Category: Revision weight loss surgery
COVID Vaccines
March 05, 2021 3:50 pm
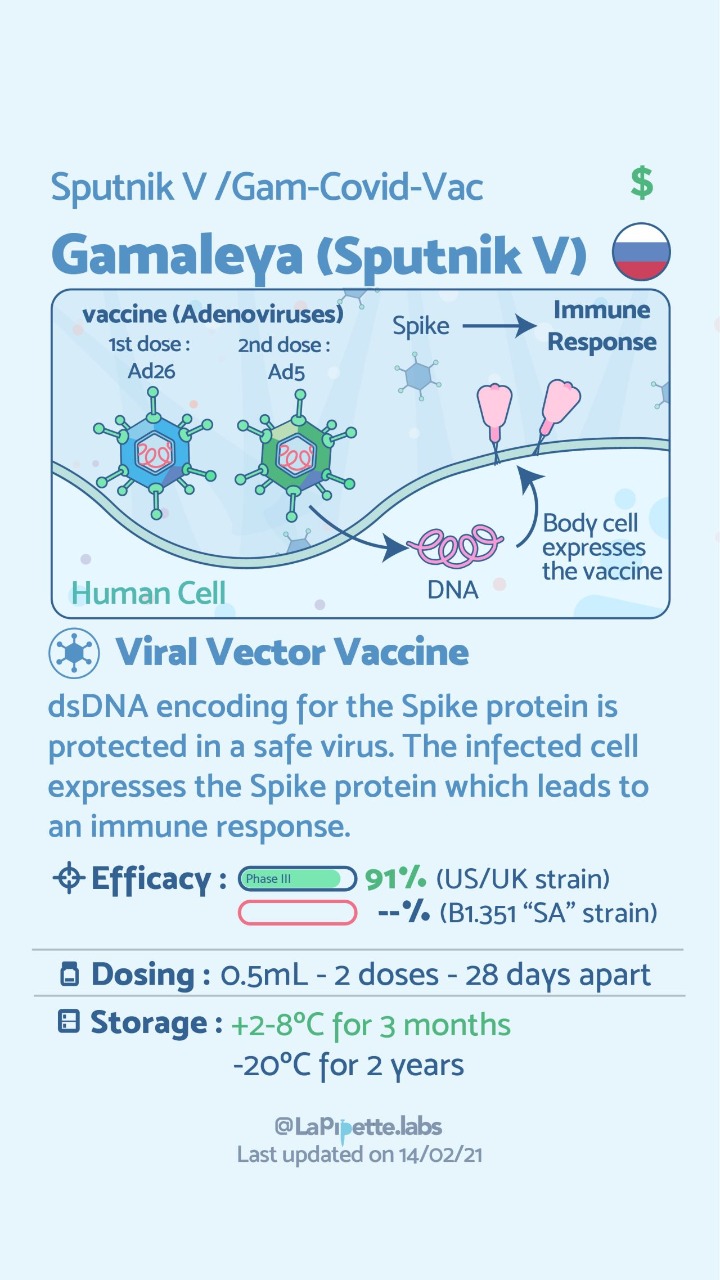
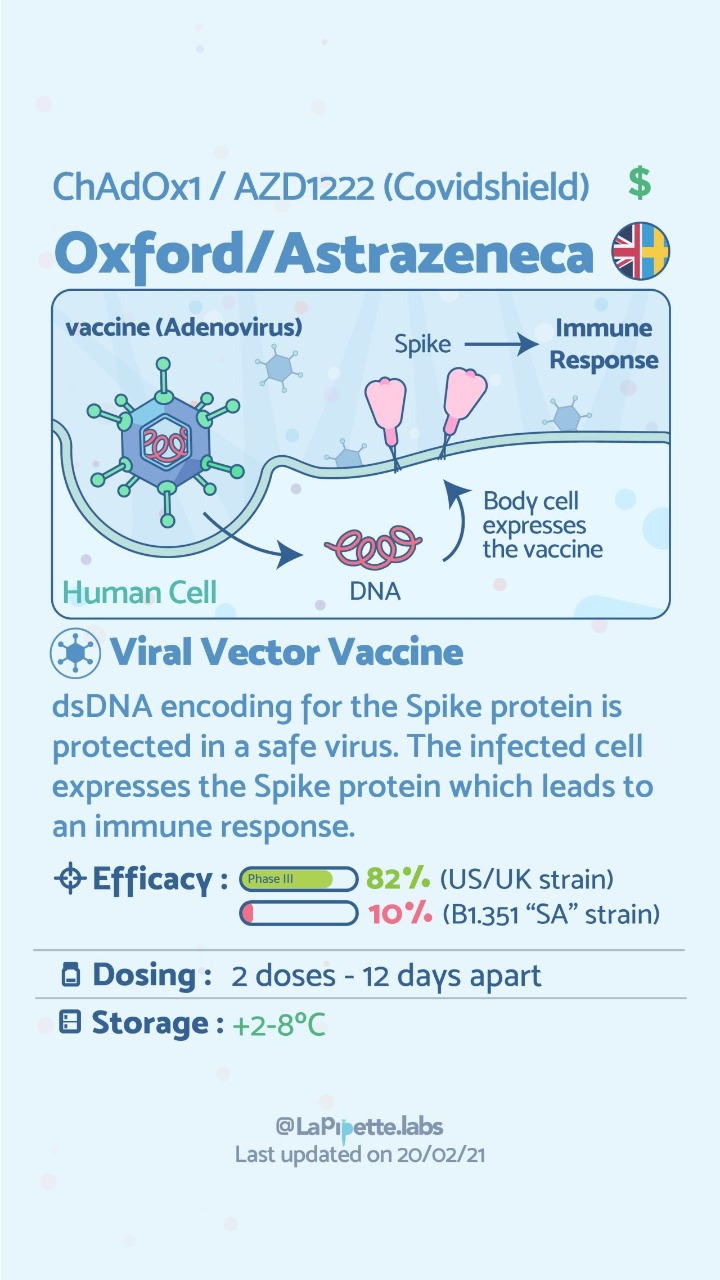
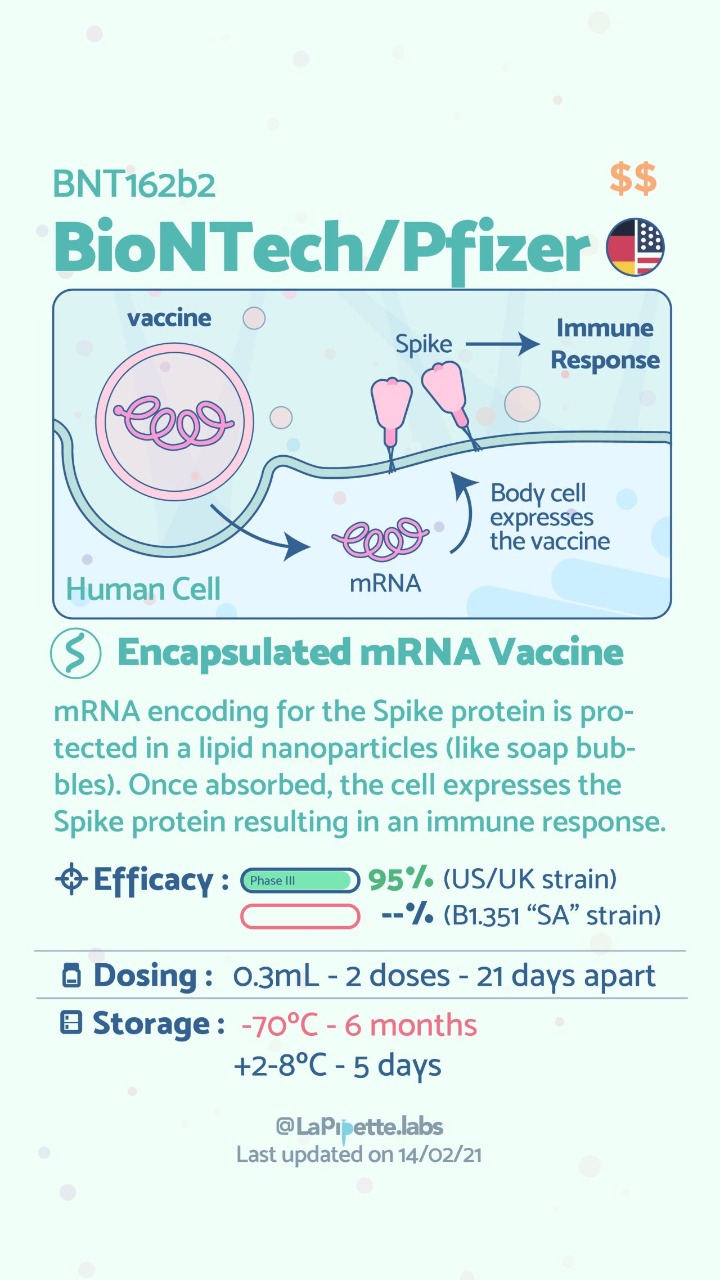
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
Sleeve And Weight Regain
July 22, 2019 9:50 am
Dr. Facebook
March 22, 2019 8:24 am
We have become reliant on the information that we obtain from the internet, specifically platforms such as Facebook. In our practice we have to continuously correct information that patients have obtained from other patients, unmonitored sites, blogs, and postings. Most of this information is based on individual experiences that has become gospel. “Fat is good for you” is one of them. To clarify, some health fat (olive oil, avocado, Omega 3) is healthy and needed for all patients. We do not recommend “fat bombs” as a part of ones daily dietary intake.
The following article was written on the accuracy of nutritional posts in support groups on Facebook.
Koalall et. all in SAORD, December 2018 Volume 14, Issue 12, Pages 1897–1902 published
“Content and accuracy of nutrition-related posts in bariatric surgery Facebook support groups”
The conclusion, as suspected, that “Over half of the posts contained inaccurate content or information that was too ambiguous to determine accuracy..:”

