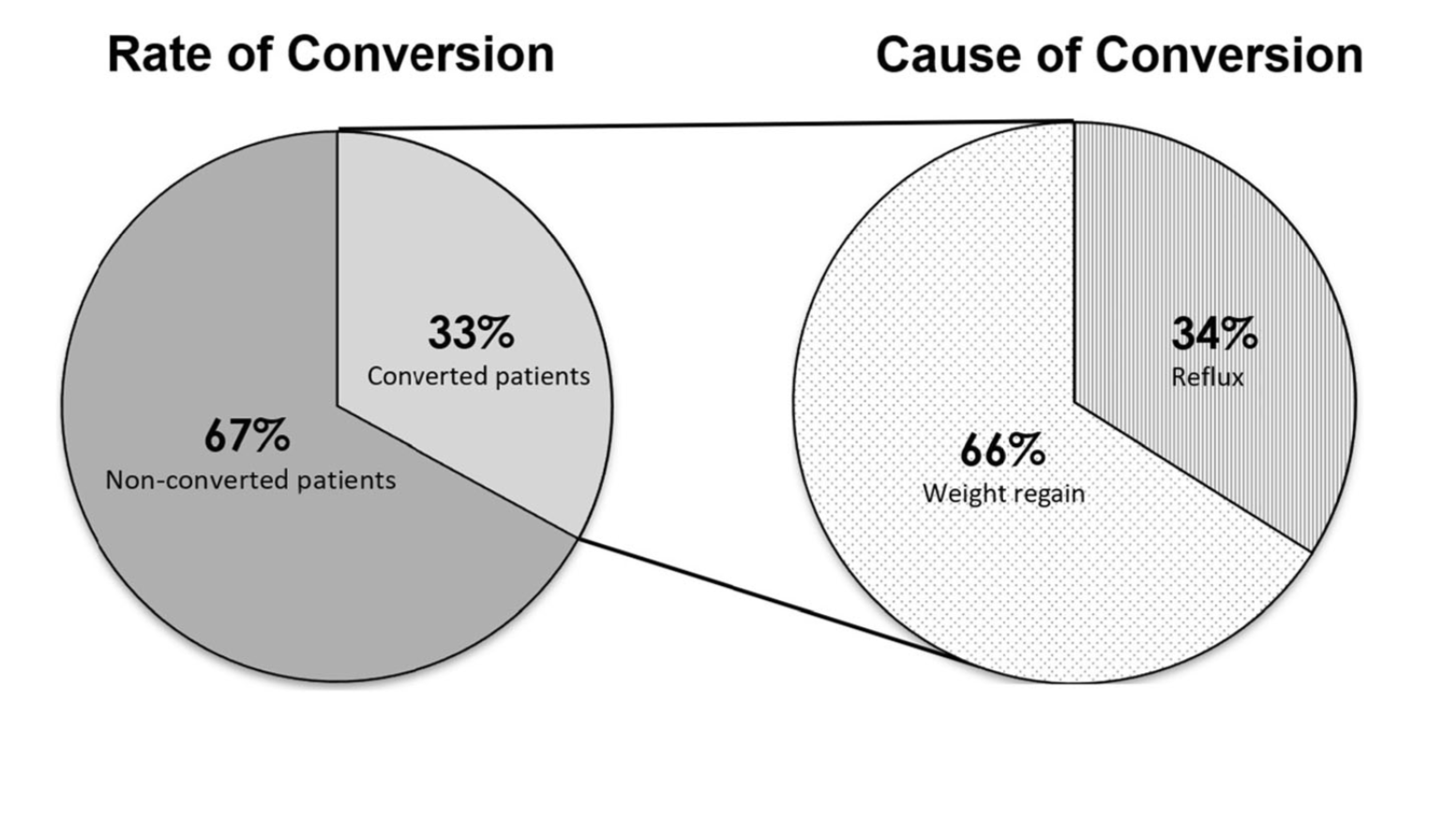
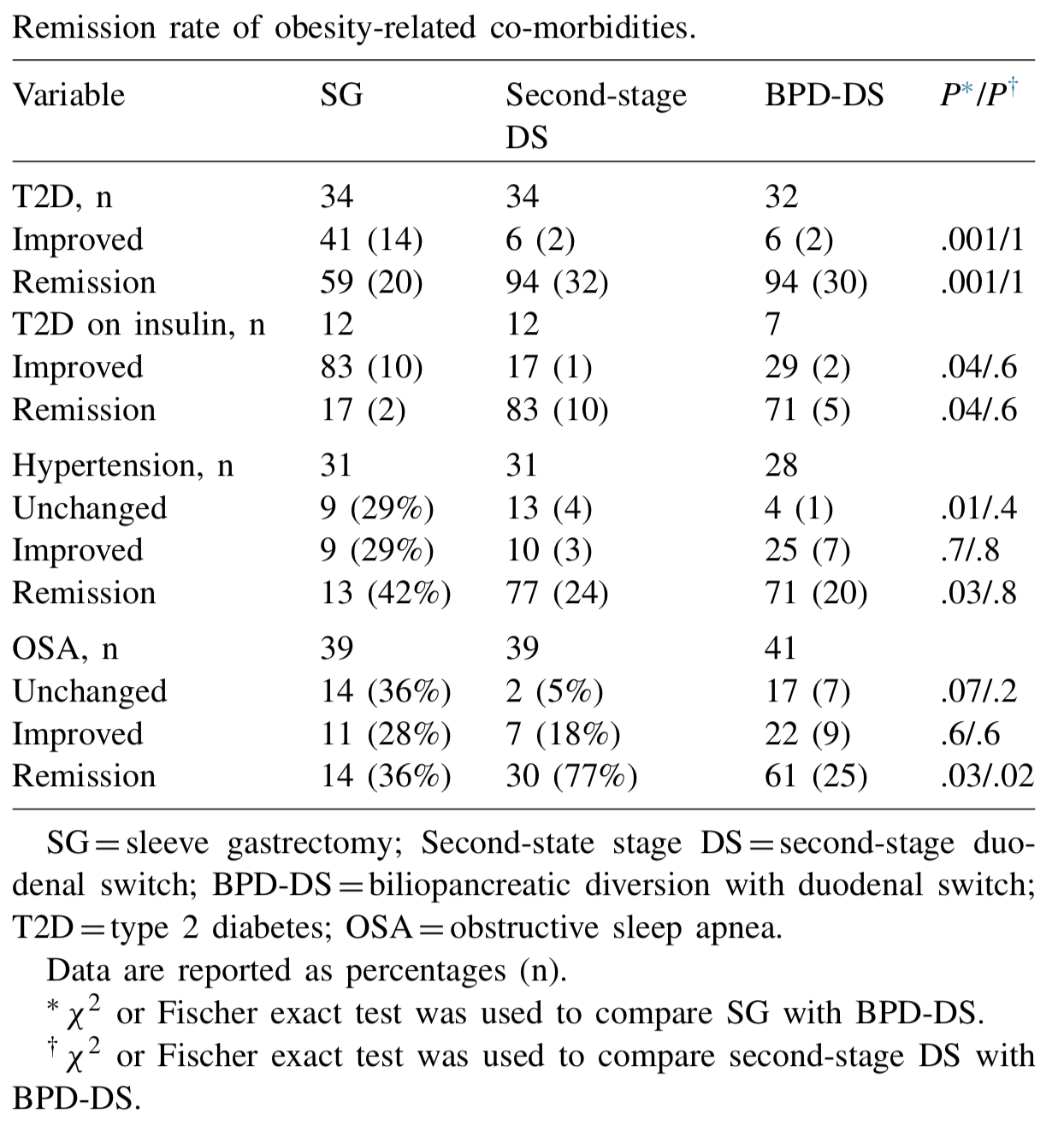
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss. 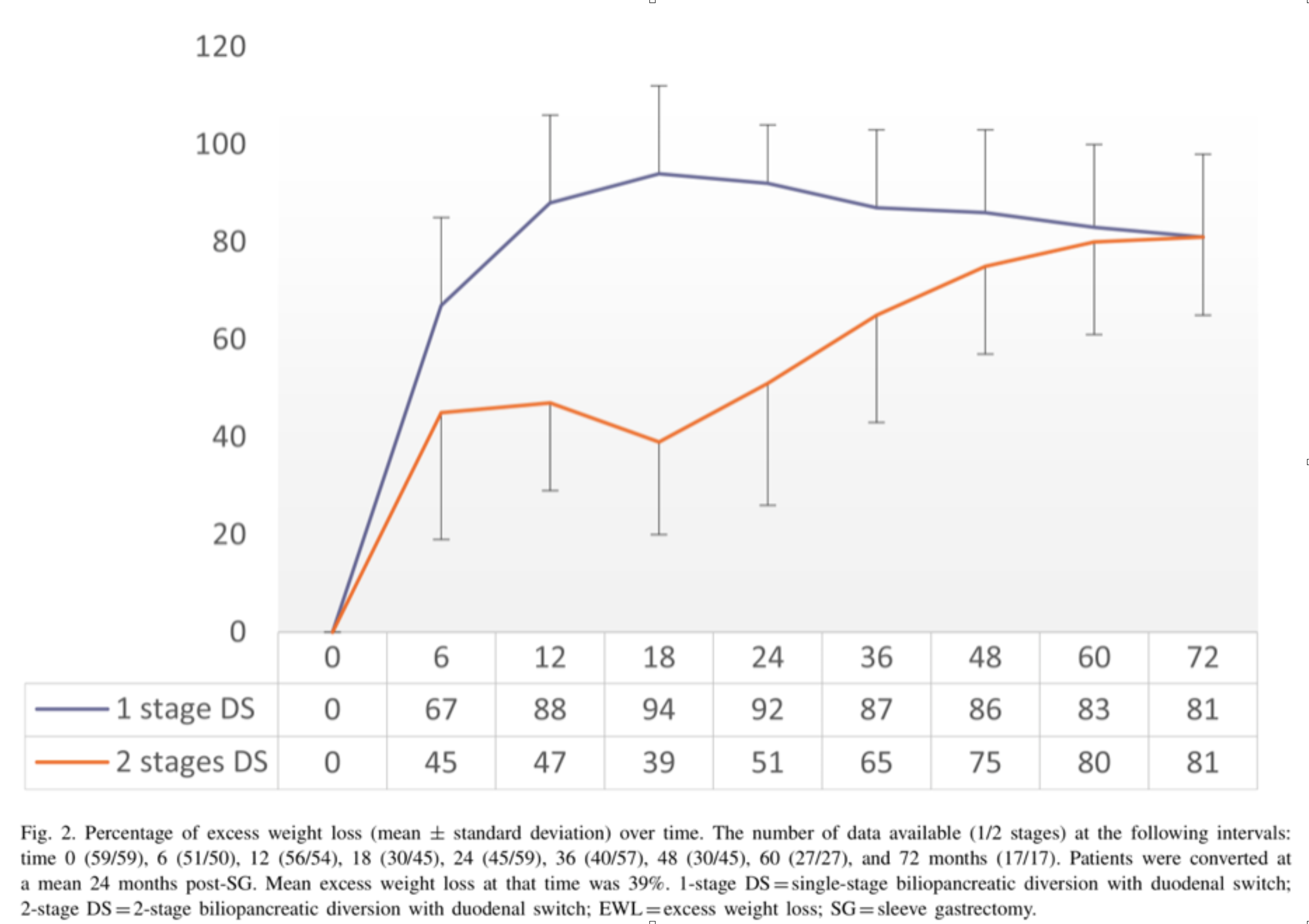
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.
Dr. Facebook
March 22, 2019 8:24 am
We have become reliant on the information that we obtain from the internet, specifically platforms such as Facebook. In our practice we have to continuously correct information that patients have obtained from other patients, unmonitored sites, blogs, and postings. Most of this information is based on individual experiences that has become gospel. “Fat is good for you” is one of them. To clarify, some health fat (olive oil, avocado, Omega 3) is healthy and needed for all patients. We do not recommend “fat bombs” as a part of ones daily dietary intake.
The following article was written on the accuracy of nutritional posts in support groups on Facebook.
Koalall et. all in SAORD, December 2018 Volume 14, Issue 12, Pages 1897–1902 published
“Content and accuracy of nutrition-related posts in bariatric surgery Facebook support groups”
The conclusion, as suspected, that “Over half of the posts contained inaccurate content or information that was too ambiguous to determine accuracy..:”

It is our recommendation before any dietary recommendations are taken from facebook and the like, the source of the information should be verified. As I have stated in the past, a frequent flier passenger is probably not qualified to fly a
commercial airplane, any more than a previous weight loss surgical patient providing medical and nutritional advice. We realize that there is significant value to the forum for exchange of information and sharing of experiences with other weight loss surgical patients as long as the information is well sourced and verified.

Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

Shared Success- Samantha had a Sleeve to Duodenal Switch Revision
July 14, 2017 9:30 am
After struggling with obesity for most of my life I was finally fed up. I had heard about weight loss surgeries before but was always under the common misconception that it was for people who wanted the “easy” way out of a hard situation. I had been working out and reducing calories and tried every popular diet and trainer you could think of. I was still huge and each time I would stop one of these extreme programs I would only end up larger than I was before.
My husband’s cousin had the sleeve surgery and she raved about it. Watching her success is what started to open my mind to surgery, but I was only considering the sleeve gastrectomy. I went to a center in another state that offers Duodenal switch, lapband, RNY and the sleeve. The surgeon I met with strongly suggested RNY to me, but I was stuck on the sleeve. I didn’t want my intestines touched period. I had the sleeve surgery on October 9, 2013.
