Category: Endoscopy
Surgery for Reflux
August 02, 2025 6:58 pm
Surgery for Reflux
Gastroesophageal reflux disease (GERD) is a common gastrointestinal problem in both the general population and post-weight-loss surgical patients.
The general population may have GERD symptoms with weight gain, pregnancy, hiatal hernia, Helicobacter pylori infection, gallstones, ulcers, motility issues of the esophagus or stomach, and other conditions. With proper workup, they all have their specific treatment plans. In a post-weight-loss surgical patient, some of the exact causes may be present in addition to those that may be specifically related to the type of surgery and its unique side effects and complications.
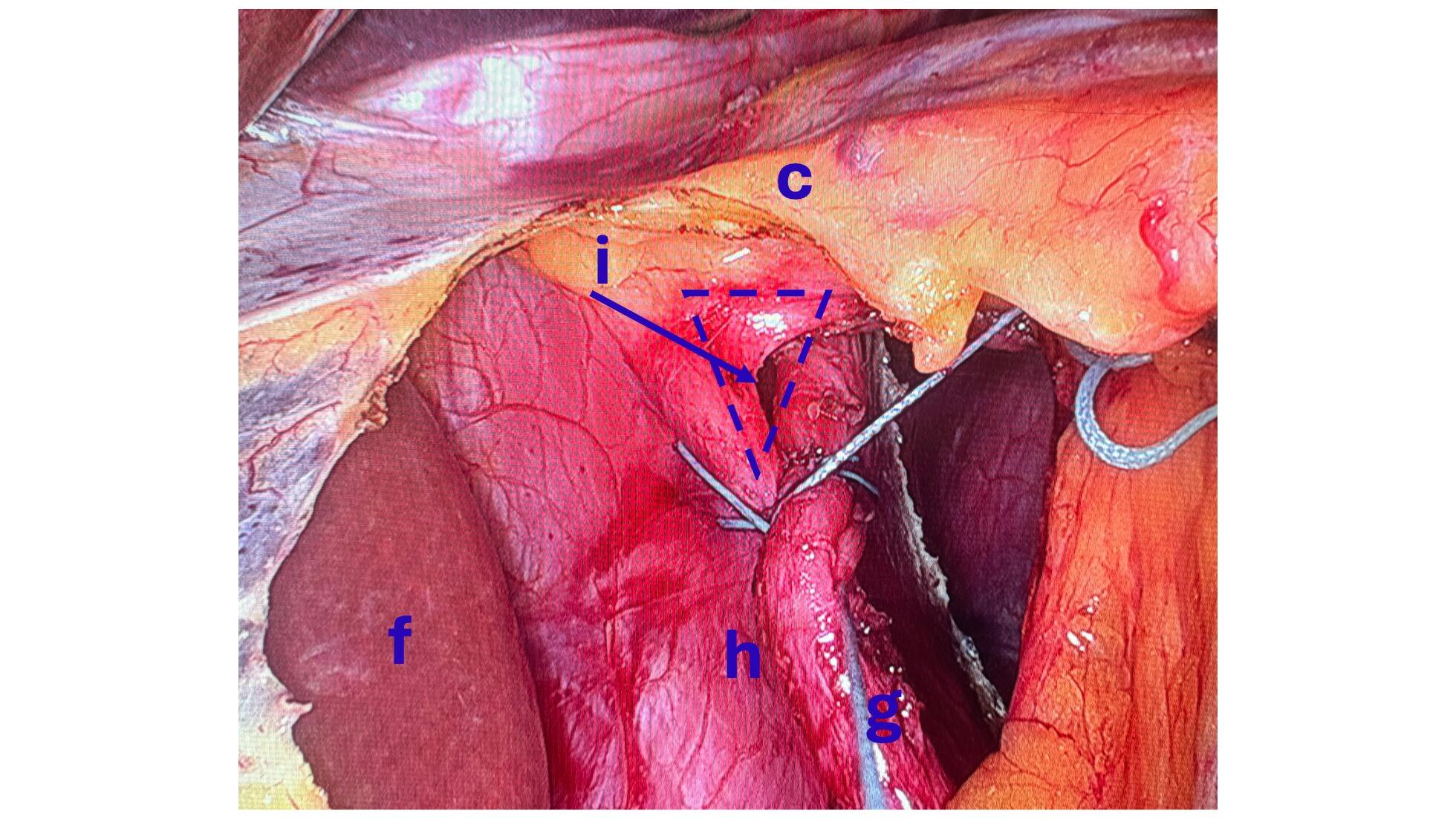
There is a subset of patients with hiatal hernia who should undergo surgical repair, but do not. There has been a series of publications from over 15 years ago that have been embraced by the gastroenterologist who frequently, incorrectly, dismisses Nissen fundoplication as an effective surgical tool for the treatment of GERD and hiatal hernia.
The treatment for GERD with a hiatal hernia, regardless of size, is Nissen Fundoplication and not lifelong use of proton pump inhibitors (omeprazole, pantoprazole) and other classes of medication. It should be noted that these medications were never approved for long-term use and can cause significant metabolic and gastrointestinal side effects.
Recent publications have shown that not only the old data that gastroenterologists frequently rely on was not reliable, but also that surgery is very safe and effective with a very low rate of short and long-term complications.
Gastroesophageal Reflux: Bile Vs. Acid
May 14, 2019 12:52 pm
Gastroesophageal (GE) reflux is the condition when the stomach contents are able to “reflux” back through an incompetent lower esophageal sphincter (LES) into the esophagus.
Gastroesophageal reflux Disease (GERD) is a clinical condition caused by long-standing reflux that results in microscopic and visible changes to the inner lining of the esophagus and esophageal mucosa.
GERD is nondescript as to the cause of the condition. It only states that the stomach contents have been irritating the lining of the esophagus on a chronic basis. This can be caused by an anatomical abnormality of the GE junction (hiatal hernia) or may be related to dysfunction of the LES. Other possible causes of GERD may be infection (H. Pylori), environmental (stress), and dietary (nicotine, alcohol, caffeine, spicy food) in origin.
So far, we have not clarified the chemical nature of the refluxed content.
In Acid Reflux, the relative acid overproduction of acidic secretion and the exposure of the esophageal mucosa need to be addressed. This is accomplished by acid suppression medications, anti-histamine (H2 blockers), and Proton pump inhibitors (PPIs). The physiology and the mechanism involving this condition are well understood. As a surgeon, however, I do see patients who should have had surgical intervention. The initial mode of therapy for a patient with documented acid reflux and or symptomatic hiatal hernia is placing them on medication. These patients are then recommended to have a related upper endoscopy. Patients who do not improve or where deterioration of the esophageal mucosa and the presence of precancerous cells are referred for surgical intervention.
Bile Reflux, contrary to acid reflux, may have tiny, if anything, to do with the LES. The symptoms experienced by the patient may be as after related to the excessive bile in the stomach, which is seen frequently
after cholecystectomy, or in those patients with a dysfunctional gallbladder (low EF on HIDA scan).
The treatment of Bile reflux is Duodenal Switch without the associated sleeve gastrectomy component in addition to repair of hiatal hernia if present. Ann Surg. 2007 Feb; 245(2): 247–253.
GI Bleed following Weight Loss Surgery
September 17, 2018 10:28 am
Gastrointestinal (GI) Bleed following weight loss surgery is rare but does require knowledge of the particular bariatric surgical procedure the patients has and how to proceed with diagnostics to fully evaluate the situation. Acute or chronic gastrointestinal bleeding can cause anemia in patients. However, Anemia may also be caused by nutritional deficiencies (iron, vitamin , minerals), Kidney disease, bone marrow disease and others. The work-up for anemia following weight loss surgery follows a routine protocol. If there is an evidence of bleeding from intestine (bloody emesis, bloody bowel movement, “tar” like black bowel movements) then the diagnostic work up would include an upper and lower endoscopy.
Endoscopic Procedures:
Upper endoscopy Esophagogastroduodenoscopy (EGD): evaluates the esophagus, stomach and a limited area of the duodenum past pyloric valve.

Lower endoscopy Colonoscopy or coloscopy: evaluates the rectus and the entire colon.
Between these two tests, there is still a considerable amount of the small bowel that is not accessible or visualized with endoscopic procedures. For the small bowel, examination Capsule endoscopy is an option in an intact GI tract. Patients who have had Gastric bypass RNY or the Duodenal Switch, the large segments of the small bowel can not be visualized or examined with capsule endoscopy.



Patients who have had Duodenal Switch, Gastric Bypass and SADI – S would need a tagged red cell scan or CT angiography if GI bleed is suspected in areas of the small intestine that are inaccessible by endoscopic procedures.