It is our recommendation before any dietary recommendations are taken from facebook and the like, the source of the information should be verified. As I have stated in the past, a frequent flier passenger is probably not qualified to fly a
commercial airplane, any more than a previous weight loss surgical patient providing medical and nutritional advice. We realize that there is significant value to the forum for exchange of information and sharing of experiences with other weight loss surgical patients as long as the information is well sourced and verified.

Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

Candy Cane Gastric Bypass – RNY
June 21, 2018 1:05 pm
One of the findings following Gastric Bypass is a Candy Cane Gastric Bypass. Nausea and vomiting , upper abdominal pain is a common complaint of patient who have had the Gastric Bypass RNY operation. This is in addition to the high incidence of patients who experience the complications of weight regain and or dumping syndrome.
Quite frequently the symptoms of nausea, vomiting and upper abdominal pain of a patient with history of gastric bypass is evaluated by a primary care, referred to a gastroenterologist. The “routine” work up recommended is X-ray of the abdomen, maybe contrast study (Ct scan or upper GI) and for sure and upper endoscopy. The result quite frequently reported as “…nothing wrong”.
A typical upper GI in a Candy Cane Gastric Bypass situation may look like this:

A common and underreported problem may be a Candy Cane finding. The “blind” end of the small bowel anastomosis is too long and this results in food settling in the hook of the candy cane. The symptoms of the nausea, vomiting and upper abdominal pain may be from the residual food and liquids that do not drain from this area.

