Category: SIPS
SIPS-SADI and ASMBS
December 31, 2023 1:21 pm
Vitamin D and Covid -19
May 07, 2020 9:24 am
We are all aware of the many roles that Vitamin D plays in our bodies. This includes immune function in addition to all the regulatory roles that Vitamin D plays in several physiologic reactions. There may be a correlation of low Vitamin D and COVID-19 infection increasing death risk as looked at in research articles.
Covid -19 in a subset of patience causes significant lung injury. These patients require mechanical ventilation.
Previously reported publications have suggested a possible correlation between ace inhibitors and increased risk of pulmonary complications of Covid -19. Some researchers suspect that the Covid-19 may be able to enter lung cells by the ACE receptors.
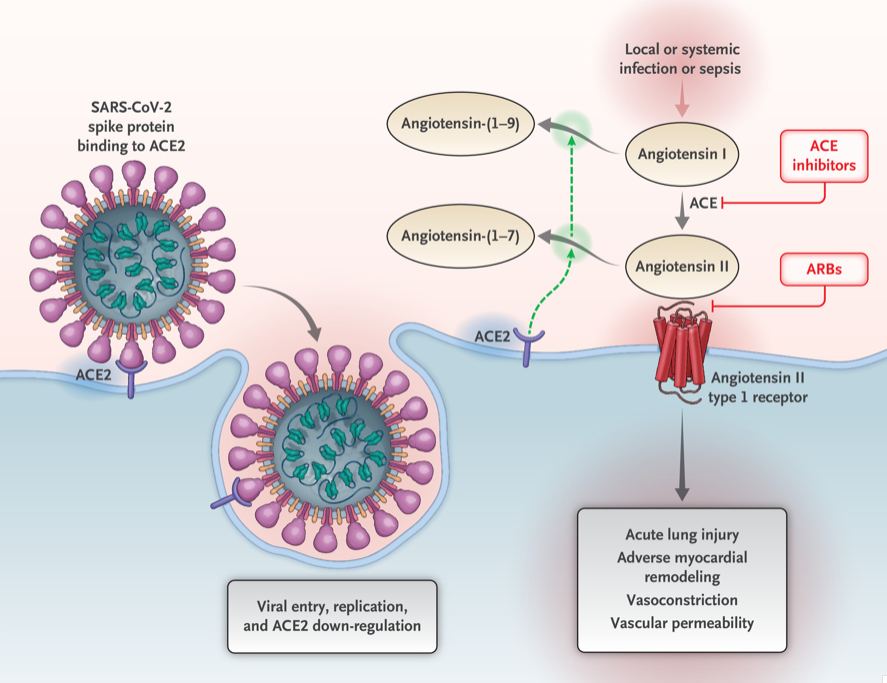
Vitamin D may positively implact the receptor ACE2. This study, report clear correlation between the high death rate with low vitamin D levels in Covid infected patients. There are limitation to this study that the attached abstract outlines.
Our take home message would be to please make sure you have updated labs and that you are all taking the recommended Vitamin D based on your surgical anatomy and laboratory values, not just an average non-bariatric person recommended dose.
