Category: malnutrition
Vitamin D level and Liver Function Test (LFT) elevation
February 08, 2026 11:21 am
After weight-loss surgery, some patients may experience a transient elevation in liver function tests that resolves over time. We have previously reported on this. IT is essential to distinguish between the Duodenal switch and the SIPS/SADI procedure, where some patients are led to believe they are identical. These procedures differ physiologically, and their weight loss and metabolic behaviours vary significantly.
Other than the stress of the weight loss, obesity, and comorbidities of obesity, there may be other anatomical post-surgical causes for elevated liver function test. This has also been discussed extensively.
A recent literature review supports the protective effects of vitamin D supplementation.
Elevated liver enzymes may be caused by many factors, including nutritional deficiencies, excessive supplementation (turmeric), medications, alcohol, adhesions causing partial bowel obstruction, and increased enterohepatic bile reabsorption . I would be very cautious about associating vitamin D supplementation with elevated liver function test results, even if the vitamin D level is in the very high normal range, regardless of the daily dose (much less frequent with injectable).
Vitamin D, as a fat-soluble vitamin, however, protects the liver and improves liver function test even in very high serum level . In rare cases, prolonged, elevated vitamin D levels may strain the liver. In Fact, the association of the vitamin D level and liver disease, including cirrhosis, leads to hepatocellular carcinoma (HCC) and dea h. Vitamin D protects the liver from HCC but cannot reduce the risk of cirrhosis.
Iron Supplements
July 29, 2025 1:30 pm
Iron is critical for the production and action of red blood cells. Deficiency of iron may have many causes. These include bleeding from the GI track, inadequate absorption, inadequate intake, and menstrual losses in females.
Regardless of the underlying cause, chronic deficiency of iron will lead to iron deficiency anemia (IDA).
Normal Iron Ranges:
It’s important to have at least yearly laboratory studies to surveil for abnormalities. Normal results of iron testing may be different for men, women, and children. Iron and TIBC are measured in micrograms per deciliter (mcg/dL). Normal results for iron are:
- 65 to 175 mcg/dL for men
- 50 to 170 mcg/dL for women
- 50 to 120 mcg/dL for children
Normal results for TIBC are 250 to 450 mcg/dL for men and women.
To correct or prevent IDA, iron supplementation is recommend in some patients. Iron absorption is very inefficient. It take a long time to develop IDA and as long if not longer to correct it with oral supplementation. This is why we recommend some patient condor getting iron infusion.
For most, oral supplements are adequate. There are different formulary of iron supplement with varying degree of absorption.
Heme iron and iron bisglycinate have been shown to have much better absorption than ferrous sulfate formulary.
This is why we recommend:


Cheers! Alcohol Metabolism
December 17, 2024 1:59 pm
Cheers! Let’s take a minute to look at alcohol metabolism. It’s that time of year when it seems we are going from one Holiday or Christmas party to another, and then we get together with the family and have a little more alcohol. The following diagram shows how alcohol metabolism takes place.
Alcohol is a caloric intake, and we all need to keep close tabs on it. Alcohol is very easily metabolized and the calories add up quickly. Every stage of alcohol processing in the liver involves the extraction of calories and free radicals, which are toxins. Excess calories not used in bodily functions can be stored as fat mass. Alcohol can be a roadblock in weight loss. Those drinks add up!


Here is a short video as a reminder while everyone waits to get ready for the next party.
Happy holidays.
A newsletter post from 2004 regarding the effects of alcohol and weight loss surgery.
Too Much Protein & Protein Metabolism
December 17, 2024 12:40 pm

Covid 19:Anesthesia, Weight Loss Surgery and Malnutrition
October 30, 2021 8:52 am
As the COVID-19 pandemic is charting its course into 2022, as health care providers, we have had to adapt and adjust to the transient and shifting environment. Testing for COVID-19 has been in place, and is now part of the standard for preoperative work-up. In addition, covid testing will likely be part of screening any surgical procedure for the foreseeable future.
The challenge of pandemic control is the large pockets of populations in the US and worldwide that do not have protection against the virus and are not vaccinated. Vaccination provides the only proven long-term protection against COVID-19 infection and its long-term persistent health effect. In addition, the complication rate reported in scientific journals is negligible compared to the complication and death rate from the COVID-19 infection.
There are implications of covid infection and general anesthesia published in peer-reviewed journals. The increased risk of general anesthesia after covid infection is related to the severity of the initial infection and the extent of the treatment required, and the persistence of the post covid symptoms, including shortness of breath, fatigue, and laboratory finding elevated inflammatory markers. Long after resolution of the acute COVID-19 symptoms, the most common persistent complaints are fatigue, shortness of breath, Joint and chest pain; and all these increase the risk of post-operative complications (Carfì et al., 2020)
The required delay for surgery may be as short as 2-4 weeks to as long as six months or longer if the persistent symptoms are present. Surgery may not be avoidable in a critical life-threatening situation and may be necessary even with a much-increased risk of complication (Collaborative, 2020). Recovery post-COVID-19 may not be complete with the resolution of the initial symptoms (Dexter et al., 2020)
Recent publications and scientific presentations have also shown the protection that weight loss surgery and maintained weight loss provide in those who come down with the COVID-19 infection (Aminian et al., 2021). However, the rate of weight gain, lack of weight loss is worse for weight loss surgical patients post COVID-19 disorder (Bullard et al., 2021; Conceição et al., 2021). Furthermore, patients with COVID-19 infection post weight loss are at a higher risk of malnutrition (di Filippo et al., 2021; Kikutani et al., 2021). Up to 40% of patients have malnutrition if hospitalized with COVID (Anker et al., 2021).
To summarize, Weight loss and weight loss surgery reduce the severity of the initial COVID-19 infection. However, it increases malnutrition risk, requiring nutritional support and surgical interventions in non-responsive cases.
REFERENCES:
Aminian, A., Fathalizadeh, A., Tu, C., Butsch, W. S., Pantalone, K. M., Griebeler, M. L., Kashyap, S. R., Rosenthal, R. J., Burguera, B., & Nissen, S. E. (2021). Association of prior metabolic and bariatric surgery with severity of coronavirus disease 2019 (COVID-19) in patients with obesity. Surgery for Obesity and Related Diseases, 17(1). https://doi.org/10.1016/j.soard.2020.10.026
Bullard, T., Medcalf, A., Rethorst, C., & Foster, G. D. (2021). Impact of the COVID-19 pandemic on initial weight loss in a digital weight management program: A natural experiment. Obesity, 29(9). https://doi.org/10.1002/oby.23233
Conceição, E., de Lourdes, M., Ramalho, S., Félix, S., Pinto-Bastos, A., & Vaz, A. R. (2021). Eating behaviors and weight outcomes in bariatric surgery patients amidst COVID-19. Surgery for Obesity and Related Diseases, 17(6).
Di Filippo, L., De Lorenzo, R., D’Amico, M., Sofia, V., Roveri, L., Mele, R., Saibene, A., Rovere-Querini, P., & Conte, C. (2021). COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clinical Nutrition, 40(4). https://doi.org/10.1016/j.clnu.2020.10.043
Kikutani, T., Ichikawa, Y., Kitazume, E., Mizukoshi, A., Tohara, T., Takahashi, N., Tamura, F., Matsutani, M., Onishi, J., & Makino, E. (2021). COVID-19 infection-related weight loss decreases eating/swallowing function in schizophrenic patients. Nutrients, 13(4). https://doi.org/10.3390/nu13041113
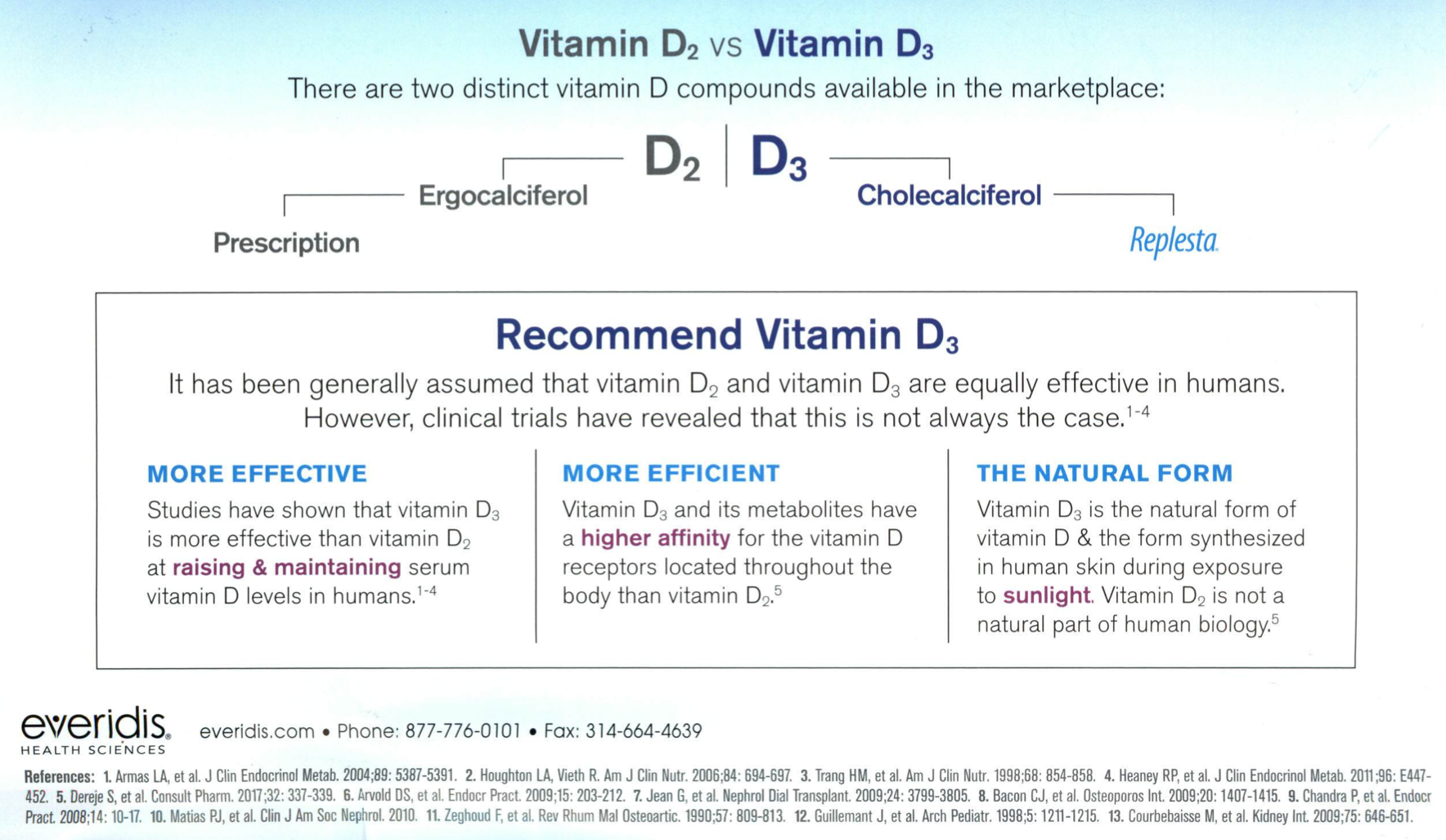
Over the Counter Vitmain D3 better than the Prescription Vitamin D2
August 30, 2021 10:41 am
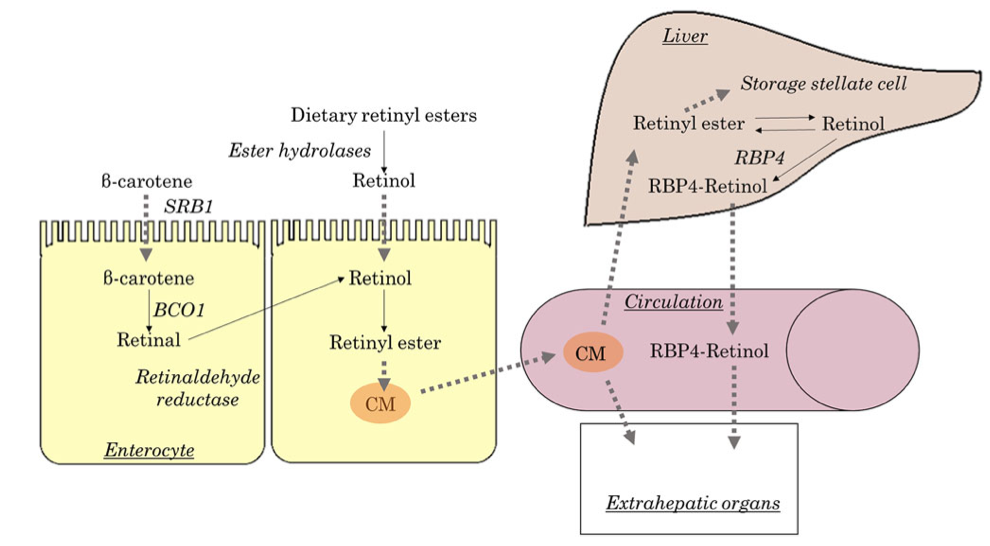
Vitamin A and Wound healing
December 21, 2020 9:37 am
Night Blindness – Vitamin A Deficiency
Nyctalopia (Night Blindness) An Early Sign of Vitamin A Deficiency with VideoA recent article discusses the types and function of vitamin A. As with the pandemic of COVID-19 continuous to stress our body and mind, we must stay vigilant with our nutritional status. Therefore, Vitamin supplements are critical in maintaining a robust immune system. For some, oral supplements are adequate; others may require injectable forms. If the oral supplements do not correct the vitamin A levels, please contact your primary care or our office to available vitamin A injections.
