Category: AdjustableGastric Band
A patient story: Lap Band complication and Wegovy
October 24, 2024 4:30 pm
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wegovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
- Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
- Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
- GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
- GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
- I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
- There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
- A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity

Radiology film of normal position and a slipped LapBand

SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
https://www.dssurgery.com/wp-content/uploads/2024/09/P000008S017b.pdf
https://www.dssurgery.com/wp-content/uploads/2024/09/20-year-all-procdure-metaanalysis.pdf
https://www.dssurgery.com/weight-loss-injection/
https://www.dssurgery.com/glp-1/
https://www.dssurgery.com/weight-loss-medications-compared-to-surgery/
https://www.dssurgery.com/articles/glp-1-agonists-a…agency-clinicians/
https://www.dssurgery.com/articles/managing-the-gas…clinical-practice/Should Adjustable Gastric Banding (Lap Band) be done?
October 06, 2024 9:17 pm
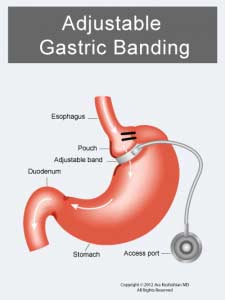 The Lap Band was approved in the US in 2001 (BMI> 40). The following studies used only small samples and examined short-term efficacy and safety. They were then performed to consider the utility of the Laob band for patients with lower BMI (BMI 30-40).
The Lap Band was approved in the US in 2001 (BMI> 40). The following studies used only small samples and examined short-term efficacy and safety. They were then performed to consider the utility of the Laob band for patients with lower BMI (BMI 30-40). 
- The Lap Band does not result in long-term sustained weight loss.
- Lap band has significant complications, some of which may not be reversible.
- The lap band can be removed, but eroding the banc to the stomach is not easy.

Articles
March 22, 2020 6:57 pm
Sleeve Gastrectomy Failure
May 07, 2019 12:53 pm
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
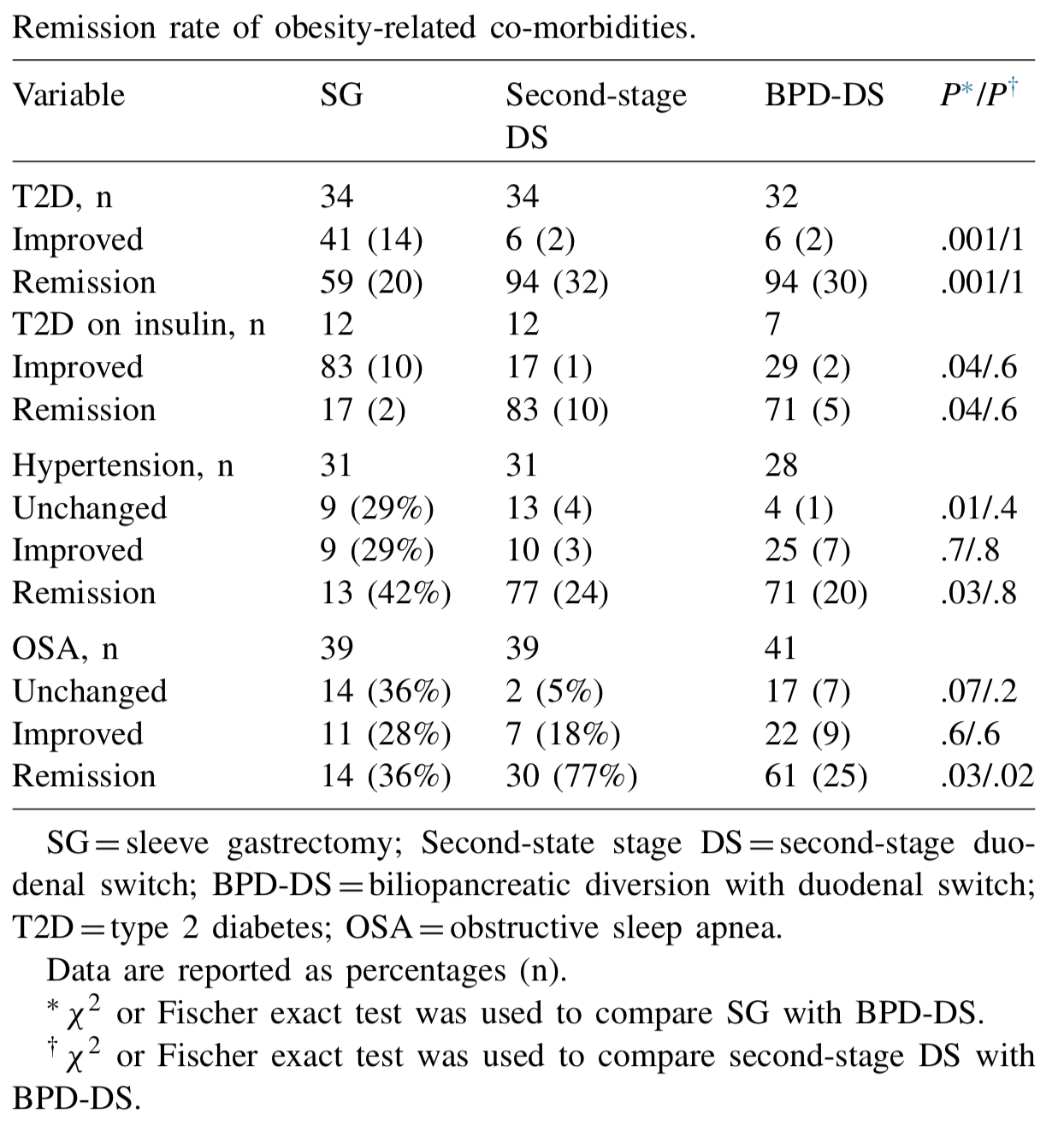
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss. 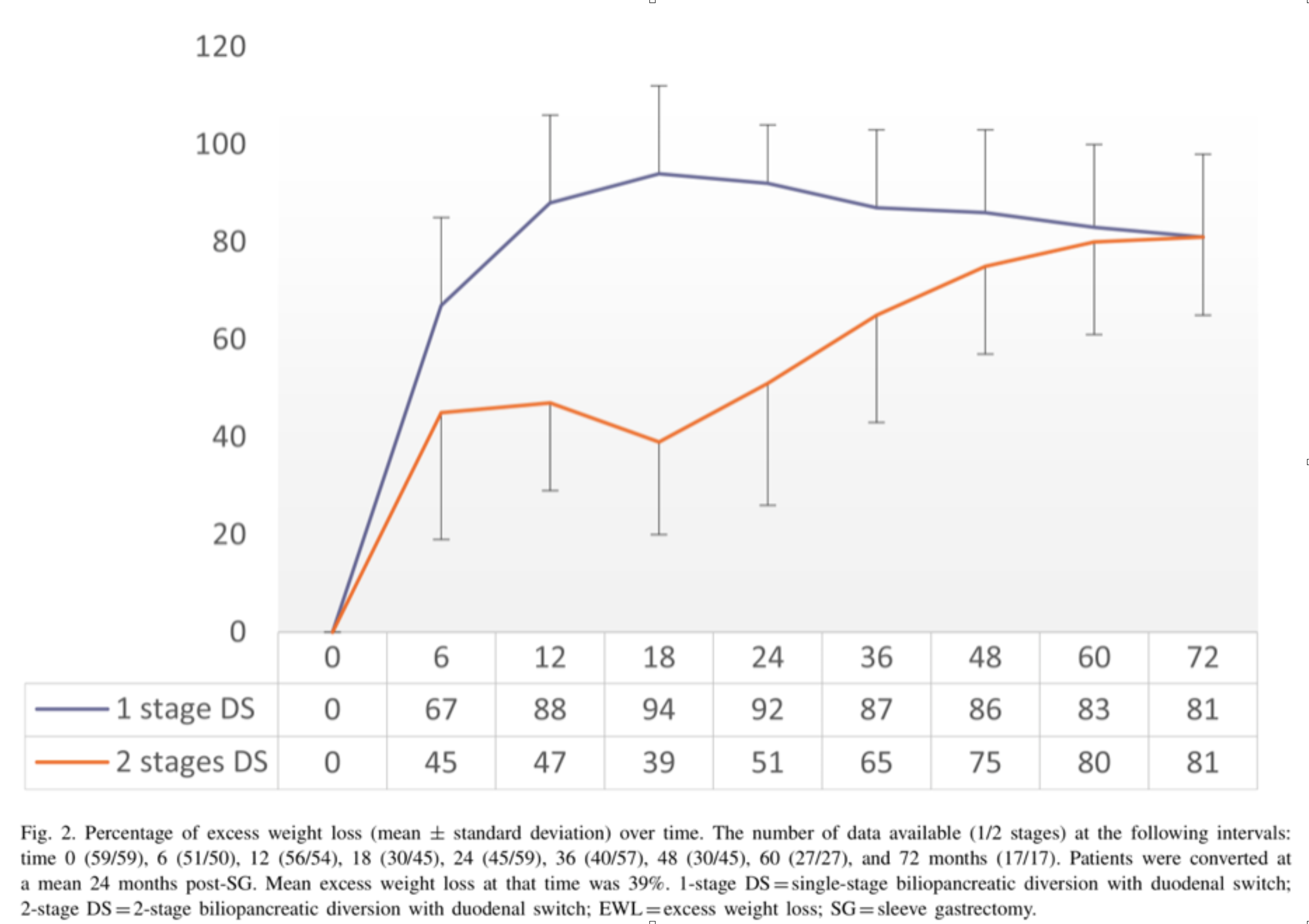
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.
Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP
PolyCystic Ovarian Syndrome PCOS
September 04, 2018 9:58 am
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.

Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
Bariatric Surgery can improve PCOS in those individuals with Type 2 Diabetes Mellitus. Further information on weight loss surgery and its effect on PCOS here.
Revision from failed AGB to Duodenal Switch
January 10, 2018 2:10 pm
A few times a month during consultation for weight loss surgery , I’m ask as to why I do not offer the adjustable gastric banding as an alternative to the patients. As I have said over the years when a patient considers an weight loss surgery the totality of the risk should be considered. This includes the operative, immediate postoperative course, the maintenance and the follow-ups needed. The potential complications of the procedure in addition to the long-term success off each operation should also be taken into account.
Unfortunately, some patients are led to believe that any perceived benefit in the short operative time and the ease of the adjustable gastric banding also translates to a better outcome. This is in fact the opposite of what the published data have shown, a recent study published in April 2017 by Vinzes et.al, shows that 71% of patient lost their band by 10 years out.




What is also interesting that more patients underwent revision from failed AGB to the duodenal switch than the sleeve gastrectomy (Fig 1.). This is what I also recommend.
More importantly, The patients who underwent a revision from failed AGB to the duodenal switch operation had the best long term results of all patients (Fig 2.) note the “rBPD” line that is the highest of %EBMIL.
Complication’s were broad and frequent (Table 3.)
Further information on revision from failed AGB to Duodenal Switch or other failed weight loss surgeries can be found here.
Long Term Complications of Adjustable Gastric Banding
October 17, 2017 6:35 am
It is interesting to encounter patients who are still being recommended for Lap Band placement to treat morbid obesity. There is a vast body of scientific evidence supporting that Lap Band not only does not result in a sustained weight loss for majority of the patients, but that it results in significant long term complications for some.
One of the complications is a significant stricture (narrowing) where the band is located even when it is completely empty. This is cause by:
1- either scarring of the tissue around that band causing a “belt” effect around the stomach, or


There are numerous other complications that are associated with Adjustable Gastric Bands that encompass a wide range of areas that are not discussed in this blog. This recent article (yes another one) outlines the dismal long term outcome of the Adjustable Gastric banding- Buyer Beware.
https://www.dsfacts.com/pdf/agb-long-term-results-1506834076.pdf
Gastric Band Complications
June 21, 2017 10:22 am
For years, we have seen patients who have had Adjustable gastric bands placed and continue to suffer from the complications associated with it. Gastric Band complications include erosion, persistent nausea, vomiting abdominal pain, inadequate weight loss and weight regain, etc. . Unfortunately, when seeking help, they are often told that this never happens to others and that complications are a rare occurrence. Let’s remember that the Adjustable Gastric Band was promoted and sold as a procedure with almost no down side, low risk and easily revisable!
There is an unfounded expectation that the band can be deflated and all the Gastric Band complications will resolve. This could not be any further from the truth. The reality is that there are patients whose symptoms may somewhat improve but will continue to have the abdominal pain, the nausea and or vomiting-albreit, not to the same intensity. There are several Gastric Band complications that are considered emergency situations that require immediate attention by a physician.
Our position has always been, and continues to be, that all Adjustable Gastric Bands should be removed by a surgeon who is experienced with the Gastric Band complications and revisions.
")
")
")
Slipped Band Emergency
April 27, 2017 12:35 pm
A slipped Band emergency
This patient had a Adjustable Gastric Band (AGB) or LapBand place approximately 7 years ago. The last time this patients had a follow up with the surgeon who placed the AGB was 5 years ago. The patients has been having reflux, episodes of Nausea and vomiting on and off for about 2 years requiring multiple medical visits and procedures. He/she has had upper endoscopies, not by the surgical team and was diagnosed with esophagitis.
This patient presented in the Emergency Room with projective vomiting for 24 hours, bloody emesis, and significant dehydration. After obtaining the necessary tests and X-ray studies a plan was constructed. At this time, due to the continuous and significant nature of the symptoms this patient was taken to the Operating Room for emergency AGB removal.
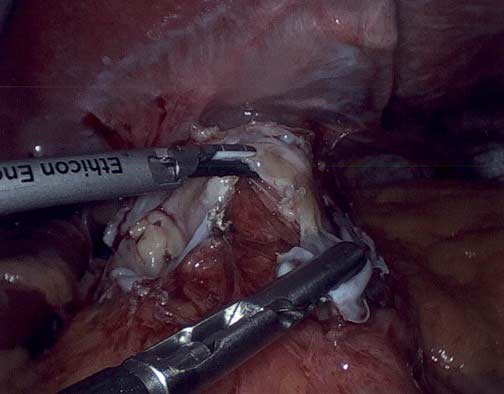
The abdominal X ray showed a slipped band. Following a complicated surgical procedure, the band was removed and a segment of the stomach that had eroded into the stomach was removed. The photograph below shows the end result with a portion of the stomach removed due to the band’s erosion into the stomach.
Additional information regarding complications of Adjustable Gastric Banding here.
We have several Adjustable Gastric Banding related surgical videos here under the heading of
“Band Related”, including a slipped band emergency video.