https://www.dssurgery.com/wp-content/uploads/2020/05/manuscript.pdf
Articles
March 22, 2020 6:57 pm
Stapled Anastomosis
December 30, 2019 11:23 am
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
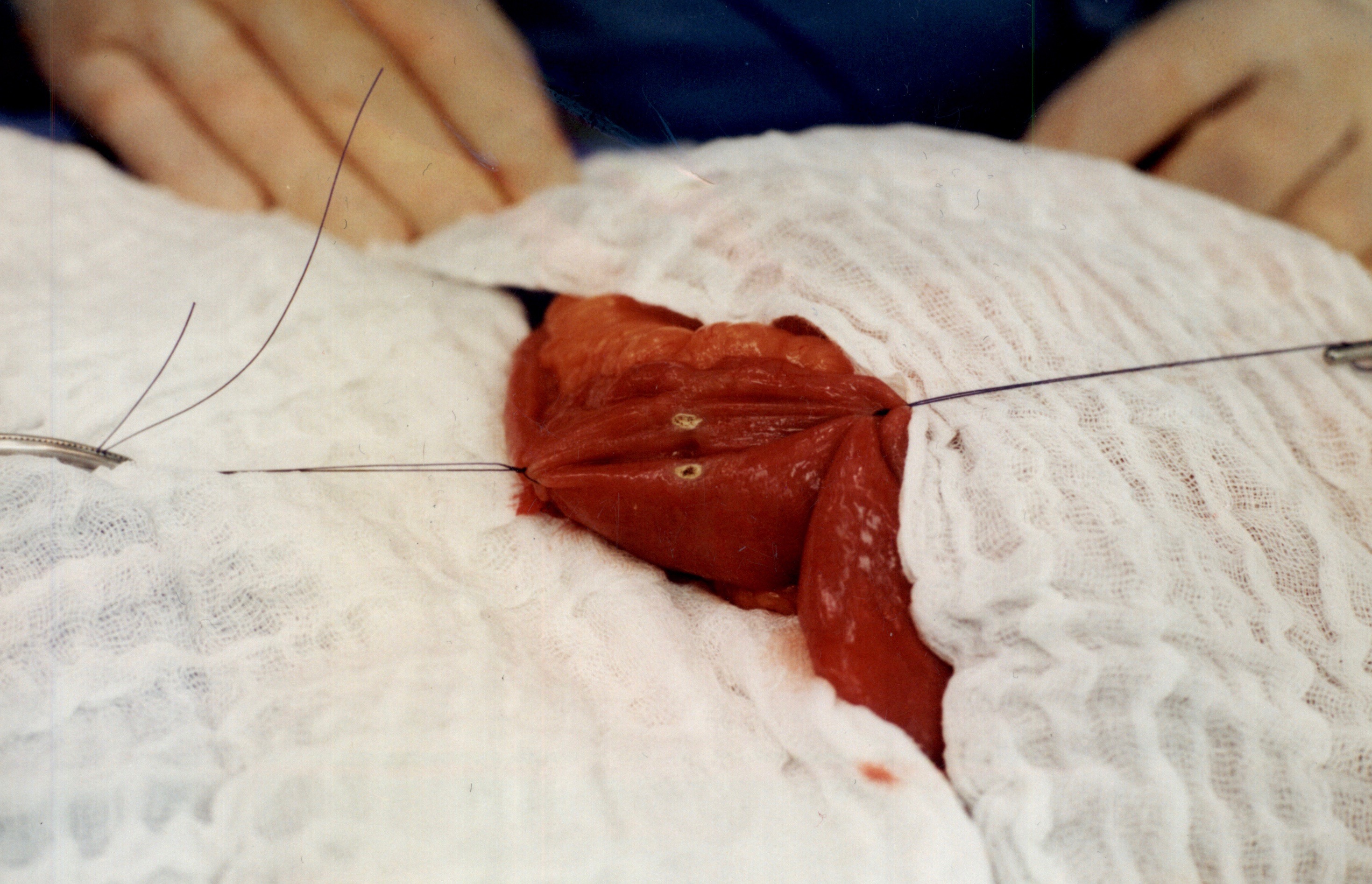
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
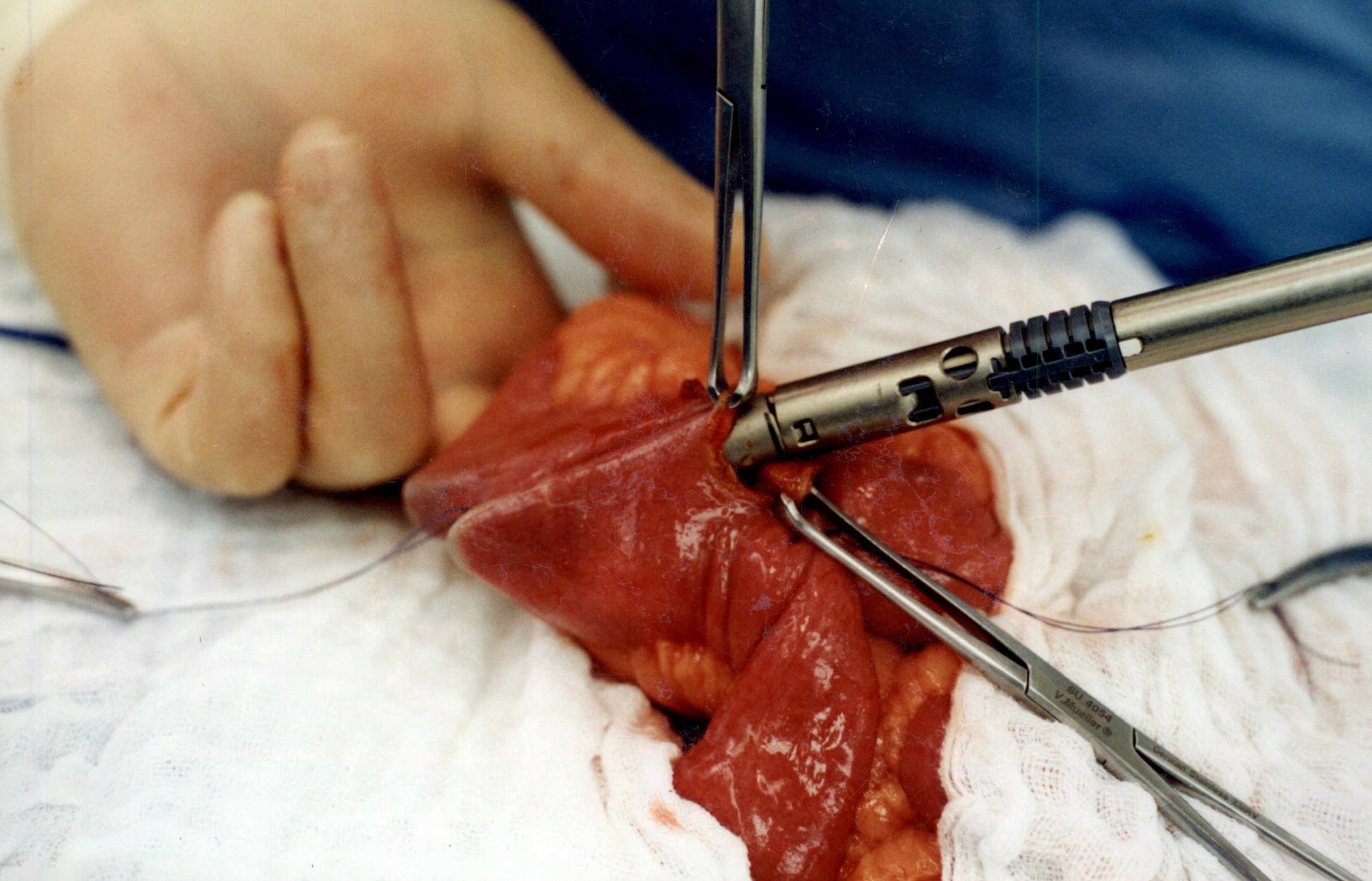
When the stapler is fired in opposite direction, a very wide anastomosis is created.
