Tag: revisional weight loss surgery
Bile Reflux Gastritis
May 19, 2026 4:13 pm
Hello, it’s best to clarify a few points:
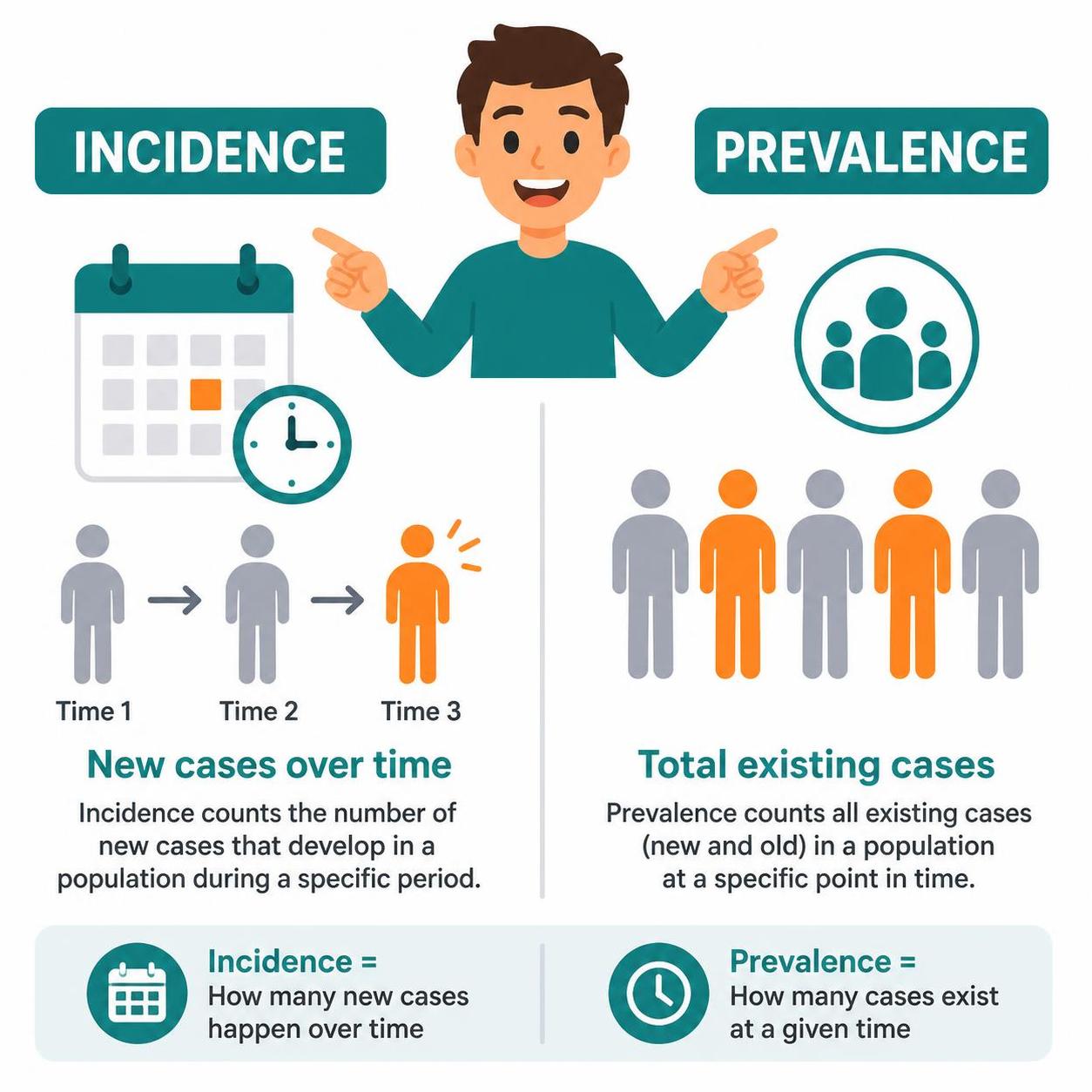
- The difference between prevalence and incidence.
- Incidence means new cases over
- Prevalence refers to existing cases at any time
- The difference between causation, coexistence, and correlation
- Causation refers to a condition causing an effect.
- Coincidence refers to two conditions present together at the same time, with neither causing the other.
- Correlation refers to two conditions that may occur together, with no causation.