Fat Soluble Vitamins
April 26, 2020 10:20 am
Written By: Maria Vardapetyan, Eric Baghdasaryan, Osheen Abnous
Vitamins are chemicals that facilitate many processes in the human body such as blood clot formation, good vision, fight infections etc. There are two classes of vitamins. Water soluble vitamins and fat soluble vitamins. Water soluble vitamins dissolve in water. This makes it possible for them to be absorbed through all mucous membranes. Fat soluble vitamins on the other hand do not dissolve or pass through mucous membranes. Fat-soluble vitamins are absorbed in the intestine along with fats in the diet. These vitamins have the ability to be stored in the fat tissues of the human body. Water-soluble vitamins are not stored in the body and have to be taken in daily with the food and dietary supplements. Solubility of a vitamin is not a function of its physical state. There are fat soluble vitamins that have a liquid form and almost all of the water soluble vitamins come in form of pills or powders.
In this article, we are going to focus on fat soluble vitamins. They are all complex molecules made of carbon, hydrogen, and oxygen in different arrangements (see figures 1, 2, 3 and 4). These fat soluble vitamins are vitamin A, D, E and K.
Vitamin A
Vitamin A has a major role in vision, immune function, cell growth, and maintenance of organs such as heart, kidneys, lungs, etc. It plays a pivotal role in the health of our eyes, specifically the retina1. Rhodopsin protein, a major protein that has the leading role in the process of vision, is found in the retina where it allows us to perceive light. This protein requires vitamin A to function properly. Without vitamin A, rhodopsin cannot sense light and thus cannot initiate the process by which vision occurs.

Figure 1: Chemical structure of Vitamin A molecule
Vitamin D
Vitamin D regulates different chemical reactions that are associated with bones, muscles, and the immune system. The simplified way it does this regulation is it helps absorb calcium from dietary nutrients which in turn strengthens the bones, helps neurons exchange signals to move muscles and helps the immune system to fight against viruses and bacteria2.
 Figure 2: Chemical structure of Vitamin D molecule
Figure 2: Chemical structure of Vitamin D molecule
Vitamin E
Vitamin E acts as an antioxidant. Antioxidants are naturally occurring chemicals that neutralize toxic byproducts of many chemical reactions in the human body. When food is consumed and digested, the human body converts it into energy. As a result of metabolism free radicals (toxic byproducts) are formed and are neutralized with the help of vitamin E. In addition, free radicals are also in the environment. Furthermore, vitamin E stimulates the immune system to fight against bacteria and viruses3.
 Figure 3: Chemical structure of Vitamin E molecule
Figure 3: Chemical structure of Vitamin E molecule
Vitamin K
Vitamin K can be obtained from food and dietary supplements. There are two forms of vitamin K: phylloquinone (Vitamin K1), which is found in spinach, kale and other greens and menaquinone-4 (Vitamin K2), which is found in animal products. Vitamin K1 is involved in blood clotting, and Vitamin K2 is involved in bone tissue building. Vitamin K1 is the main Vitamin K in human diet (75-90% of all vitamin K consumed), however, it is poorly absorbed in the body4,5.

Figure 4: Chemical structures of Vitamin K1 and K2 molecules
Absorption of fat soluble vitamins
Polarity describes the inherent charge(positive or negative) or lack of charge for any given substance or molecule. Molecules that are charged are referred to as “polar”, while those that lack charge are “nonpolar”. When discussing solubility, it is important to remember the phrase “like dissolves like”. That means polar (charged) substances like to interact with a polar environment like water, since water contains a slight negative charge. Hence, charged substances are water-soluble. Nonpolar substances on the other hand readily interact with nonpolar environments such as fat, which contains no charge. Therefore, molecules that lack a charge such as vitamins A, D, E, and K are referred to as fat soluble.
Due to their water fearing nature, these fat soluble vitamins cannot simply be absorbed directly into the bloodstream (which is mostly water) like the sugars and amino acids in our diet. As their name suggests, these fat soluble vitamins like to be embedded in fatty droplets, which facilitate their absorption in the following way. Fat soluble vitamins group together with other fat molecules to form fatty droplets, effectively reducing the amount of interaction with the watery environment of the intestines. Therefore, without an adequate amount of fat in your diet, your body is unable to effectively absorb these fat-soluble vitamins. This may be true in an intact anatomy, however, post weight loss surgical patients can not increase their fat soluble vitamin levels by increasing their fat intake. This is due to the fact that a high fat diet causes excessive bowel movement which in turn washes away any vitamins taken by mouth. DS limits fat absorption (thus the great weight loss) which can cause vitamin A and D deficiency that can not be easily corrected with oral supplementation.
As mentioned before, fat soluble vitamins are hydrophobic and nonpolar, which means they are also fat loving or lipophilic. Excess fat soluble vitamins can be stored in the liver and fat tissue. Therefore, these vitamins do not need to be eaten every single day since stores of these vitamins can sustain a person for some time. It may take several weeks or months for our body to deplete these stores of fat soluble vitamins which is why it generally takes a longer amount of time for fat soluble vitamin deficiencies to manifest themselves. The ability to store these fat soluble vitamins in tissues can also lead to vitamin toxicity – marked by an excess of vitamin stores in our body.
Clinical manifestations of A, D, E, K deficiency
| Vitamin | Clinical Deficiency manifestations |
| Vitamin A | Vision Problems
Dryness of the eye |
| Vitamin D | Softening and weakening of the bones
Bone shape distortion Bowed legs (generally in children) Hypocalcemia |
| Vitamin E | Damage to red blood cells
Tissue/organ damage due to inability to supply enough blood Vision problems Nervous tissue malfunction |
| Vitamin K1 | Excessive bruising
Increased bleeding time Small blood clots under nails Increased bleeding in mucous membrane |
| Vitamin K2 | Weak bones
Increased plaque deposits along gumline Arterial calcification |
References
- Office of Dietary Supplements – Vitamin A. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/#. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin D. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminD-Consumer/. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin E. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminE-Consumer/. Accessed April 26, 2020.
- Vitamin K. The Nutrition Source. https://www.hsph.harvard.edu/nutritionsource/vitamin-k/. Published July 2, 2019. Accessed April 26, 2020.
- Beulens JWJ, Booth SL, van den Heuvel EGHM, Stoecklin E, Baka A, Vermeer C. The role of menaquinones (vitamin K₂) in human health. The British journal of nutrition. https://www.ncbi.nlm.nih.gov/pubmed/23590754. Published October 2013. Accessed April 26, 2020.
Copper Deficiency Intravenous SupplementationExclusive Member Content
November 17, 2019 9:23 pm
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
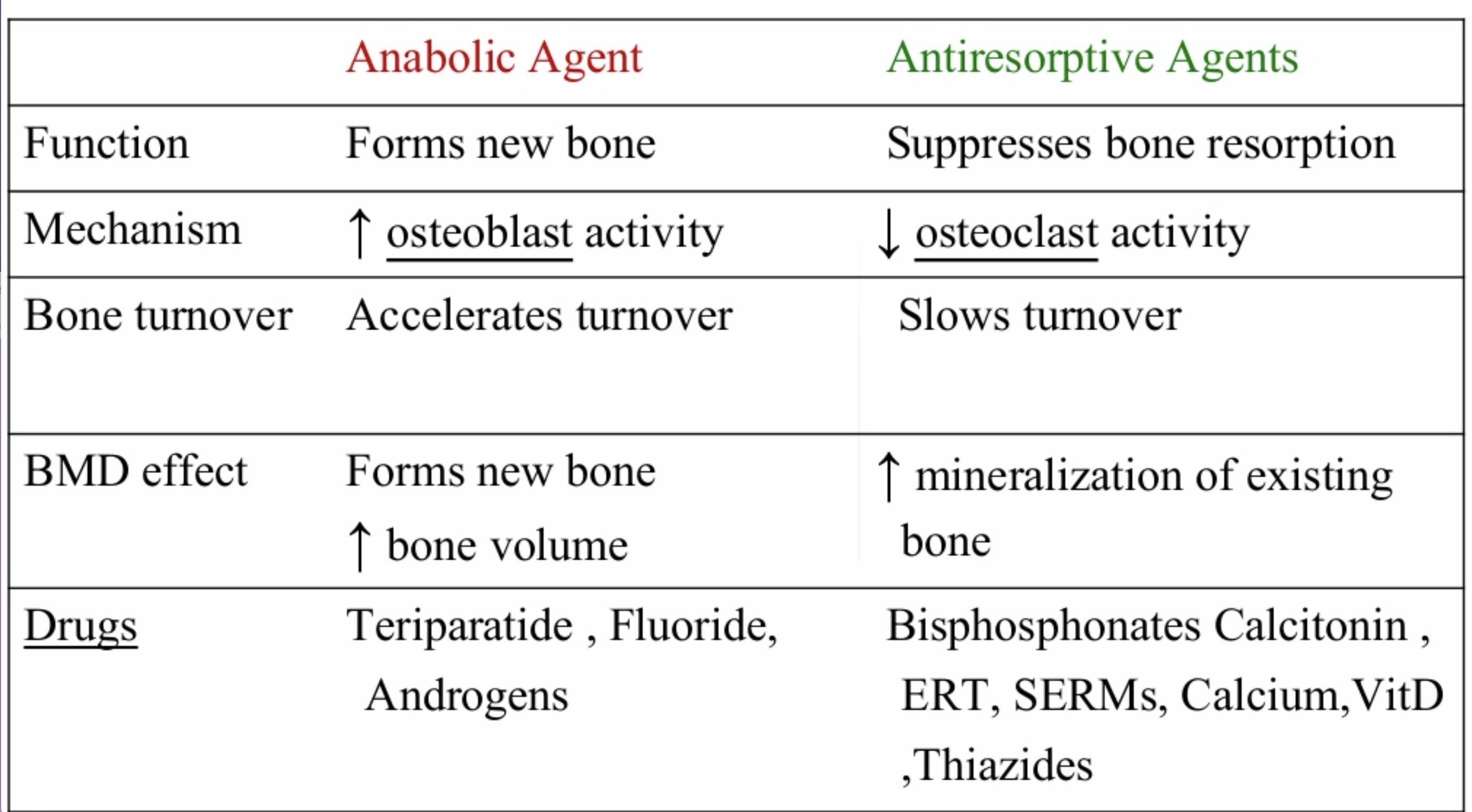
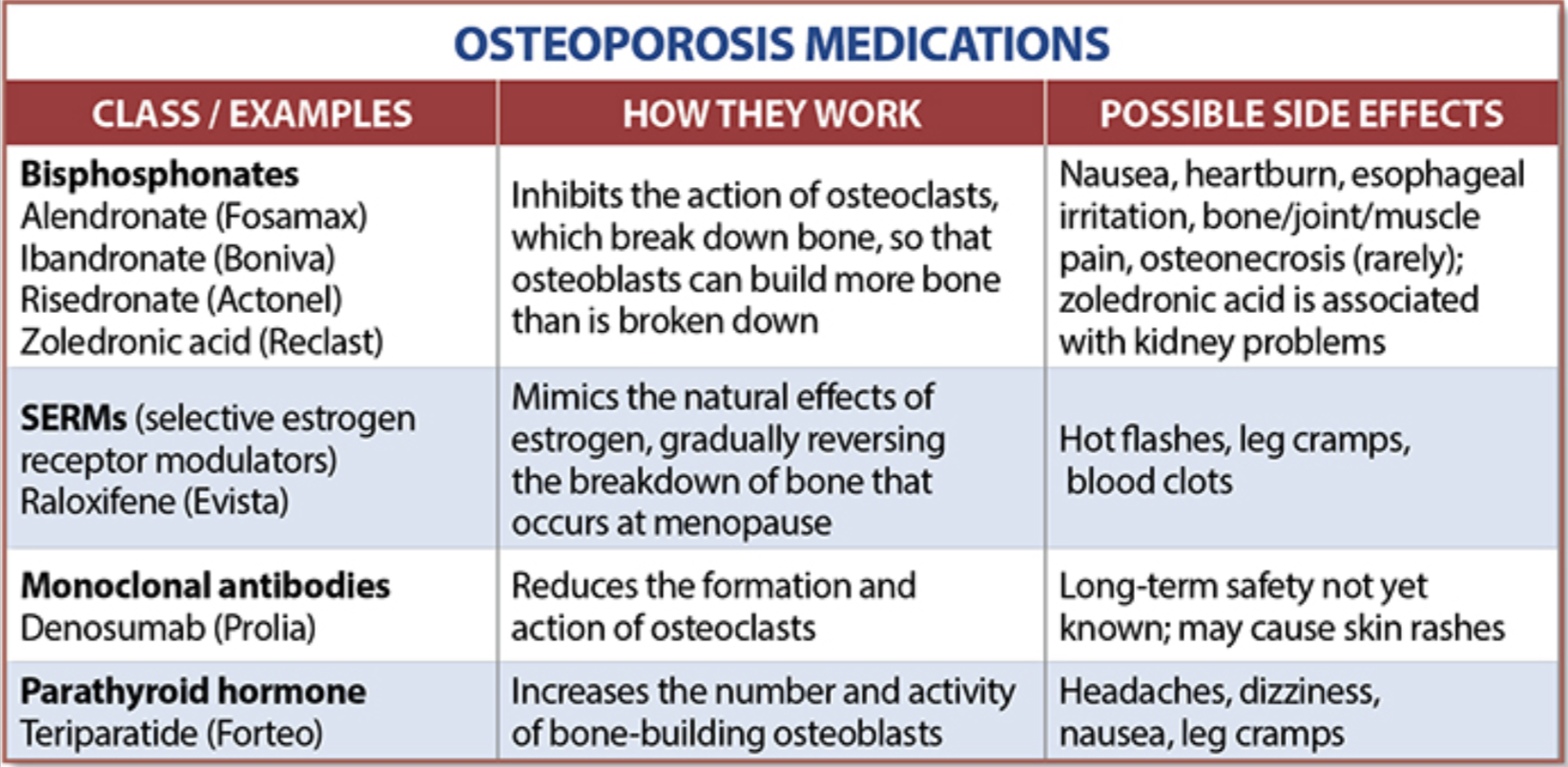
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.
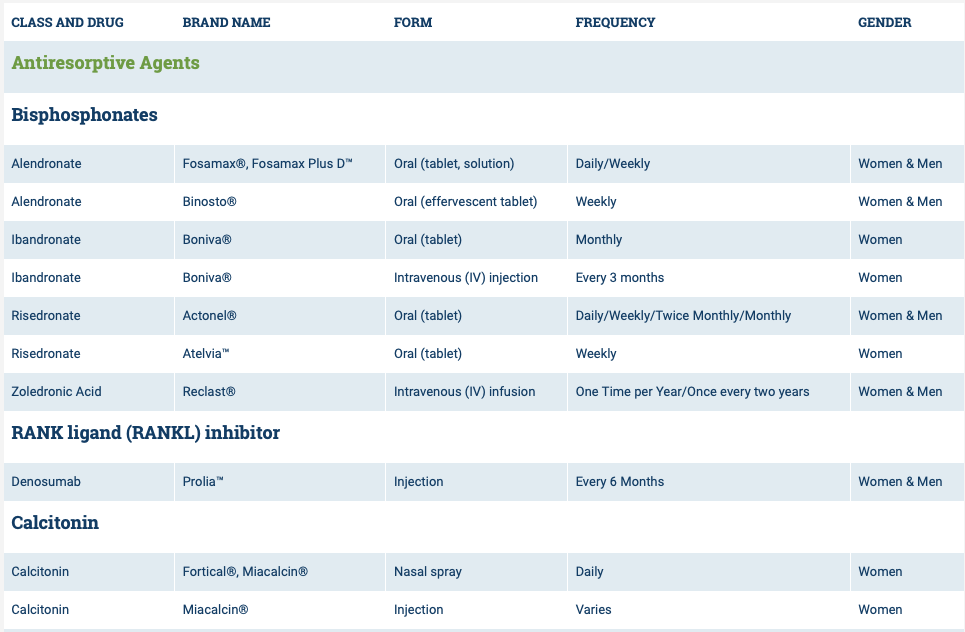

The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.