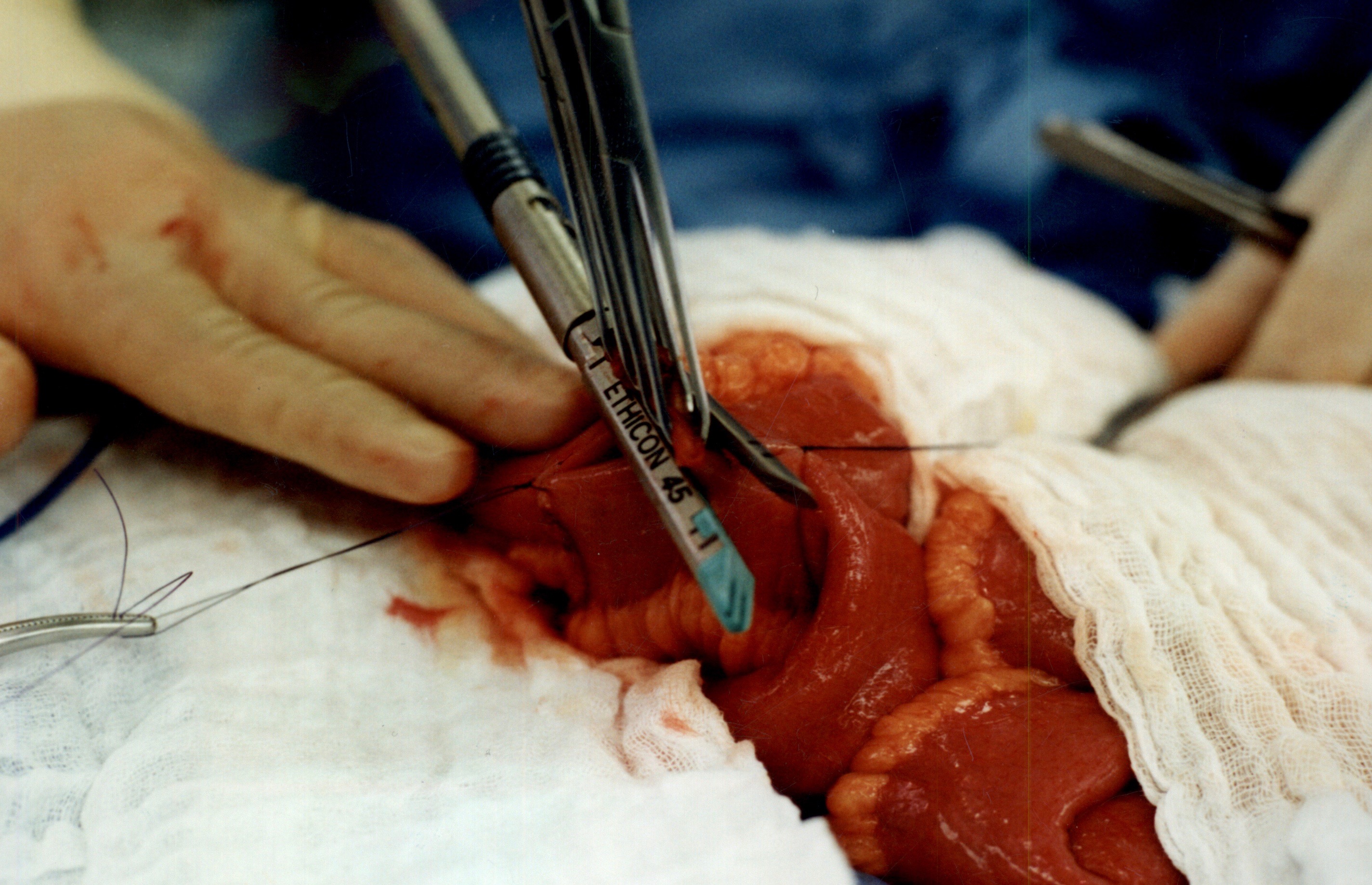
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Copper Deficiency Intravenous SupplementationExclusive Member Content
November 17, 2019 9:23 pm
Protein Intake
October 14, 2019 7:08 am
Protein intake requirements change over time following weight loss surgery. This is based on the requirements imposed on our body by a number of variables. These include, activity level, muscle mass, over all health condition to name a few.
