Category: protein absorption
Too Much Protein & Protein Metabolism
December 17, 2024 12:40 pm

Length of Bowel : Hess or No Hess
March 22, 2020 5:58 pm
“…What is the length of my common channel” is probably one of the frequently asked questions about the duodenal switch operation in the office. This usually comes up at the initial consult when patients repost credible sources such as Dr. Google and Dr. Facebook for patient with different bowel length have done well or not so after duodenal switch operation. Dr. Hess described the Duodenal Switch by using total bowel length measurements and creating the common channel as a percentage of the total small bowel length. However, it seems that this is being done less and less.
This leads to my explanation that is on the website
Hess calculator : Bowel Length Calculator
How the actual measurements matters: Bowel length video link
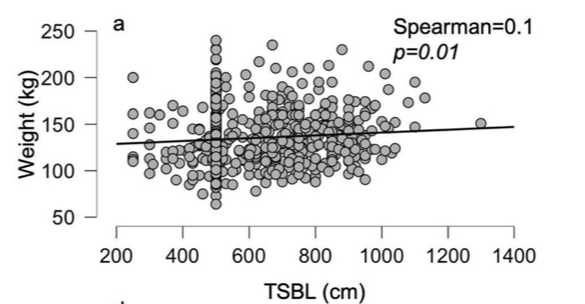
In 2019, Bekheit et.al published a very interesting study comparing total small bowel length (TSBL) to a number of variables such as height, weight, sex and BMI. They identified a few loose correlations. Male patient have longer TBSL than females. There was correlation between TSBL and height stronger in males than females but not statistically significant.
In Conclusion they reported ” Despite statistical significance of the correlation between the TSBL and the height and weight of the included participants, the correlation seems to have no clinical meaning since the effect size is negligible. ”
As I have previously discussed this Making the common and alimentary length standard for every duodenal switch patient will make some loose too much and other not enough weight.
Figure 1 shows TSBL on the horizontal axis, and height, weight, BMI and Age on the vertical axis. For the most part what they all show is that one can not predict how long a patients bowel is by any of the measures that we take in the office as a part of the routine exam.
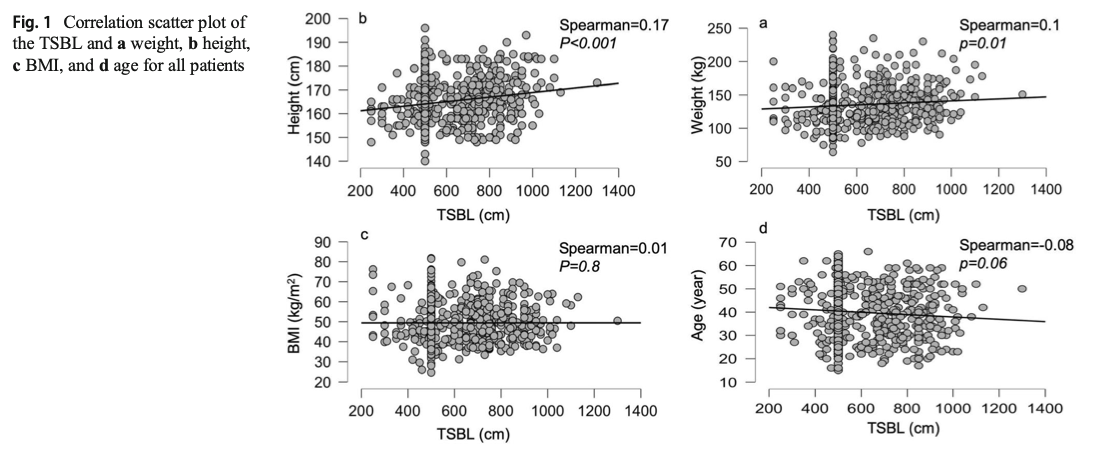
This raises, the concerns that I had raised previously. How could two similar patients who have the same weight, age, sex and BMI have the same surgery and expect the same result if one of them has TSBL of 400 cm and the other one 800cm?
Protein Intake
October 14, 2019 7:08 am
Protein intake requirements change over time following weight loss surgery. This is based on the requirements imposed on our body by a number of variables. These include, activity level, muscle mass, over all health condition to name a few.