My high weight was 402 lbs and I weighed 343 on the day of my sleeve surgery. I actually did well with the sleeve and was able to get down to 218 as my lowest. However it was still much like dieting. It was so stressful. After a while my body wouldn’t drop the weight regardless of how little I ate and exercised. I was eating 800-1200 calories a day and low fat meals and working out and kept slowly gaining weight. I was frustrated and honestly I gave up. My reflux wouldn’t go away so I visited a bariatric surgeon in my area who suggested that we essentially re-do the sleeve surgery to make my sleeve small again so that I would eat less and lose weight again. I got a second opinion and that surgeon suggested I revise to RNY. I went to obesity help’s website to explain my situation and a lot of people with much more experience than me HIGHLY urged me to see Dr Keshishian before making a decision. He was said to be an expert in revision weight loss surgery. I almost cancelled my appointment and didn’t have hope with this doctor either, but since I was in a dead end I went anyway. Dr Keshishian told me it wasn’t my fault. WHAT!? I had never heard that before. I usually get the shame from doctors who assume I must not be trying or that I am secretly eating something wrong. He ordered tests and told me it was “simply science” and I just LOVED him! I had a stricture in my Sleeve that needed to be repaired so since I needed surgery anyway I decided to go ahead and revise to a surgery that has the highest success rate, Duodenal Switch.


I was so scared of my intestines being cut and Dr. Keshishian eased my fears. I wish I had went that route the first time but then I might not appreciate it like I do now. Duodenal switch is the ONLY surgery I would recommend to anyone. As Dr K says it’s simple numbers. It’s the surgery with the highest percent of excess weight lost and kept off. I was 252 before my revision from Sleeve to Duodenal Switch and I am just at a year out and today I weigh in the low 190’s and I am still losing. Dr K’s goal for me was about 180. My goal is about 175. I eat more fat now than I ever did even when I was 400 lbs. I enjoy what I eat and I enjoy exercising and most of all I get to enjoy seeing results from my hard work. Food no longer causes me stress and anxiety. I know with 100% certainty that I made the right decision. Thank you Dr. K for your great skill and I don’t mean just with the knife but with the way you are able to make a high anxiety situation seem like no big deal.


Review & Update Giveaway!
August 31, 2016 6:27 pm


The Prize winners are Jo and Kimberly! Congratulations ladies and enjoy the Obesity Help National Conference! Thank you to all that participated in the Giveaway!
We are holding a review and update giveaway for two different prizes! Thank you for your
participation!
One Prize and One Grand Prize
Prize: two tickets to Obestiy Help National Conference Sept. 30-Oct 1, 2016
Grand Prize: two tickets to Obesity Help National Conference and one night
hotel stay October 1, 2016
Conference: 11999 Harbor Boulevard Garden Grove, California 92840 Event link here
Hotel Prize: SHERATON GARDEN GROVE – ANAHEIM SOUTH HOTEL
12221 Harbor Boulevard
Garden Grove, California
Official Rules:
How to Enter and eligibility: All entrants and winners must be 18 years of age or older at the time of entry. Up to 5 entries per person.
- Write a review of Dr. Ara Keshishian on one or all of the sites below or do an update on your profile on Obesity Help between now and Sept. 8, 2016 at 5:00 PM
2. Take a screen shot of the review or update with your username and date.
3. E-mail the screenshot to [email protected] with your contact information (name, phone number, e-mail, and mailing address )
4. Entries must be a verifiable patient of Dr. Ara Keshishian in Glendale, CA.
Promotion Timing:
The Review & Update Giveaway begins September 1, 2016 and ends September 8, 2016 at 5:00pm PST
How Winners are Chosen:
Winners will be chosen by random draw. Odds of winning vary upon the number of entries received for the giveaway.
Winner Notification and the Claiming of Prizes:
Winners will be notified via the email provided at time of entry and also published on our blog comments www.dssurgery.com/blog and on our FaceBook page. The winner will have 72 hours to respond to the winning notification email or the prize will be forfeited. The prizes have no cash value. The prizes are non-transferable and must be accepted as awarded. No changes may be made to the prizes. There is no cash value for the prizes.