A very young muscular athletic male with a BMI or 30 will require much higher protein intake (and absorption) that an inactive older Female with the same BMI. The same young athletic male will require much higher protein intake is he is recovering from a surgery than his baseline.
As we have stated in the past, the protein intake, should be adequate and not excessive. High level of protein intake that are not accounted for based on muscle mass and activity level, will eventually result in weight gain. The best measure of protein intake in a stable weight patient over 3-4 years post op is their albumin and protein level. Following your yearly laboratory values at a minimum is an important part of weight loss surgery follow up care.
You also need to adjust protein intake when necessary. Protein needs increase depending on physical needs, infection, healing, pregnancy, surgery, age, injury, etc. Plastic surgery requires higher protein needs for appropriate healing.
Information on protein sources and quality here.
The basic formula for protein intake is 1gm/kg of ideal body weight. The calculator below will provide a guide for the protein into based on your stable weight in lbs.
Thyroid Medication Absorption And Weight Loss Surgery
June 10, 2019 8:59 am
Question : “Do I have to take higher dose of thyroid medication after the duodenal switch? ”
Answer : “Maybe”
With all weight loss surgical procedures, there may be changes to absorption of medications. It is easily understood why duodenal switch may results in decreased absorption of fat-soluble medication. What is not as clear is the reduction in absorption of other medication with procedures that do not explicitly change the absorption at the level of the small bowel directly.
The research data is all over on this topic. There is published literature that shows improvement in the thyroid function after gastric bypass and the sleeve gastrectomy. However, the exact mechanism is not completely understood.