A very young muscular athletic male with a BMI or 30 will require much higher protein intake (and absorption) that an inactive older Female with the same BMI. The same young athletic male will require much higher protein intake is he is recovering from a surgery than his baseline.
As we have stated in the past, the protein intake, should be adequate and not excessive. High level of protein intake that are not accounted for based on muscle mass and activity level, will eventually result in weight gain. The best measure of protein intake in a stable weight patient over 3-4 years post op is their albumin and protein level. Following your yearly laboratory values at a minimum is an important part of weight loss surgery follow up care.
You also need to adjust protein intake when necessary. Protein needs increase depending on physical needs, infection, healing, pregnancy, surgery, age, injury, etc. Plastic surgery requires higher protein needs for appropriate healing.
Information on protein sources and quality here.
The basic formula for protein intake is 1gm/kg of ideal body weight. The calculator below will provide a guide for the protein into based on your stable weight in lbs.
Protein Sources
May 16, 2019 10:26 am
Not all proteins are created equally. The protein that we digest serves as the source of the essential amino acids, (the building blocks which make up a protein). The essential amino acids can not be made in out body. Protein sources can be animal or plant based. We’ve written a in-depth explanation of protein sources in this previous blog: Protein Optimization
The proteins can also be decided into two categories:
1-High quality or Complete proteins
Complete proteins contain all the indispensable amino acids that we need. Animal based proteins for the most part are complete proteins. These include cheese, mean, fish, mild, yogurt, egg and poetry.
2-Low quality or Incomplete proteins
Incomplete protein are mostly plant based proteins. In most cases, the incomplete proteins either lack or have insufficient about of the one or a number of amino acids to be able to satisfy our nutritional requirements.
This is why we general recommend animal based proteins.
Following weight loss surgery there are some guidelines that can be helpful in our previous blog: Importance of Protein.
Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium
Shared Success Story- Theresa & Rodney (Duodenal Switch)
August 05, 2017 8:41 am
Life before surgery seems like a lifetime ago for both my wife and I. Being extremely overweight is not only a burden on your general health but a burden on your lifestyle in general. You have the awful label of being called obese, or morbidly obese. This is such a wonderful word that makes you feel as if you have been judged a misfit in society. We were both overweight all of our lives and had done all of the diets known on the planet throughout the years. Some worked a little some not at all and we always found ourselves back to where we were before and usually larger than that. The main focus though as we were getting older was our health. For Theresa it was very difficult. Along with being over 400 pounds she had a severe case of asthma which caused her episodes where she felt she was going to suffocate. She also had very little muscle mass which made it very difficult to get up and down from seating or lying positions. Theresa had her surgery in February of 2014 and not a moment too soon. If she had done nothing it is a good chance that she was facing a horribly short future. She also has a slight heart murmur which did not bode well for a person with her weight. She did not have diabetes thank goodness but her A1C was on the rise as was her BP. She did have sleep apnea as well and had to have a CPAP machine.
I was also severely overweight, my highest weight was nearly 400 pounds and on surgery day I was 355 pounds. I was also under the illusion that I had more control over my weight and that once Theresa had her surgery I would just be able to diet and exercise my way to a healthy weight. I was able to do this in my younger years to a certain extent and I was naive enough to think I could continue to do so. How wrong I was. I had found that no matter how much diet and exercise I did my weight would drop a bit at first but then stall and I would have to essentially starve to lose any more and of course that just makes for a bad outcome. My A1C shot up to 7.6 and this was with 1000mg of metformin a day! My BP was very high with both numbers over 100, well over. This is with a high dose of BP meds. I had a severe case of sleep apnea and could not even consider sleeping without a CPAP machine with a high pressure. I have an artificial hip that was being burdened by my 350 pound plus frame and would probably need to be replaced sooner rather than later. My future was not looking good. Dying before I was 60 seemed like a reality for me and that is not the future I was hoping for. The decision to have weight loss surgery for the both of us was tough. You of course hear the nay sayers spout what a cop out it is and it’s the easy way out! You are just weak and just simply need to not eat hamburgers, French fries and donuts. Just stick with non-fat and low calories and you will reach the promised land. What a load of BS.