General Conditions:
By entering the Giveaway, entrants agree to abide by and be bound by these Official Rules and the decisions of the Sponsor, which are final and binding in all matters relating to the Giveaway, and release and hold harmless Sponsor and its affiliates, directors, officers, employees and assigns from and against any liability, claims, lawsuits, judgments, losses, damages of any kind, injuries, death, property damage, costs and expenses, arising from, resulting from or in connection with the Giveaway, the participation in the Giveaway, or the receipt, possession, use or misuse of any prize. Sponsor is not responsible for lost, late, incomplete, inaccurate, stolen, delayed, misdirected, undelivered or illegible entries or for lost or stolen entry boxes or other errors or difficulties of any kind whether human, mechanical, electronic, typographical, printing or otherwise relating to or in connection with the Giveaway, including, without limitation, errors or difficulties which may occur in connection with the administration of the Giveaway, the processing of entries, the announcement of the prizes, or in any Giveaway-related materials. Sponsor is not responsible for technical, hardware, software or telephone malfunctions of any kind, lost or unavailable network connections, or failed, incorrect, incomplete, inaccurate, garbled or delayed electronic communications caused by the user or by any of the equipment or programming associated with or utilized in the Giveaway. Persons who tamper with or abuse any aspect of the Giveaway or who are in violation of these Official Rules, as solely determined by Sponsor, will be disqualified and all associated entries will be void. The Sponsor reserves the right, at its sole discretion, to cancel, terminate, modify or suspend the Giveaway if, in Sponsor’s opinion, it is not capable of running as planned, including, but not limited to, due to tampering, unauthorized intervention, fraud, technical or phone line failures or any other problems beyond the control of the Sponsor, and select the winners for affected drawing(s) from among all eligible entries timely received for such affected drawing(s) prior to cancellation.
Don’t lose your Pyloric Valve over a Failed Gastric Sleeve
June 22, 2016 9:32 am
In my opinion, there are very few reasons to lose your Pyloric Valve after sleeve gastrectomy. Recently, I am hearing of people who have had regain due to a failed Sleeve Gastrectomy being revised to Gastric Bypass RNY and then seeking a Duodenal Switch due to regain from Gastric Bypass RNY. A better option is to go from Sleeve Gastrectomy to Duodenal Switch, due to the long term excess weight loss maintenance of Duodenal Switch. The benefit of the pyloric valve can not be taken lightly.
Let’s start by reminding ourselves as to how the Sleeve Gastrectomy has gained popularity. In the quest for a simple solution to the complex problem of obesity, adjustable gastric banding gained popularity only fail to deliver anything close with the results that were promoted and heavily marketed. The focus was then changed to another seemingly simple procedure, laparoscopic sleeve gastrectomy. For some surgeons this is a new procedure. Surgeons that had been doing the duodenal switch operation for decades, sleeve gastrectomy has not been a new procedure. Surgeons that just started doing sleeve gastrectomy as a stand alone procedure started experiencing complications of the sleeve gastrectomy, such as regain and are now looking for another option for these patients. This complication are even more frequent when they’re done following a failed adjustable gastric band procedures due to the metabolic issues after revising one weight loss surgery to another. A similar short sighted approach is also being promoted with SIPS/SADI procedures, which is significantly simpler to perform than the duodenal switch operation.


Laparoscopic sleeve gastrectomy has a predictable profile for weight loss. It will not have as good on the long-term success rate as a duodenal switch operation. Complications of the sleeve gastrectomy including reflux, stricture, fistula, inadequate weight loss which may warrant evaluation and possible intervention. In my opinion, as a surgeon who does the duodenal switch operation routinely, a sleeve gastrectomy requiring revision should almost never be revised to a gastric bypass. I have seen number of patient’s who have had an adjustable gastric banding which was revised to the sleeve gastrectomy then to a gastric bypass. We are contacted for a possible revision to Duodenal Switch operation because of the weight regain. One can argue that the patient should not have had the sleeve gastrectomy or gastric bypass. It is critical that the complexity of the disease of the obesity is clearly appreciated that it purely restrictive procedure will not yield the desirable outcome long-term.
Benefits of the Pyloric Valve:
The pylorus is the valve located at the end of the stomach. It controls the release of the liquid mixture of food from the stomach into the small intestine.
The body naturally regulates the passage of food, so food will stay in the stomach for a certain period of time. We believe it is very important to continue that feeling of fullness in between meals. As a result, one of the principle functions of the pyloric valve is to regulate the amount of food products released into the small intestine where they are absorbed. This helps prevent dumping syndrome and ulceration.
The bodies natural diameter of stomach, pyloric valve and small intestine is left intact. This elevates stretching of the stomas created by RNY Gastric Bypass.
Summary
These failed Sleeve Gastrectomies should be revised to Duodenal Switch unless there are overwhelming health issues that would require another option. I always suggest several opinions from different Bariatric Surgeon’s who do a variety of Weight Loss Surgeries before deciding which type of revision to proceed with.