Candy Cane Gastric Bypass finding

Candy Cane Gastric Bypass cases will require surgical intervention to shorten the length of the blind segment of the small bowel to improve symptoms.
It is my recommendations that any patient with history of weight loss surgery who is having any persistent gastrointestinal symptoms be evaluated by weight loss surgeon.
Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium
Revision from failed AGB to Duodenal Switch
January 10, 2018 2:10 pm
A few times a month during consultation for weight loss surgery , I’m ask as to why I do not offer the adjustable gastric banding as an alternative to the patients. As I have said over the years when a patient considers an weight loss surgery the totality of the risk should be considered. This includes the operative, immediate postoperative course, the maintenance and the follow-ups needed. The potential complications of the procedure in addition to the long-term success off each operation should also be taken into account.
Unfortunately, some patients are led to believe that any perceived benefit in the short operative time and the ease of the adjustable gastric banding also translates to a better outcome. This is in fact the opposite of what the published data have shown, a recent study published in April 2017 by Vinzes et.al, shows that 71% of patient lost their band by 10 years out.




What is also interesting that more patients underwent revision from failed AGB to the duodenal switch than the sleeve gastrectomy (Fig 1.). This is what I also recommend.
More importantly, The patients who underwent a revision from failed AGB to the duodenal switch operation had the best long term results of all patients (Fig 2.) note the “rBPD” line that is the highest of %EBMIL.
Complication’s were broad and frequent (Table 3.)
Further information on revision from failed AGB to Duodenal Switch or other failed weight loss surgeries can be found here.
Shared Success- Samantha had a Sleeve to Duodenal Switch Revision
July 14, 2017 9:30 am
After struggling with obesity for most of my life I was finally fed up. I had heard about weight loss surgeries before but was always under the common misconception that it was for people who wanted the “easy” way out of a hard situation. I had been working out and reducing calories and tried every popular diet and trainer you could think of. I was still huge and each time I would stop one of these extreme programs I would only end up larger than I was before.
My husband’s cousin had the sleeve surgery and she raved about it. Watching her success is what started to open my mind to surgery, but I was only considering the sleeve gastrectomy. I went to a center in another state that offers Duodenal switch, lapband, RNY and the sleeve. The surgeon I met with strongly suggested RNY to me, but I was stuck on the sleeve. I didn’t want my intestines touched period. I had the sleeve surgery on October 9, 2013.
My high weight was 402 lbs and I weighed 343 on the day of my sleeve surgery. I actually did well with the sleeve and was able to get down to 218 as my lowest. However it was still much like dieting. It was so stressful. After a while my body wouldn’t drop the weight regardless of how little I ate and exercised. I was eating 800-1200 calories a day and low fat meals and working out and kept slowly gaining weight. I was frustrated and honestly I gave up. My reflux wouldn’t go away so I visited a bariatric surgeon in my area who suggested that we essentially re-do the sleeve surgery to make my sleeve small again so that I would eat less and lose weight again. I got a second opinion and that surgeon suggested I revise to RNY. I went to obesity help’s website to explain my situation and a lot of people with much more experience than me HIGHLY urged me to see Dr Keshishian before making a decision. He was said to be an expert in revision weight loss surgery. I almost cancelled my appointment and didn’t have hope with this doctor either, but since I was in a dead end I went anyway. Dr Keshishian told me it wasn’t my fault. WHAT!? I had never heard that before. I usually get the shame from doctors who assume I must not be trying or that I am secretly eating something wrong. He ordered tests and told me it was “simply science” and I just LOVED him! I had a stricture in my Sleeve that needed to be repaired so since I needed surgery anyway I decided to go ahead and revise to a surgery that has the highest success rate, Duodenal Switch.