Once you wrap your head around the fact that your body is wired in such a way that it will always seek a higher weight every time you lose weight, it’s time to consider the type of surgery. Everyone has heard of the Gastric bypass and that seemed to be the path at the time of Theresa’s surgery. The thing about Theresa and what I admire very much is her persistence and her ability to research to the point where a decision is spot on. She looked at all of the four possible surgeries and quickly realized that the Duodenal Switch was a no brainer. It had the greatest measure of success in the long term as well as short term. Reading about the process and talking to others who have had the surgery it became clear that it was the right choice. Finding out where to go and have the surgery was a real challenge. We were lucky to find Dr. Ara Keshishian and have the ability to travel to his location to have the surgery.
Theresa’s Stats Rodney’s Stats
Surgery Weight: 410 Surgery Weight: 355 Pounds
Total Weight Loss: 215 pounds Total Weight Loss: 170 Pounds
Surgery Type: Duodenal Switch Surgery Type: Duodenal Switch
Surgery Date: February 2014 Surgery Data: May 2016
Surgeon: Dr. Ara Keshishian Surgeon: Dr. Ara Keshishian
Life after surgery is an amazing series of challenges, changes, and a journey that transforms your life in a huge way. For Theresa, it was freedom. Freedom from the overbearing weight she was carrying that kept her from essentially moving or doing anything but staying at home. We did very little outside of the house before surgery. Only the necessities of shopping and keeping up the house on the inside and out. Even that was difficult and went by the wayside all too often. Of course eating out was easier than going to the grocery store and that made the scale just go higher. After surgery, Theresa began to lose weight and you could see day by day the changes. After the first month, you could see a dramatic change not only in her look but the fact that she was moving again! She had dropped 35 pounds in that first month and it made a huge difference. As the weight kept coming off over the next few months we began doing things we have not done before. We started to do a lot of walking and a lot more things around the house that needed to be done. Shopping became a breeze and we ate out a lot less. The dramatic change was in her health. A number of changes for the better were happening on that front. The main one and a huge relief was the asthma. It simply was no longer there. She was no longer short on breath and was simply out moving me! I could barely keep up with her. She also had a bad case of psoriasis which before surgery she could do nothing about. Since the surgery it has disappeared. It might be due to the increased in vitamins, particularly the D vitamin. Her sleep apnea went away and now she is healthy and happy. It is almost difficult to describe the changes until you see them for yourself. For Theresa it has been a life changing experience that has transformed the both of us in ways we never imagined. Theresa eats a normal diet and after 3 ½ years post op she fluctuates about 5 pounds either way. It is amazing.
For me it was not what I expected. What I mean by that is, learning to eat is a challenge. With the Duodenal Switch you are not only eating less, but what you eat is tremendously important to the success of the transformation. With the other surgeries, Lap Band, Bypass and Sleeve you do not have the degree of malabsorption. You simply eat less and you lose weight, but you are still essentially “on a diet”. With the Duodenal Switch you have to consider the malabsorption and think protein first and for most. Once you get past the first month of eating small amounts and what you can while your innards heal you need to learn what to eat and is it enough protein. You may also have to contending with the fact that you have an aversion to foods you ate before. I, for one, could not even eat cheese, and chicken. I pretty much lived on scallops, crab, shrimp and protein drinks for the first three months. Nuts were also a good source of the protein when you get to that stage. This does change and things do go back to normal as far as the taste changes, but it takes a few months. The weight in that first month pretty much peeled off. I was dropping like a pound a day. It was incredible. You think that this is going to be a breeze and you will drop it all in no time! Then that 4 week somewhat of a stall occurs. From what I can tell, everyone experiences it in one form or another. It freaks you out because you start to think about the past where you would work your butt off and either gain or drop and ounce or two. But I was lucky, my wife had gone though it two years before me so she was there to explain that it was normal. The whole “this is a journey thing”, and she was right! At the time though I was listening to the negative voice in my head from the past. That is where the support from the many groups come in. You see that pretty much everyone has the same ups and downs and then your body gives up the farm and you drop a bunch of weight in a weeks’ time. There is really a lot of science behind it. Researching and reading about this particular surgery and how it works will benefit you while you go through the process. Another important thing we face with this surgery is the necessity of Vitamins. Thank goodness for my wife and the DS groups and of course my surgeon. You will not be without knowledge if you actively join the different groups and do your research on the vitamins. I am still learning about what my body needs and am looking forward to my labs in the next month to see where I may be deficient. I have also come to realize the importance of drinking water and avoiding dehydration. I never used to drink it much before the Duodenal Switch, but since the surgery I find it aids heavily in the success if you drink it and drink a lot of it.