There is research that reports “…decreased postoperative levothyroxine requirements.” Other have shows no correlation between the length of the bowel distal to duodenum to absorption of thyroid medication.
With all this confusing data, the best course would be to always “treat the patient and not the lab results.”
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
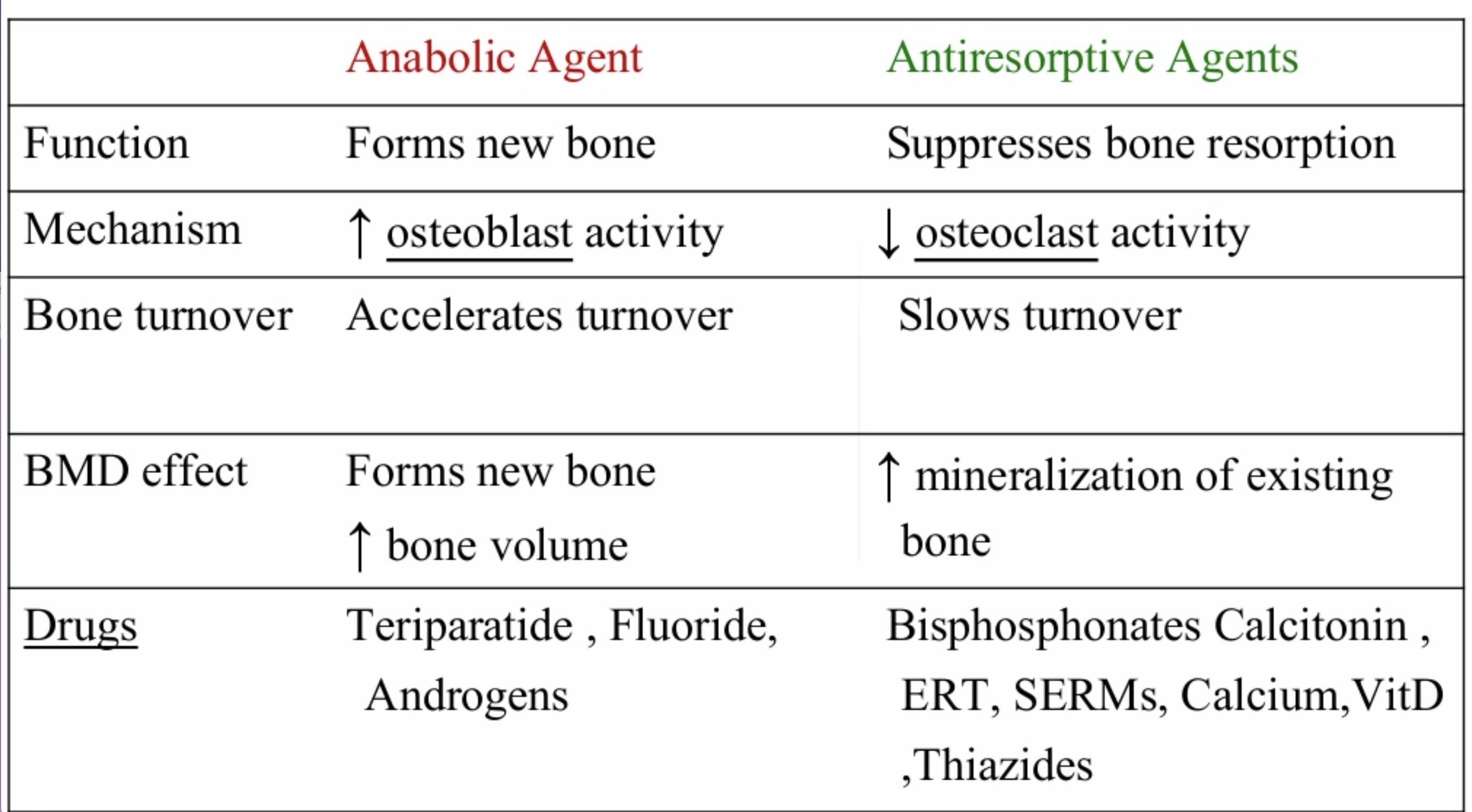
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
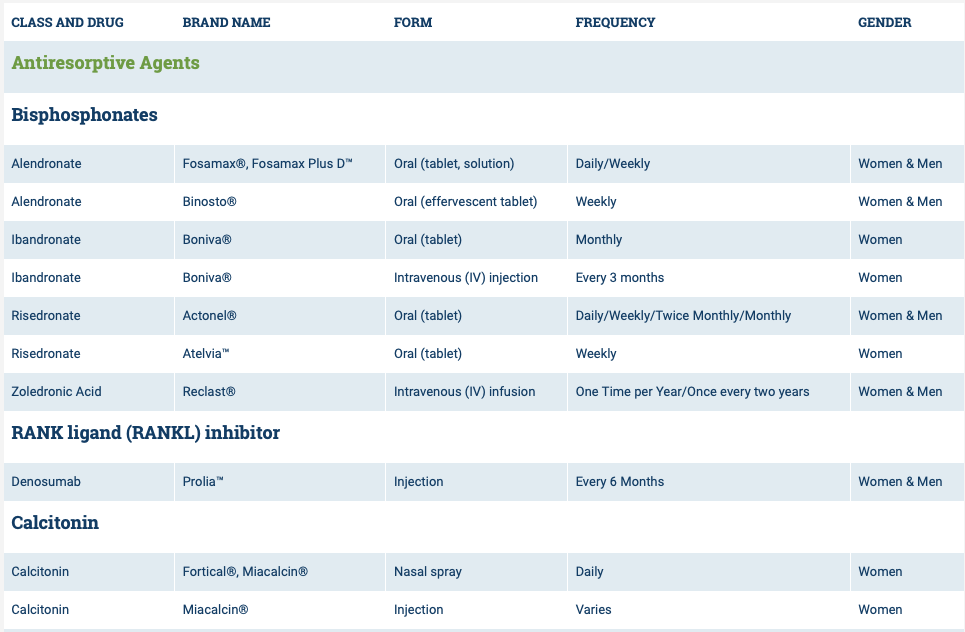
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

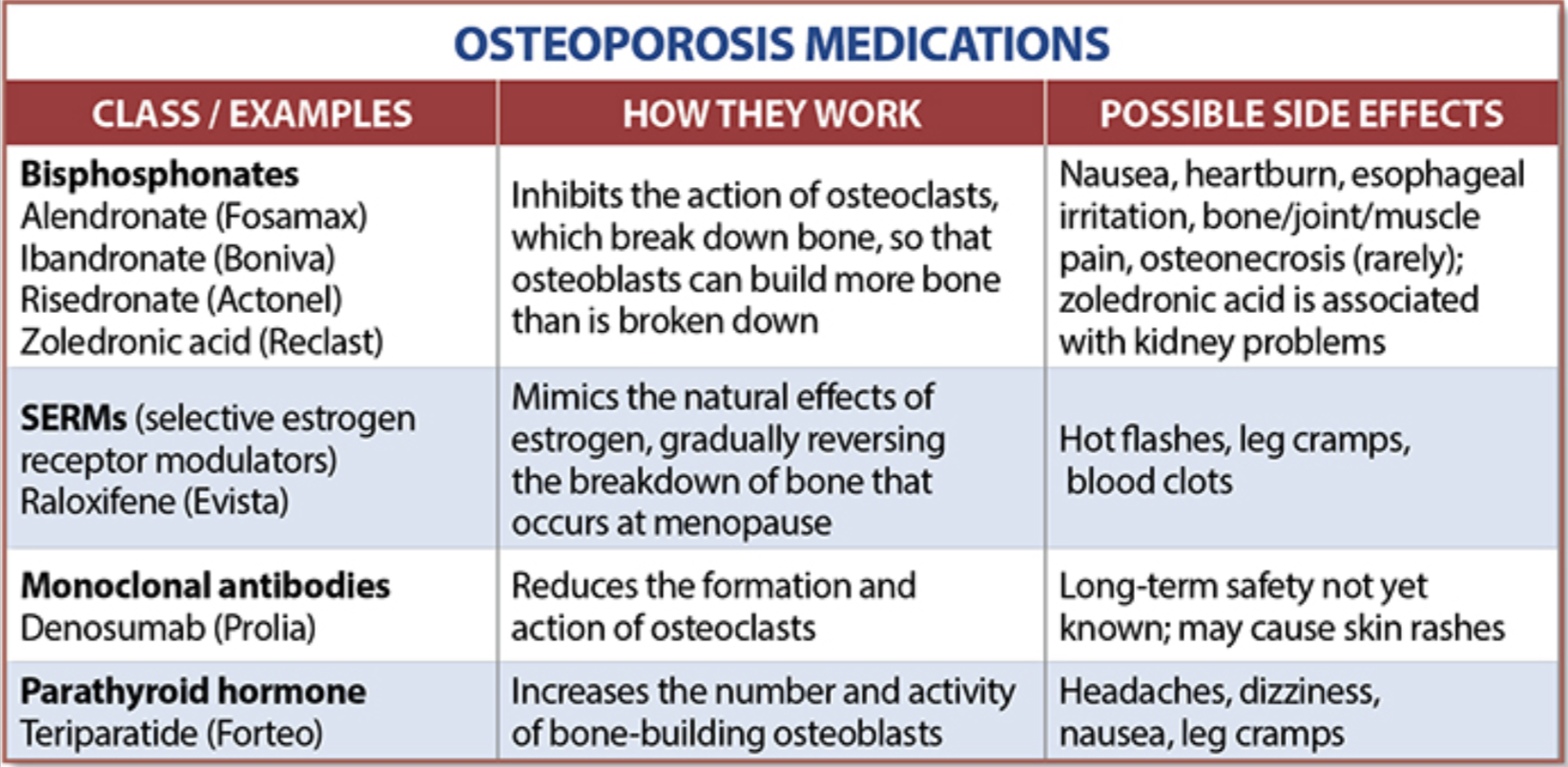
The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
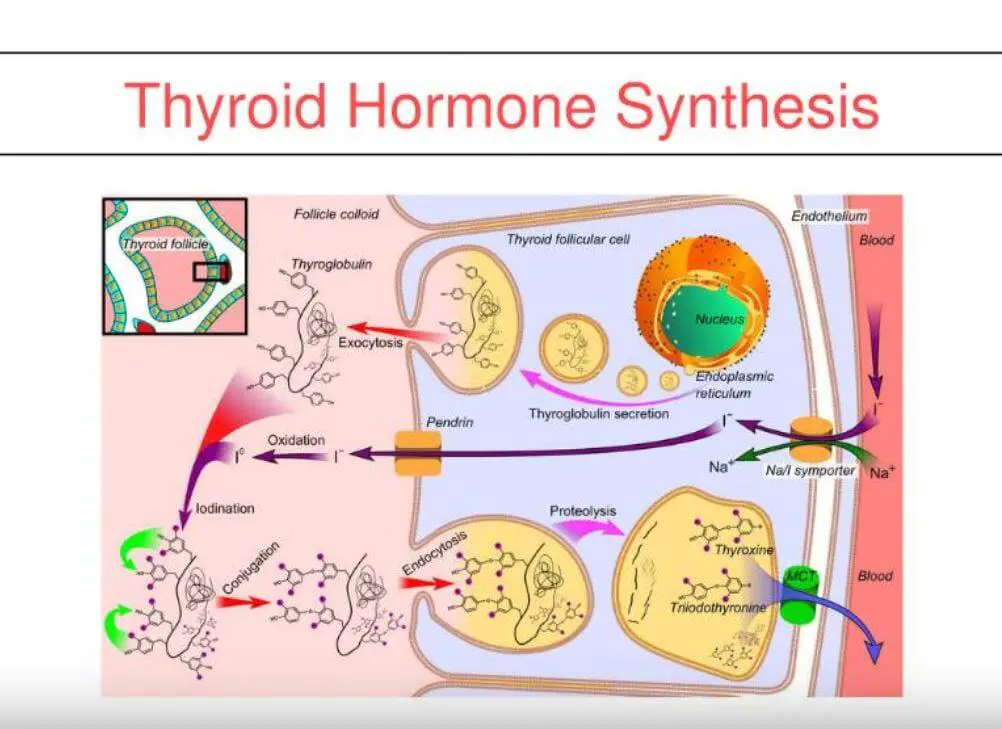
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
SIPS, SADI-S, Loop DS
May 01, 2019 9:03 am

The American Society for Metabolic and Bariatric Surgery (ASMBS) and MBSAQUIP-A on March of 2019, published and updated list of “Endorsed Procedures and Devices”
Endorsed Procedures and Devices | American Society for Metabolic and Bariatric Surgery
Note that any surgical procedures that does not employ two anastomosis, are not endorsed and are only recommended to be performed with an IRB (Institutional Review Board) or an IRB exemption. Duodenal Switch, Sleeve Gastrectomy, Roux en Y Gastric Bypass, Gastric Balloon, Adjustable Gastric Banding, and Nerve Blocking which are endorsed procedures.
SIPS, SADI-S, SIPS, Loop DS are all in the category of the “Non-Endorsed Procedures and Devices”. To see an anatomical comparison of these procedures to the Duodenal Switch procedure.
Patients should request that their consent be clearly defined and should explicitly outline the procedure that is being proposed to them. This is to avoid a patient having a procedure that they assumed, or are led to believe to be a Duodenal Switch operation with two anastomosis. Do your due diligence and know the procedure you want. Investigate if the surgeon you are working with performs the procedure you are interested in. Have them draw a picture of the procedure or give you a diagram of the procedure.
Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP