Category: GERD
Surgery for Reflux
August 02, 2025 6:58 pm
Surgery for Reflux
Gastroesophageal reflux disease (GERD) is a common gastrointestinal problem in both the general population and post-weight-loss surgical patients.
The general population may have GERD symptoms with weight gain, pregnancy, hiatal hernia, Helicobacter pylori infection, gallstones, ulcers, motility issues of the esophagus or stomach, and other conditions. With proper workup, they all have their specific treatment plans. In a post-weight-loss surgical patient, some of the exact causes may be present in addition to those that may be specifically related to the type of surgery and its unique side effects and complications.
There is a subset of patients with hiatal hernia who should undergo surgical repair, but do not. There has been a series of publications from over 15 years ago that have been embraced by the gastroenterologist who frequently, incorrectly, dismisses Nissen fundoplication as an effective surgical tool for the treatment of GERD and hiatal hernia.
The treatment for GERD with a hiatal hernia, regardless of size, is Nissen Fundoplication and not lifelong use of proton pump inhibitors (omeprazole, pantoprazole) and other classes of medication. It should be noted that these medications were never approved for long-term use and can cause significant metabolic and gastrointestinal side effects.
Recent publications have shown that not only the old data that gastroenterologists frequently rely on was not reliable, but also that surgery is very safe and effective with a very low rate of short and long-term complications.
Three Different Problems: Gastritis, Gastroesophageal Reflux, and Bile reflux Gastritis
June 05, 2025 4:52 am
Gastritis is a general term used for the description of symptoms associated with several very different physical conditions and require different treatments based on their ideology . Gastritis, gastroesophageal reflux, and bile reflux gastritis
Gastritis may be caused by excess acid or bile in the stomach. Some patients may have gastroesophageal reflux due to a hiatal hernia, which needs to be treated surgically with Nissen fundoplication, regardless of the size of the hernia, contrary to what gastroenterologists recommend by prescribing antacids for an extended period. I have seen patients who have had one cm hiatal hernia and have been very symptomatic, and others who have had larger hiatal hernias and have been asymptomatic. Size should not be a determinant of whether the patient has had or will have a hernia repair or not.
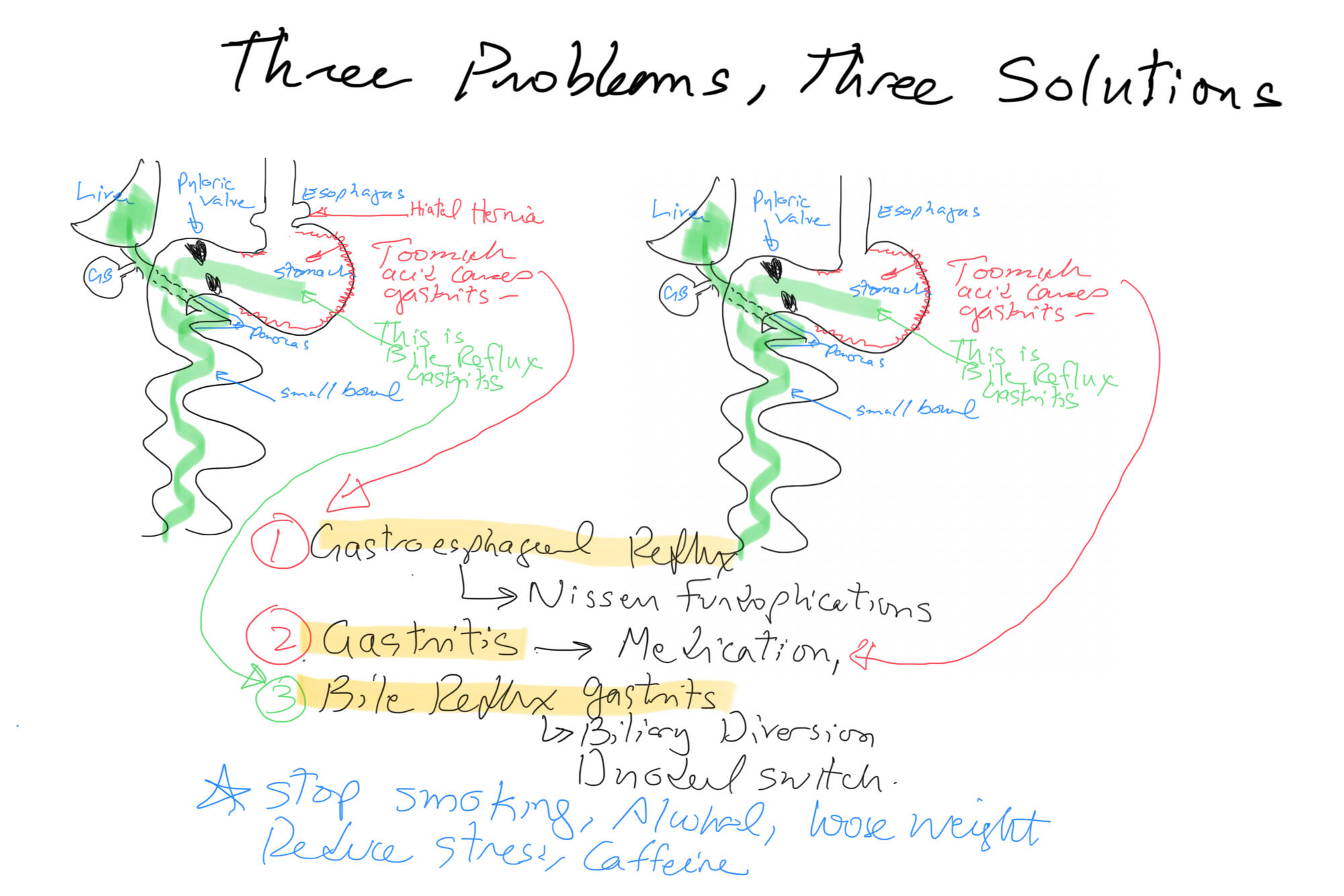
Billiary Diversion is the definitive surgical procedure for Bile Reflux Gastritis.
Bile Reflux Gastritis and Cholecystectomy
May 21, 2025 2:41 pm
Bile reflux gastritis is not a the result of the cholecystectomy but may be seen in a subset of patient with other confounding conditions. Bile is produced in the liver and stored in the gallbladder. In response to high fat and protein in the stomach, the gallbladder contracts to ” squeeze” the bile stored in the gallbladder into the small bowel to help absorb the fat and protein.

With the gallbladder removed, the bile produced by the liver cannot be stored and goes directly to the small bowel via the biliary tree.

It is possible and likely that some of the bile will find its way back to the stomach. In some patients, due to compounding circumstances, the bile may collect and cause gastritis. We need to dissect this a little for it to make sense.
- Not every patient after cholecystectomy will have bile in their stomach.
- Not every patient with bile in the stomach has gastritis.
To appreciate this, let’s remember that for bile to get from the small bowel to the stomach, it needs to:
- Go upstream, against the peristalsis of the small bowel, and do not be washed down by the flow of the gastric
- juices coming out of the stomach.
- Go through the pyloric valve.
- If it reaches the stomach, the acid in the stomach does not neutralize it, causing gastritis.

As I’m sure we all appreciate, other contributing factors besides cholecystectomy may cause bile reflux and bile reflux gastritis. This is why it’s also emphasized that bile in the stomach alone does not confirm biliary reflux gastritis. It is also why we always state that bile reflux gastritis is a disease of exclusion, where other conditions such as gastroparesis, acid reflux, and hiatal hernia (regardless of size, as some patients are unfortunately told that since the hernia is small it does not need to be fixed, which is incorrect) must be considered. Further information on Bile Reflux.
Billary Diversion is the only definitive surgical procedure for Bile Reflux Gastritis.
Staples Used in Gastrointestinal Surgery
February 11, 2025 11:23 am
I have frequently been asking what staples are used in sleeve gastrectomy. A stapling device is used with sleeve gastrectomy. This device comes in different shapes and sizes for different bowel thicknesses and applications. However, they all function the same way. The staple cartridges (the part of the stapler that is replaced after each use with a new one) are selected based on the thickness of the segment of the bowel that needs to be stapled and divided.
The stapling and dividing take place simultaneously. The sampler deploys six rows of staples and cuts between them, leaving three rows on one side and three on the opposite side. With the sleeve gastrectomy, this means that the sleeve stomach that is left has three rows of staples, and the segment of the stomach that is removed also has three rows of staples.

1-Can I have a CT or an MRI done? Yes, The titanium staples are safe for both CT and MRI.
2-What are they made from? The staples are made of titanium and alloys, which are non-reactive and safe.
3-How big are the staples? Different staples are of different sizes, mainly in the mm range; see the tip of the pencil in the image for the relative size.
Video of stapler demonstation here

Long Term Health Implications of PPI Use, Antacids
November 19, 2019 12:38 pm
The FDA had initially approved almost all PPI’s, and antacids with an explicit limit placed on the duration of the therapy, which ranged in days to weeks. At that time there were no long term studies done on the health benefits, or side effects of the long term use of the PPI.
This Summary Letter outlines all the concerns dating back to 2011. I have found the information in this letter a good overview of the supporting medical evidence and lack of any long term data in regards to long term PPI.
The FDA made changes in the Black Box warning of the PPI medications. This was done with the mounting evidence and the health concerns of long term PPI use.
PPI’s have been shown to have detrimental long term side effects. It is prudent that a patient is continuously monitored and evaluated for identification of the possible underlying causes of the reflux, that may be the reason for the PPI use. There are a whole host of potential causes of reflux and other options for treatment.
There have been numerous studies recently published:
It can lead to increase risk of fractures and in a large study from the VA system it has been associated with the risk of premature death
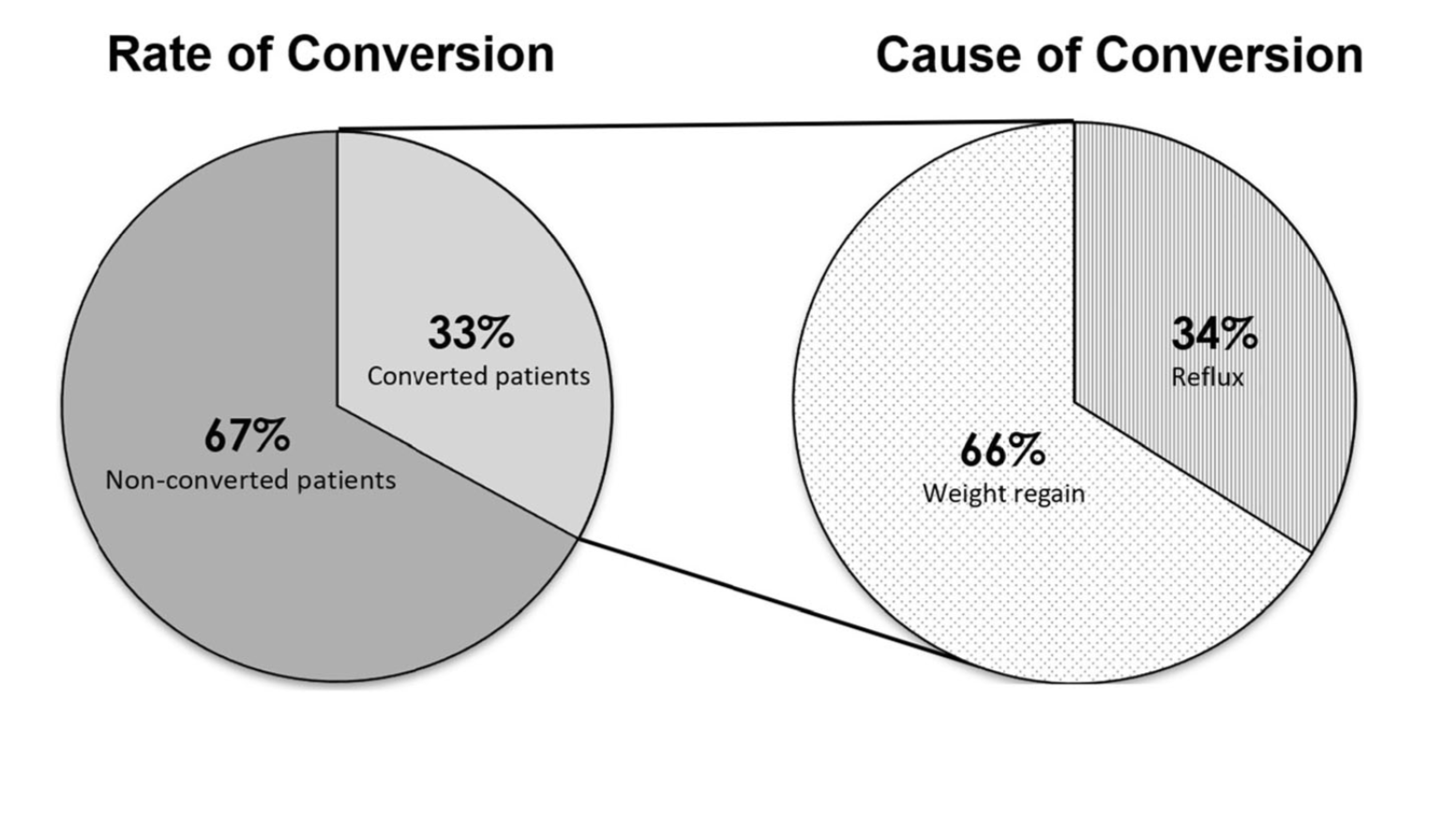
Sleeve And Weight Regain
July 22, 2019 9:50 am
Gastroesophageal Reflux: Bile Vs. Acid
May 14, 2019 12:52 pm
Gastroesophageal (GE) reflux is the condition when the stomach contents are able to “reflux” back through an incompetent lower esophageal sphincter (LES) into the esophagus.
Gastroesophageal reflux Disease (GERD) is a clinical condition caused by long-standing reflux that results in microscopic and visible changes to the inner lining of the esophagus and esophageal mucosa.
GERD is nondescript as to the cause of the condition. It only states that the stomach contents have been irritating the lining of the esophagus on a chronic basis. This can be caused by an anatomical abnormality of the GE junction (hiatal hernia) or may be related to dysfunction of the LES. Other possible causes of GERD may be infection (H. Pylori), environmental (stress), and dietary (nicotine, alcohol, caffeine, spicy food) in origin.
So far, we have not clarified the chemical nature of the refluxed content.
In Acid Reflux, the relative acid overproduction of acidic secretion and the exposure of the esophageal mucosa need to be addressed. This is accomplished by acid suppression medications, anti-histamine (H2 blockers), and Proton pump inhibitors (PPIs). The physiology and the mechanism involving this condition are well understood. As a surgeon, however, I do see patients who should have had surgical intervention. The initial mode of therapy for a patient with documented acid reflux and or symptomatic hiatal hernia is placing them on medication. These patients are then recommended to have a related upper endoscopy. Patients who do not improve or where deterioration of the esophageal mucosa and the presence of precancerous cells are referred for surgical intervention.
Bile Reflux, contrary to acid reflux, may have tiny, if anything, to do with the LES. The symptoms experienced by the patient may be as after related to the excessive bile in the stomach, which is seen frequently
after cholecystectomy, or in those patients with a dysfunctional gallbladder (low EF on HIDA scan).
The treatment of Bile reflux is Duodenal Switch without the associated sleeve gastrectomy component in addition to repair of hiatal hernia if present. Ann Surg. 2007 Feb; 245(2): 247–253.
Candy Cane Gastric Bypass – RNY
June 21, 2018 1:05 pm
One of the findings following Gastric Bypass is a Candy Cane Gastric Bypass. Nausea and vomiting , upper abdominal pain is a common complaint of patient who have had the Gastric Bypass RNY operation. This is in addition to the high incidence of patients who experience the complications of weight regain and or dumping syndrome.
Quite frequently the symptoms of nausea, vomiting and upper abdominal pain of a patient with history of gastric bypass is evaluated by a primary care, referred to a gastroenterologist. The “routine” work up recommended is X-ray of the abdomen, maybe contrast study (Ct scan or upper GI) and for sure and upper endoscopy. The result quite frequently reported as “…nothing wrong”.
A typical upper GI in a Candy Cane Gastric Bypass situation may look like this:

A common and underreported problem may be a Candy Cane finding. The “blind” end of the small bowel anastomosis is too long and this results in food settling in the hook of the candy cane. The symptoms of the nausea, vomiting and upper abdominal pain may be from the residual food and liquids that do not drain from this area.

Candy Cane Gastric Bypass finding

Candy Cane Gastric Bypass cases will require surgical intervention to shorten the length of the blind segment of the small bowel to improve symptoms.
It is my recommendations that any patient with history of weight loss surgery who is having any persistent gastrointestinal symptoms be evaluated by weight loss surgeon.
Bile Reflux Gastritis
January 10, 2018 1:45 pm
Bile reflux gastritis has been recognized as a significant cause of dyspepsia in a subset of patients. This patient group set does not respond to the standard treatment (not expected to) and some get improvement with the treatment of H.Pylori infection if one is diagnosed at the time of upper endoscopy and biopsy.
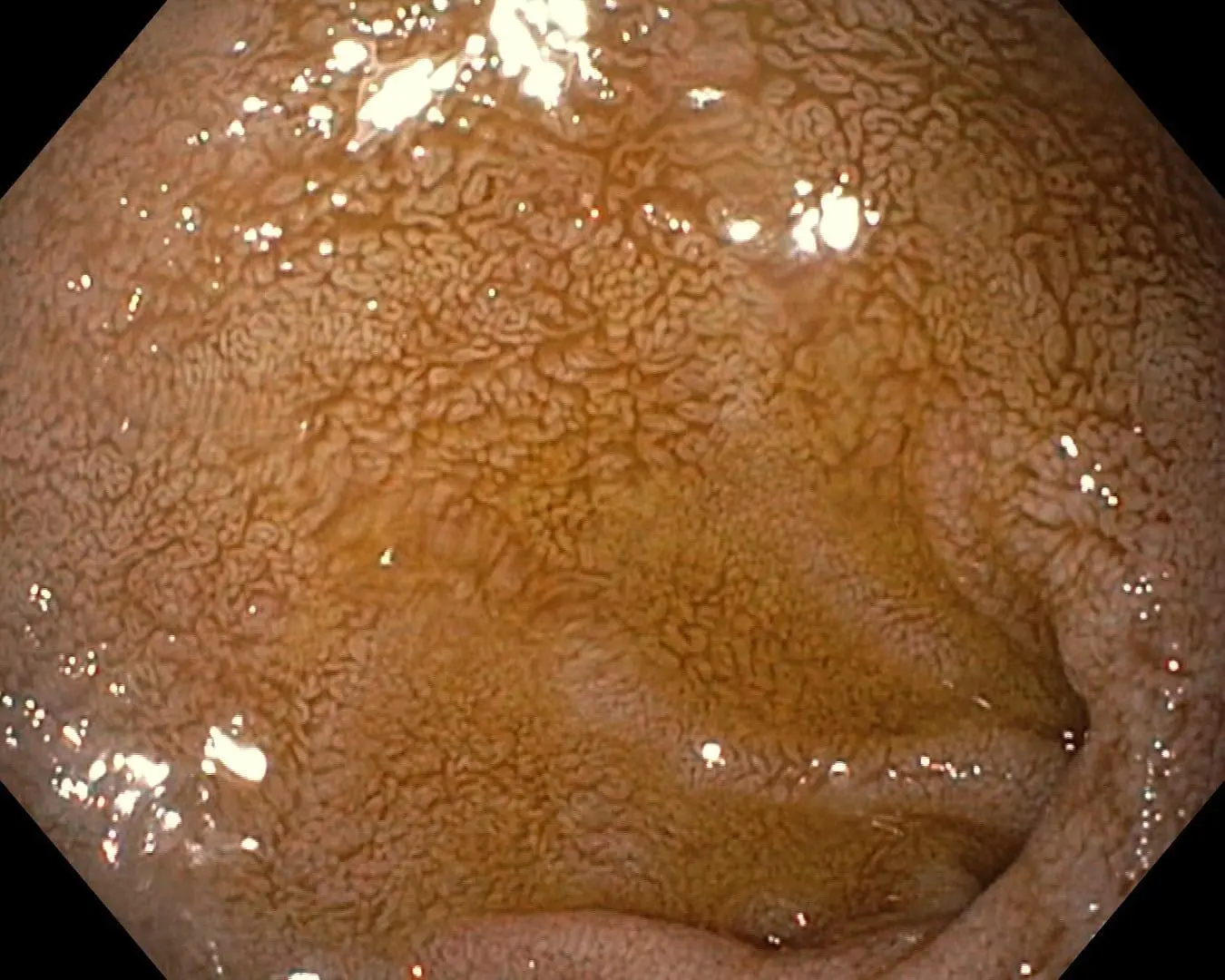
Inflammation and Foveolar hyperplasia are some of the findings that can be seen endoscopically. This and other findings have all been documented in the literature. An article published in 2005, reported over 40% incidence of Foveolar hyperplasia in patient with bile relax.
It is been noted that bile causes the thickening of the mucosa lining of the GI track. This is called Foveolar hyperplasia when the mucosa of the stomach is noted to be thicker with more numerous and deeper folds.

The treatment for this is reduction and prevention of bile reflux to the stomach, in some cases this can only achieved by surgical diversion of the bile from the stomach. Additional information on Bile Reflux and the surgical treatment can be found here.
Reflux and Hiatal Hernia
April 17, 2017 9:41 am
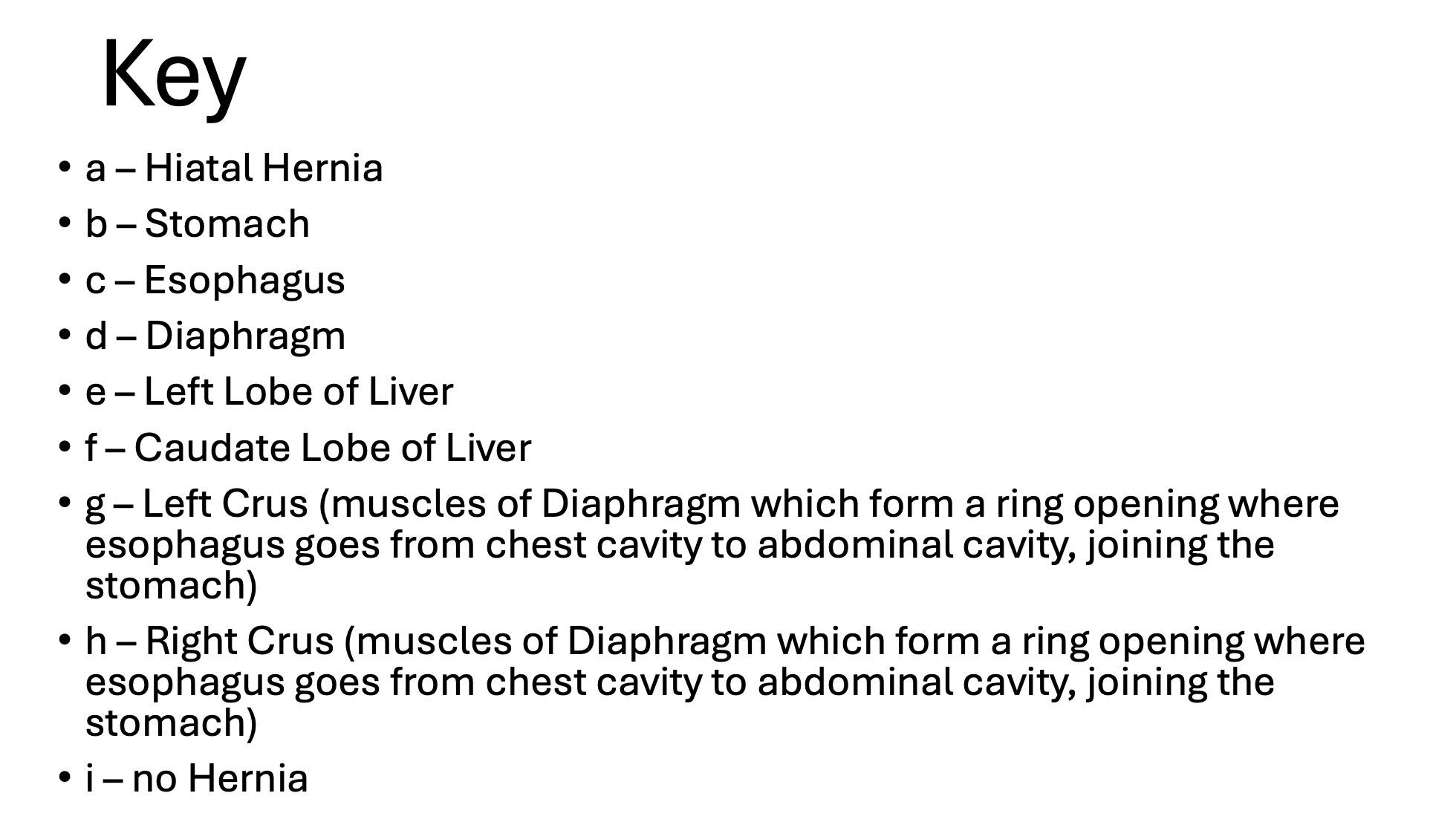
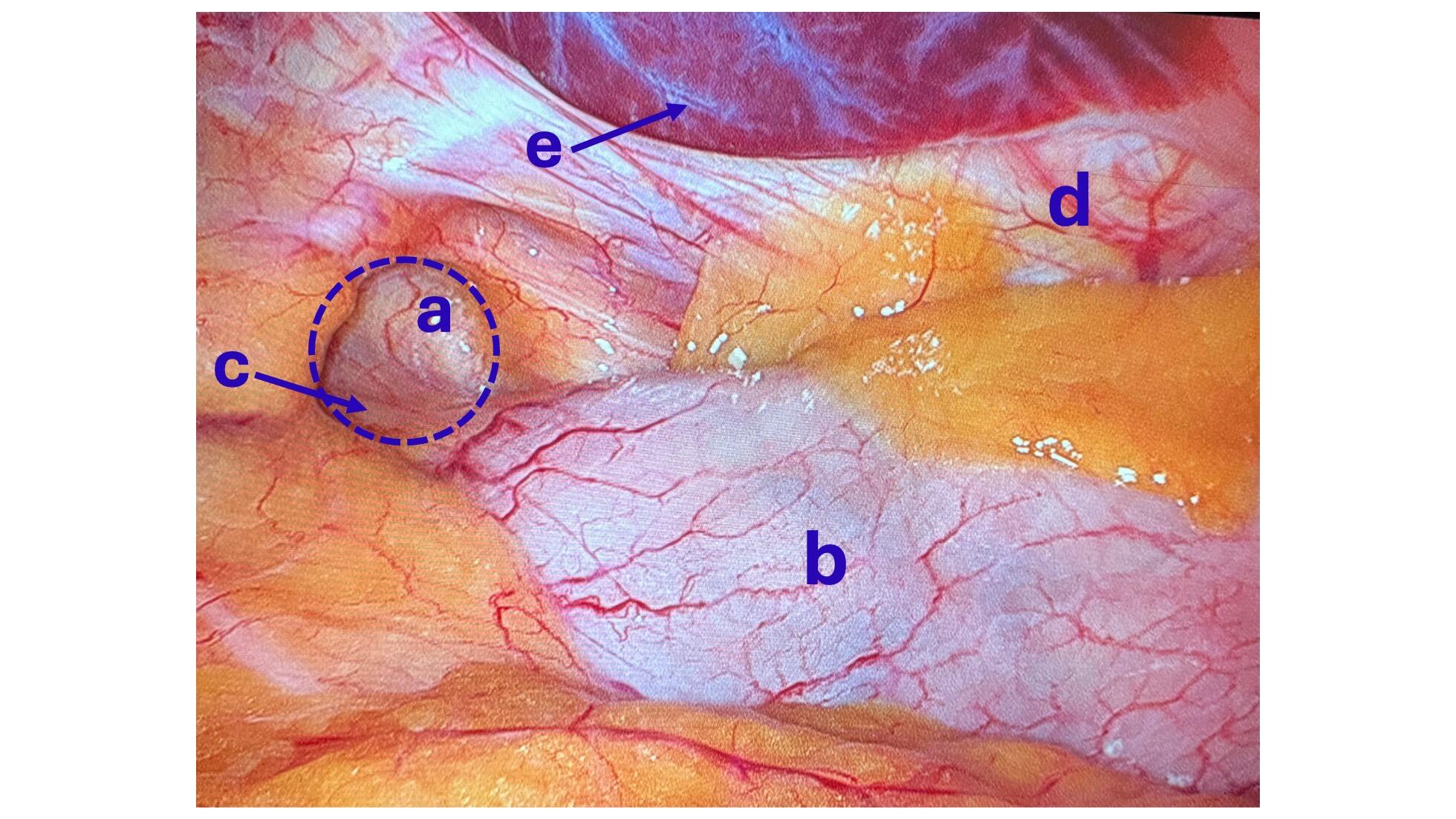
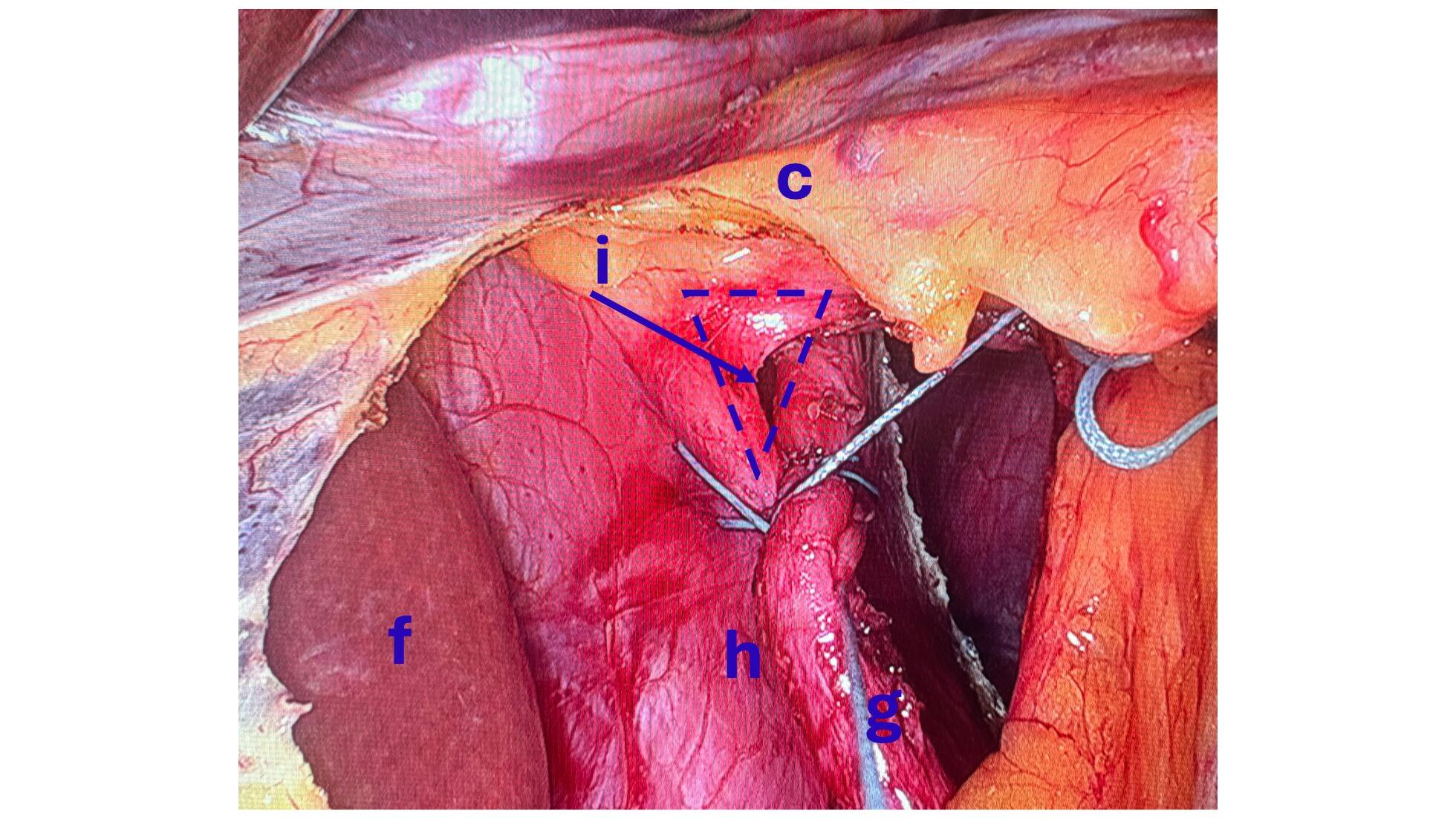
One of the leading reasons for Gastro-esophageal reflux disease (GERD) is a physical defect called a Hiatal hernia. The esophageal Hiatus is the opening in the diaphragm where the esophagus enters from chest cavity allowing the esophagus to pass into the abdominal space. If the opening in the diaphragm is much larger than the esophagus, it will result in reflux of the stomach secretions and food from the stomach into esophagus. *Note: Graphic surgical pictures below
Hiatal Hernia Causes:
- heavy lifting
- coughing
- obesity
- injury
- persistent vomiting
- age related
Reflux and Hernia Symptoms:
- sour taste
- reflux
- heartburn
- belching
- chest or abdominal pain
- difficulty swallowing
- vomiting
- no symptoms


The treatment includes dietary changes, medication and in those who do not improve surgery.
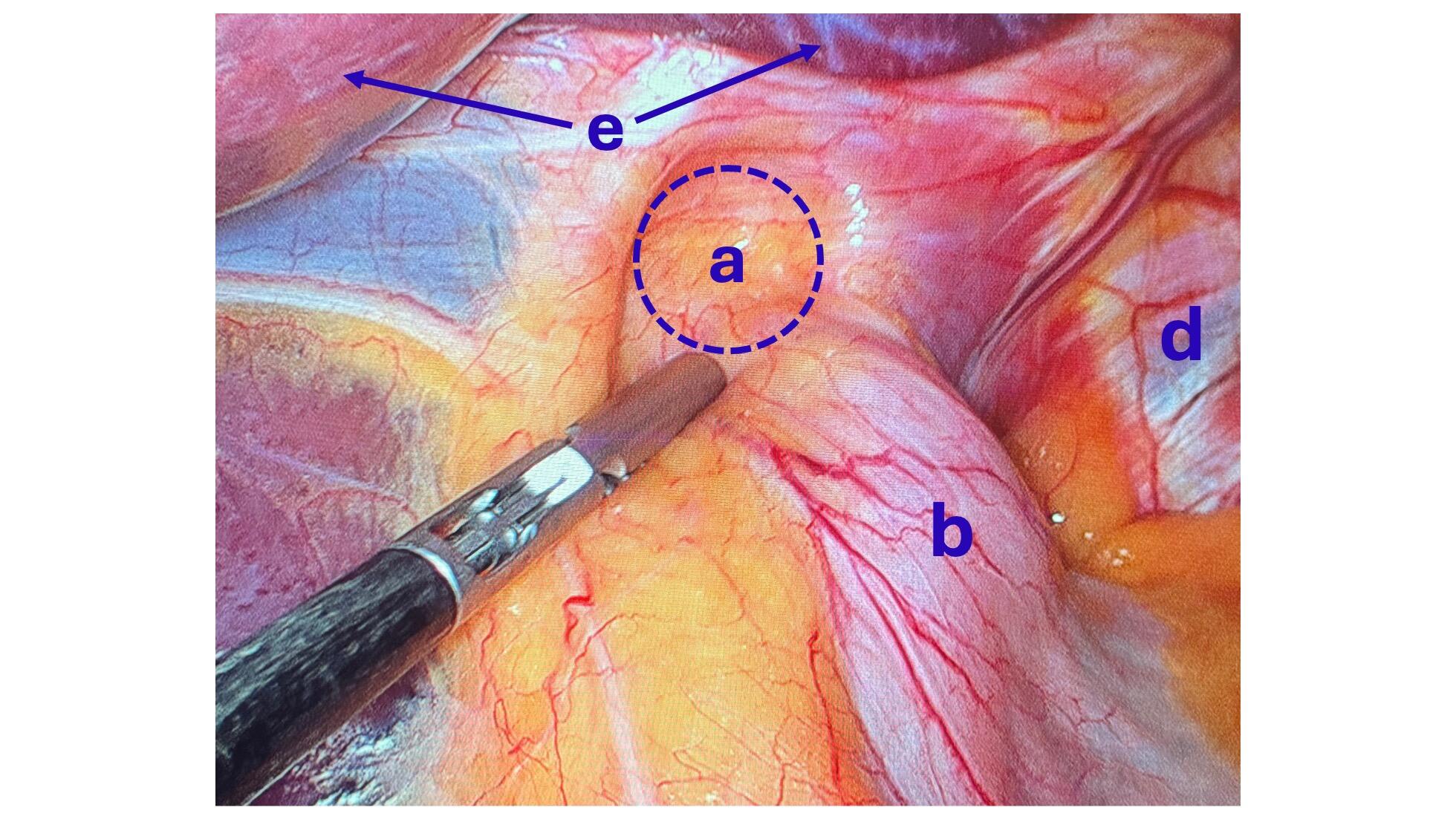
Hiatal hernia repair includes tightening of the dilated opening of the esophageal hiatus by re-appoximating the separated muscle fibers of the right and the left crus. This tightens the defect in the diaphragm and helps prevent part of the stomach or stomach contents from entering the chest cavity.
You can find further information and dietary changes regarding Hiatal Hernia and GERD here, including information unique to weight loss surgery and Hiatal Hernia. You can also find further surgical information, as well as a surgical video here.