To conclude this has been a journey and one I wish I could have done a lot sooner in life, but it is never too late. Today Theresa and I are at weights that we are happy with and our bodies are happy with. We are more active then we have ever been before together. No more days idle in front of the television with large amounts of fast food and drinks. That is what we used to look forward too. Now we cannot wait until we go out and do something. We are not running marathons or anything but we are active and enjoy being so. We no longer have the ailments we had before surgery. Theresa’s asthma is practically nonexistent, living in the northwest with fires in the summer she may have a bout or two. Nothing even close to what she has before and a simple inhale and its gone. Both of us no longer need a CPAP! The freedom to simply lay your head on the pillow and sleep is amazing and wonderful. All of the medication we had prescribed for us are gone as well. My A1C was 5 on my last set of labs and 5.3 on the one before that. Theresa’s is the same and has been for three years. BP is normal and my hip is holding steady. Oh, and another cool thing about it is you can actually shop for clothes anywhere! Your sizes will shrink but we have found we have become quite the clothes horses since losing all this weight. It makes it fun to be able to fit into a size you haven’t seen since who knows when.
Life is always a challenge for many reasons but to remove the burden of the weight simplifies things just a bit. It is a decision we will never regret and wished we had made a long time ago. We both owe our lives firstly, to having Duodenal Switch surgery. Secondly, and most important – was in seeking out the best surgeon we could find, and that was without a doubt, Dr. Ara Keshishian. As a surgeon he is thorough, meticulous, constantly learning and keeping up on the latest research;as a person he is easy to talk to, very approachable, and genuinely cares about his patients before, during and after the surgery process. We could not imagine choosing anyone else.
Importance of ProteinExclusive Member Content
September 08, 2016 2:43 pm
Dual Testimonial: Cameron’s Gastroparesis surgery & Scott’s Revision of a Duodenal Switch
February 01, 2016 8:04 am
In 2015, I came into contact with the most unique, passionate, urgently responsive; talented beyond belief and caring surgeon I have ever met. Our oldest son who is a 21-year-old cancer survivor, has had nearly five years of medical nightmare as diagnosed with severe gastroparesis resultant from his vagal nerve being severed during a previous Nissen Fundoplication surgery. We didn’t find out that this had happened until nearly two years later and only after a 4 hour gastric emptying test showed that Cameron’s stomach was only about 30% emptied after four hours (should be empty after an hour) due to gastroparesis.
I had heard about Dr. Keshishian on a Bariatric support group page on which I post and get great advice. The surgeon back in Central, IL where we live told us that Cameron needed a subtotal gastrectomy to remove 80% of his stomach! This sounded radical and no way in the world was that going to happen. I was given Dr. Keshishian’s email address so I could consult with him for his advice. It was a Saturday morning around 7 AM Central time when I sent off an email to Dr. Keshishian detailing Cameron’s medical history and current issues. I was in hoping that his office would get the email on Monday and hopefully get back to me within a week. I went out to my kitchen to get a cup of coffee and when I returned I had a missed call with a California area code. Yep, it was Dr. Keshishian. I called back and we talked for 45 minutes. He suggested several things and told me that any good general surgeon in my area could do surgery on Cameron and fix him, well that was the only time he was wrong. We couldn’t find anyone in our area who would do the surgery.
So we talked and agreed that Cameron needed a Roux-en Y drain put in place to physically drain his stomach by way of gravity (not for any weight loss as very little small bowel was bypassed). Dr. Keshishian got us in the next week and we flew out to Glendale where he met with Cameron for an examination on that Monday. On Tuesday, Dr. Keshishian performed surgery to fix Cameron’s herniated diaphragm, loose Nissen wrap, performed the Roux-n Y limb and anastomosis to the stomach. Dr. Keshishian also found a Meckel’s diverticulum (a congenital small bowel defect that can cause internal bleeding and serious issues). The following Sunday, Cameron developed severe pain due to chronic pain from his Cancer treatment and 12 subsequent surgeries, many on his abdomen. Dr. Keshishian saw Cameron in the ER and spent 3 hours fixing Cameron’s pain issue and making sure he was medically sound so we could fly home the next day.