I was so scared of my intestines being cut and Dr. Keshishian eased my fears. I wish I had went that route the first time but then I might not appreciate it like I do now. Duodenal switch is the ONLY surgery I would recommend to anyone. As Dr K says it’s simple numbers. It’s the surgery with the highest percent of excess weight lost and kept off. I was 252 before my revision from Sleeve to Duodenal Switch and I am just at a year out and today I weigh in the low 190’s and I am still losing. Dr K’s goal for me was about 180. My goal is about 175. I eat more fat now than I ever did even when I was 400 lbs. I enjoy what I eat and I enjoy exercising and most of all I get to enjoy seeing results from my hard work. Food no longer causes me stress and anxiety. I know with 100% certainty that I made the right decision. Thank you Dr. K for your great skill and I don’t mean just with the knife but with the way you are able to make a high anxiety situation seem like no big deal.


Metabolism following Reconstructive Surgery
April 18, 2017 7:47 am
I’ve had some questions regarding how Reconstructive Surgery can affect weight loss and metabolism after Duodenal Switch, Vertical Sleeve Gastrectomy, weight loss surgery and even in people who have not had weight loss surgery. There are several components that can effect a change in metabolism following Reconstructive Surgery that relates to physiological, functional, social and emotional mechanisms. These possible effects can vary person to person based on body type, age, weight, motivation, etc.
Fat mass resection and liposuction
Liposuction or the removal of fat mass by panniculectomy or abdominoplasty can have effects on lipid profile, leptin, waist hip ratio and glucose metabolism for 3-12 months depending on the individual and their health status. This have been researched and documented in both normal and higher BMI individuals. There is also an improvement noted in post bariatric surgical patients having breast reduction and abdominal plastic surgery. Of course, these effects can be controversial, conflicting and further research is needed.
Decrease in inflammatory markers
There is some evidence that the excision or liposuction of fat mass an decrease inflammatory markers and insulin resistance. This can affect C-reactive protein, TNF and cytokines levels. Little is known about the actual mechanism of this effect but the potential for this physiological change is present.
Increase metabolic need for healing
The metabolic needs following plastic surgery are much greater due to the nutrient needs required for healing. Depending on the extent of skin and tissues excised, the nutrient requirements can be considerably higher. This increase in nutrient need can increase metabolic rate, meaning you need more energy for healing. This significant stress also increases the complication associated with reconstructive surgery after weight loss surgical procedures.
Increased Motivation:
Many people are more motivated following plastic surgery because of the dramatic change in body appearance and ability. The increase in motivation can be either diet or physically related. Some people are more motivated to watch what they are eating and increase physical activity to increase the effect of plastic surgery. Obviously, this is an extremely individual experience and can happen in varying degrees
Possible increased restriction
In the case of abdominoplasty, there can be an increase in restriction due to tightening of the skin, muscle and inflammation of the abdominal wall. Thereby, helping to have a fuller feeling sooner when eating. This can also at times result the chance of the complication of reflux and/or stress urinary incontinence if the abdominal muscle tightening is excessive or there is weight regain later on after the abdominoplasty.
Increase mobility and functional status
Excess skin can impair mobility and physical activity for some. The removal of the excess skin can promote mobility, ease of movement, improve gait and posture, and can improve or relieve pain. Skin infections, rashes and irritation are often symptoms of excess skin especially in the abdominal or pelvic area. This is a functional improvement, and depending on the extent of the pannus, can be quite freeing.
Increased confidence
Improved self confidence, anxiety, mood, and body image are important motivators and incentives to post bariatric and plastic surgery patients. These improvements can have an effect on social and relationship aspects. However, it’s important to note that patients undergoing cosmetic surgery should have realistic expectations. Cosmetic, plastic or reconstructive surgery is not a panacea and does not in itself solve body image, personal or psychological issues. In addition, a post Bariatric patient may need additional time to recognize their physical and psychological changes following plastic or reconstructive surgery.
Summary
There may be metabolic, physiologic, physical and psychological improvements following Reconstructive surgery either after weight loss surgery or in non weight loss patients. These changes will vary based on the individual, age, dedication, health status, adherence to instructions, past medical and psychological history. However, appropriate education, screening and realistic goals and outcomes need to be emphasized prior to undergoing any type of plastic or reconstructive surgery.