Today, Cameron has very little to no issues which you wouldn’t have believed possible six months earlier. In the past, he had violent retching, dry heaving and bad nausea daily which had him severely incapacitated and very depressed due to a feeling of hopelessness and pain from the Gastroparesis. He didn’t believe he had a chance at a normal life but Dr. Keshishian gave Cameron his life back. We are eternally grateful for your huge heart and talent Dr. Keshishian. Thank you!
During our time in Glendale in 2015 for Cameron’s surgery Dr. Keshishian and I began discussing my situation. I had been given a virgin Duodenal Switch performed by a surgeon in Illinois in September of 2013. A year later in 2014 and 180 lbs lighter, I ended up in the hospital as I was passing out. I had a resting heart rate of 35 BPM, a blood pressure in the 75/40 range and incredibly bad labs including anemia, low copper, low zinc, and dangerously low albumin and total protein. A full cardiac work up was completed and I spent a week in intermediate care. Why? I was extremely malnourished even though I was consuming 200-250 grams of protein daily! Why was I malnourished? Because my original surgeon performed a “cookie cutter DS” on me where he didn’t measure my small bowel and arbitrarily gave this 6’2 man a 100 cm common channel and a 150 cm Alimentary limb. Way too short on the AL! Had the Hess method been followed (the only way the DS should be allowed to be completed) my CC would have been 100 cm (that was okay) but my Alimentary channel should have been 275 cm! Simply put, my absorbing portion of small bowel was 34% and the Biliopancreatic limb (non-absorbing) was 66%. It should have been a 50/50 ratio with 100 cm CC, 275 cm AL and a 375 cm BPL. In order to combat my severe malnutrition that September of 2014 I went on a pancreatic enzyme (CREON) to assist my nutrient absorption. I was taking with meals right around 400,000 IU’s of CREON (a boat load) and this was barely keeping my nutrients in range and lab values barely in range. After speaking with Dr. Keshishian, he recommended that I give it until around September of 2015 to see if my absorption increased enough to where a revision wouldn’t be required. Towards the end of July, I all of the sudden lost nearly 20 pounds in two weeks from my already frail and scrawny body. I saw my surgeon in Peoria as I was very alarmed; and I had been having bad cramping and other issues point to a possible bowel obstruction His exact words to me were “see me in 30 days, you are like the DS poster boy of good nutrition”. As you can imagine I found that completely unacceptable and soon as I was out of that appointment I emailed Dr. Keshishian. He told me that if I couldn’t get a revision ASAP I would need to immediately go on TPN. Two weeks later my wife and I landed at LAX and were in Glendale on Monday morning for an exam with Dr. Keshishian.
The job Dr. Keshishian did describing what he was going to do, and of course this was a visual presentation with Dr. Keshishian drawing (you know Dr K’s love of drawing) out for us what he was going to do. He thoroughly explained for my wife and I so she was comfortable with what was going to happen and we fully understood what he was going to do. Doc also found an umbilical hernia that he was going to repair and I had an anal fissure as well that wouldn’t heal so we discussed what he would do to examine and possibly fix during my revision surgery. The next day Dr. Keshishian performed surgery where he fixed the umbilical hernia, measured my total small bowel length to determine appropriate channel lengths and found an repaired a huge mesenteric defect (intestinal hernia and Dr K has a picture of my guts with the huge hole in the mesentery that he has posted on his blog discussing intestinal hernias and blockages), fixed my fissure (Thank you!) and put in a side by side anastomosis that effectively lengthened my AL by 125 cm and my CC by 25 cm worth of absorption. This put my absorbing intestine to BPL ratio where it should have been in the first place (50/50 ratio).
I am pleased to say that I immediately went off the CREON and my absorption and subsequently my lab values improved tremendously. At surgery on August 18, 2015 I weighed a whopping 170 lbs. Today I am weighing in at 183 pounds and well on my way to Dr. Keshishian’s suggested optimal weight target of 205.
Dr. Keshishian is absolutely amazing and the best in the world when it comes to performing the Duodenal Switch and revision to DS Surgery (Band to DS, RnY to DS, Channel extending revision to DS). I would recommend Dr. Keshishian to any patient who needs a virgin Duodenal Switch to get their health back and especially to those who were sold a garbage RnY or Crapband procedure that ultimately failed you (it failed you, you did not fail). In fact, I am trying very hard to convince my brother and Step Mother to fly to Glendale and have Dr. Keshishian perform a Duodenal Switch on them. They very much need it for their health and Dr. Keshishian is the best in the world having performed over 2,000 DS procedures.
I don’t say this lightly. Ara, you are one of the finest human beings I have ever had the good fortune of knowing and your surgical skills are second to none. I really do admire and love this gentleman like a brother and consider him to be a friend. Thank you for using your incredible skill to fix my health issues resultant from the failed cookie cutter Duodenal Switch I was given two years earlier by another surgeon. Had I met you back then and knew what I know now, you would have performed my virgin DS and I would not have suffered for two plus years. Thank you from the bottom of my heart, Dr. K!
Protein Metabolism Optimization
June 09, 2014 5:08 pm
It’s confusing out there in the world of protein supplements and nutrition. Hopefully we can clear up some of the information with this blog post. Part I will be about protein utilization and supplementation and Part II will be about Protein Energy Malnutrition (PEM). So let’s get started with the basics of protein utilization and metabolism. This will clarify what our goals are and what we need to achieve them.

Protein Metabolism:
There are 23 Amino Acids (AA) that combine to form peptide chains. These peptide chains link together to make polypeptides, which are the building blocks of many proteins sources. These types of proteins are called proteinogenic.
Essential vs Non-essential:
Nine of these proteinogenic AA’s are essential meaning that the human body cannot make them. They must be taken in by food sources. The other AA’s are considered non-essential because the body can produce these without an outside food sources.
Complete Protein vs Incomplete Protein:
A complete protein contains all of the essential amino acids and an incomplete protein does not have all nine of the essential amino acids.
|
Essential Amino Acids
|
Non-essential Amino Acids
|
|
Leucine
|
Alanine
|
|
Isoleucine
|
Arginine
|
|
Valine
|
Asparagine
|
|
Histidine
|
Aspartic Acid
|
|
Lysine
|
Cysteine
|
|
Methionine
|
Glutamic acid
|
|
Phenylalanine
|
Glycine
|
|
Threonine
|
Ornithine
|
|
Tryptophan
|
Proline
|
|
Selenocysteine
|
|
|
Serine
|
|
|
Tyrosine
|
|
|
Threonine
|
|
|
Glutamine
|

Branched Chain Amino Acids (BCAA’s) are an incredibly important subgroup of the essential Amino Acids. Three of the nine essential AA’s are BCAA’s. They are leucine, isoleucine and valine. These three AA’s make up 40% of the protein required by humans. Muscle protein is made up of 35% of these three BCAA’s. Any protein supplement after weight loss surgery should contain these three amino acids, Isoleucine, Leucine and Valine.
Protein breakdown begins in the stomach with the addition of enzymes and acid then continues into the small bowel where absorption takes place. Protein must be broken down by these enzymes and acid to single Amino Acids or peptide chains no longer the 4 AA’s in order for the intestinal absorptive cells to absorb the protein. The 4 chain peptide chains are further broken down within the intestinal absorptive cells.
Protein absorption takes place easily but the most important factor is protein utilization. Protein utilization is how much of the protein ingested is actually utilized by the body. The body may absorb a great deal of a protein food source but can only utilize about 30-40g of a high quality protein source at a time. The body does not store protein as it does with other nutrients. Therefore, whatever the body doesn’t utilize is metabolize through the liver and converted to urea. Urea is excreted through the kidneys via urine.
Different proteins absorb at different rates, amounts and in different parts of the small bowel. i.e. Milk protein is 50% absorbed in the proximal small bowel, with 90% of the absorption taking place by the time it reaches the ileum. 1 It’s important to understand this because of the rearranging of the small bowel in the Duodenal Switch. Protein is no longer being exposed to the mucosa of the proximal small bowel due to the altered anatomy of the duodenal switch. This altered anatomy results in much lower absorption of protein, thus the increase levels of protein one needs to consume after WLS. Post WLS the body will compensate and increase protein absorption in the other areas of the small bowel. This may also explain why some weight is regained several years after WLS. 2
Reduced protein absorption is why Bioavailability or Biological Value (BV) is so important when deciding on a protein source. Biological Value is the measure of how efficiently the body utilizes the protein from the food source. You will find this BV number on some protein supplemental products. The higher the BV numbers the better utilization of the protein source by the body. Whey protein and egg protein are considered the highest BV. The daily requirements of protein are 0.80 gram of protein per kilogram of ideal body weight calculating to approximately 50-65 grams a day. 3 However, after weight loss surgery (WLS) a person should get 80-100 grams per day, 1 gram per kilogram of weight and in some cases even higher amounts of protein.
|
Protein Type
|
Protein Biological Value
|
Net Utilization
|
Efficiency Ratio
|
|
Beef
|
80
|
73
|
2.9
|
|
Whey Protein
|
104
|
92
|
3.2
|
|
Soy Protein
|
74
|
61
|
2.2
|
|
Egg
|
100
|
94
|
3.9
|
|
Black Beans
|
0
|
0
|
|
|
Milk
|
91
|
82
|
2.5
|
|
Casein
|
77
|
76
|
2.5
|
|
Poultry
|
80
|
||
|
Fish
|
70-80
|
||
|
Brown Rice Concentrate
|
70-80
|
76
|
Adapted from: U.S Dairy Export Council, Reference Manual for U.S. Whey Products 2nd Edition, 1999 and Sarwar, 1997
Protein Supplements: First clarify the terminology in supplements.
Isolate: Is chemically purified to 90% pure protein. 100g scoop=90g protein intake. Isolates have a High BV rate.
Concentrate: 35-80% protein 100g scoop=35-80g protein intake Also contains fat, carbohydrates and in the case of Whey Concentrate, lactose. Concentrates have a high BV rate.
Blends: Combination of protein sources and purity levels. Varies in how many grams of protein are available in each product. They are lower in cost and quality in some cases. Blends have a medium/high BV rate.
Hydrolysate: enzymatically predigested for maximal speed of absorption and utilization. Very water-soluble but can have a bitter taste. Hydrolysates are high in cost and BV rate.
Branched Chain Amino Acids: contains the 3 essential AA Leucine, Isoleucine, and Valine that make up 1/3 of skeletal muscle and are vital in protein synthesis. Easily absorbed and utilized by the body. BCAA’s have a high BV rate and cost.
Animal Protein Supplements:
Animal proteins contain the 9 essential amino acids the body needs for skeletal muscle formation. It’s important to note that high fat in protein will decrease the amount of absorption and, therefore, utilization of protein due to altered anatomy after DS.
Whey Protein is a byproduct of cheese production. It has a high BV rate and is the most popular protein supplement. It is rich in muscle essential amino acids and has a fast digestion rate. It needs to be taken more often because the ease of digestion. It contains 5% lactose within the product. Whey products come in a wide variety of flavors and styles. Unflavored protein products can be added to other protein foods, such as yogurt, cottage cheese, etc. to increase the protein. Be wary of artificial sweeteners in protein supplements as they can give you unwanted side effects, such as gas or loose stool.
Whey Protein Isolate: (WPI) has one of the highest BV rates 104. WPI can be slightly more expensive but seems to be the most tolerated by WLS (weight loss surgery) patients. There are many flavors and styles with less fat and lactose than other whey protein products.
Whey Protein Concentrate: has a high BV rate 85-90. Concentrate has more fat and lactose, which may not be well tolerated by WLS patients.
Whey Protein Blends: Blends contain a mixture of both isolate and concentrate whey proteins. Which means the BV rate is higher than concentrate on it’s own. Because of increased fat and lactose this too may not be tolerated as well by WLS patients.
Casein Protein is a milk protein and has a BV rate of 91. Casein is the trigger in most milk allergies. It is more slowly digested and more filling than whey protein. It may be more difficult to tolerate after WLS.
Egg Albumin is very high in essential and nonessential AA’s. Eggs are also a great natural food source for protein. Does not have lactose but some people do have egg allergies. It is a cost effective source of protein. Supplement powders come in several flavors. This is probably nature’s perfect protein source with the highest utilization.
Goat Milk: One of the highest BCAA available food sources. Is better tolerated by people with lactose intolerance.
Beef, poultry, fish all have varied degrees of bioavailability. Please see the table above regarding each items BV rate. While beef may have a higher BV rate there may be other issues to deal with higher fat content that goes along with eating most cuts of beef. After DS higher fat content can mean looser stool or even diarrhea.
Vegetable Protein Supplements and Natural Food Sources:
Plant Protein may contain most or all essential amino acids but the amount is far less thank other protein sources particularly in the amounts of BCAA needed for skeletal muscle formation. It is best to combine or vary plant proteins to ensure adequate protein nutrition.
Soy Protein: has a BV rate of 74. It is fast digesting, lactose free and comes in a variety of flavors and unflavored. It is also cost effective and contains all the essential AA’s. Soy beans are commonly a GMO crop, so if that is concerning look for organic sources. Soy is also a high allergen food and can inhibit calcium absorbtion.
Pea Protein: 100% gluten free and lactose free. Pea protein is very easy to digest, rich in Amino Acids and is a high satiety protein. Pea Protein can be found with high levels of carbohydrate and low levels of carbohydrates. After WLS always choose lower levels of carbohydrates.
Brown Rice Isolate: BV of 70-80. Is easily digested and is a good vegan choice. Again with Brown Rice Isolate watch your carbohydrate content. Brown Rice Isolate can be chalky in texture.
Pea/Brown Rice Isolate: BV of 70-90 Combining these two gives a good profile of BCAA that rivals whey and egg proteins. It is easily digestible without allergy issues. When used in combination, rice protein and yellow pea protein offer a Protein Efficiency Ratio and BCAA’s that is comparable to dairy and egg. In addition, the texture of pea protein helps the chalkiness of rice protein.
Spirulina: Blue-green algae is easily digested and high in AA 80-95% of proteins can be digested. BUT is very allergic prone. It is also expensive and the taste can be hard to handle.
Hemp Protein: 30-50 BV rate. Hemp contains 21 amino acids and is considered a complete protein. The proteins in Hemp seeds are easily digestible, absorbed and utilized by the body. Hemp seeds are great to add to natural food products to increase protein and essential fatty acids. It is vegan friendly and low allergy rating.
Summary
So what does this all mean? It is important when looking for a protein supplement or natural food source to look for the highest bioavailable rating and BCAA levels. Most protein supplements have these listed on their labels. Read the labels on supplements to find low fat, carbohydrate and lactose for best tolerance after WLS. Consuming high amounts of fat after duodenal switch decreases the absorptive time the food products due to the altered anatomy after DS. When taking your protein it is best for absorption to have low fat to optimize your protein absorption. Be wary of artificial sweeteners in protein product. They may also cause WLS patient issues, such as increased loose stools or gas. Also, try getting trial sizes of several different supplements to see how your body tolerates the supplement and your taste. If you are not tolerating one brand of supplements try another. Isolate, Egg or Blends are best tolerated after WLS and give the highest bioavailability.
The best routine of taking your supplements after WLS is on an empty stomach in the morning or when you first wake. This is a good time to use an isolate, or blend supplement shake or natural food source such as egg. Have a midmorning protein snack or shake, lunch with high protein foods, a mid afternoon protein snack or shake, dinner of high quality protein and after dinner or as close to bedtime as you can tolerate protein supplement shake. For your meals choose the best BV rating food and also listen to what your body tolerate. Your natural food sources should be low fat, low carbohydrate and low lactose food choices. Also consider adding one of the plant protein supplements or unflavored animal supplements to your natural food sources to give an additional protein boost. The unflavored varieties can be added to nearly any food or recipe. Take care in adding protein powders to higher temperature foods, as high temperatures destroy the proteins. The key is frequent small meals and snacks with the highest quality protein. Varying your protein sources increases your chances of absorbing a variety of amino acids and nutrients.
After surgery, you should expect to be able to consume the same amount of grams of protein as the number of days post op that you are. i.e.; 30 grams of protein at the end of the first month, 60 grams of protein by 60 days post op, etc. Treat your body as you would an infant just starting to eat new foods. Try small amounts of food and only progress with a new item after several days of tolerating an old food. As always follow your surgeon’s guidelines and recommended diet. Do not progress until your surgeon has given you the go ahead.