- Study size refers to the research data on which the information is based. The larger the population size studied, the better the sample data and the more conclusive the results.
- Confounding factors.
Staples Used in Gastrointestinal Surgery
February 11, 2025 11:23 am
I have frequently been asking what staples are used in sleeve gastrectomy. A stapling device is used with sleeve gastrectomy. This device comes in different shapes and sizes for different bowel thicknesses and applications. However, they all function the same way. The staple cartridges (the part of the stapler that is replaced after each use with a new one) are selected based on the thickness of the segment of the bowel that needs to be stapled and divided.
The stapling and dividing take place simultaneously. The sampler deploys six rows of staples and cuts between them, leaving three rows on one side and three on the opposite side. With the sleeve gastrectomy, this means that the sleeve stomach that is left has three rows of staples, and the segment of the stomach that is removed also has three rows of staples.

1-Can I have a CT or an MRI done? Yes, The titanium staples are safe for both CT and MRI.
2-What are they made from? The staples are made of titanium and alloys, which are non-reactive and safe.
3-How big are the staples? Different staples are of different sizes, mainly in the mm range; see the tip of the pencil in the image for the relative size.
Video of stapler demonstation here

COVID Vaccines
March 05, 2021 3:50 pm
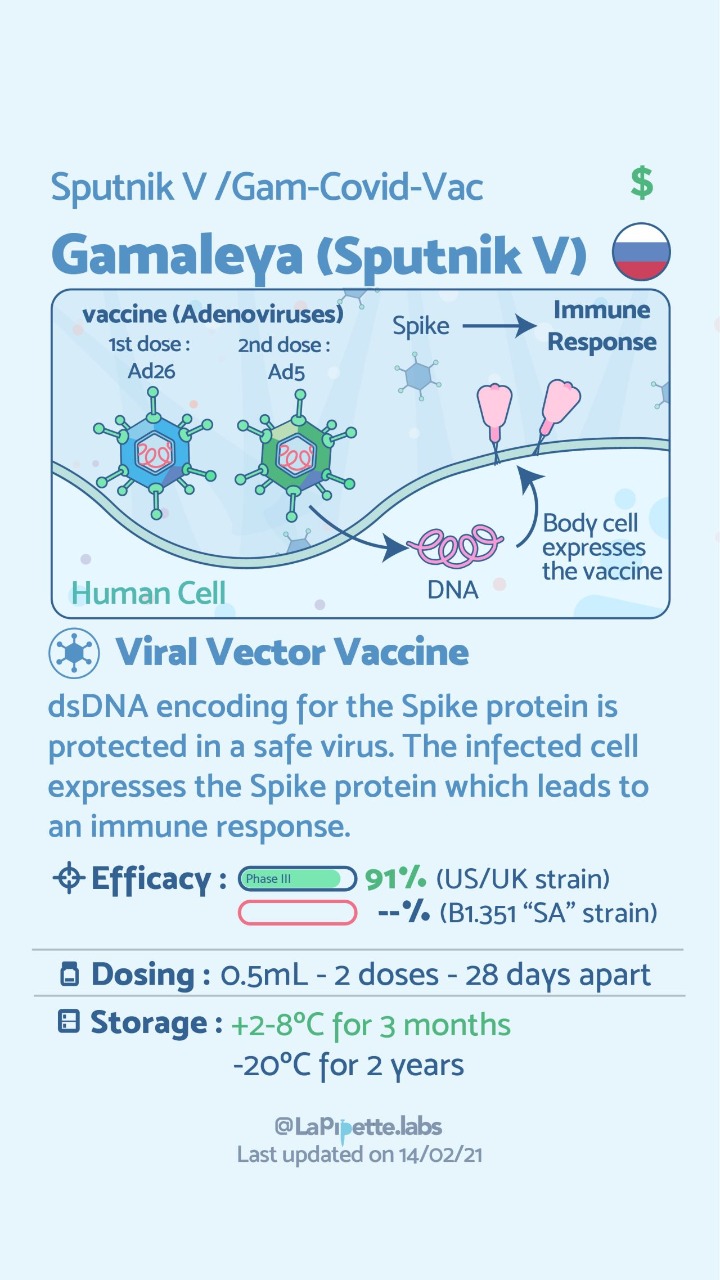
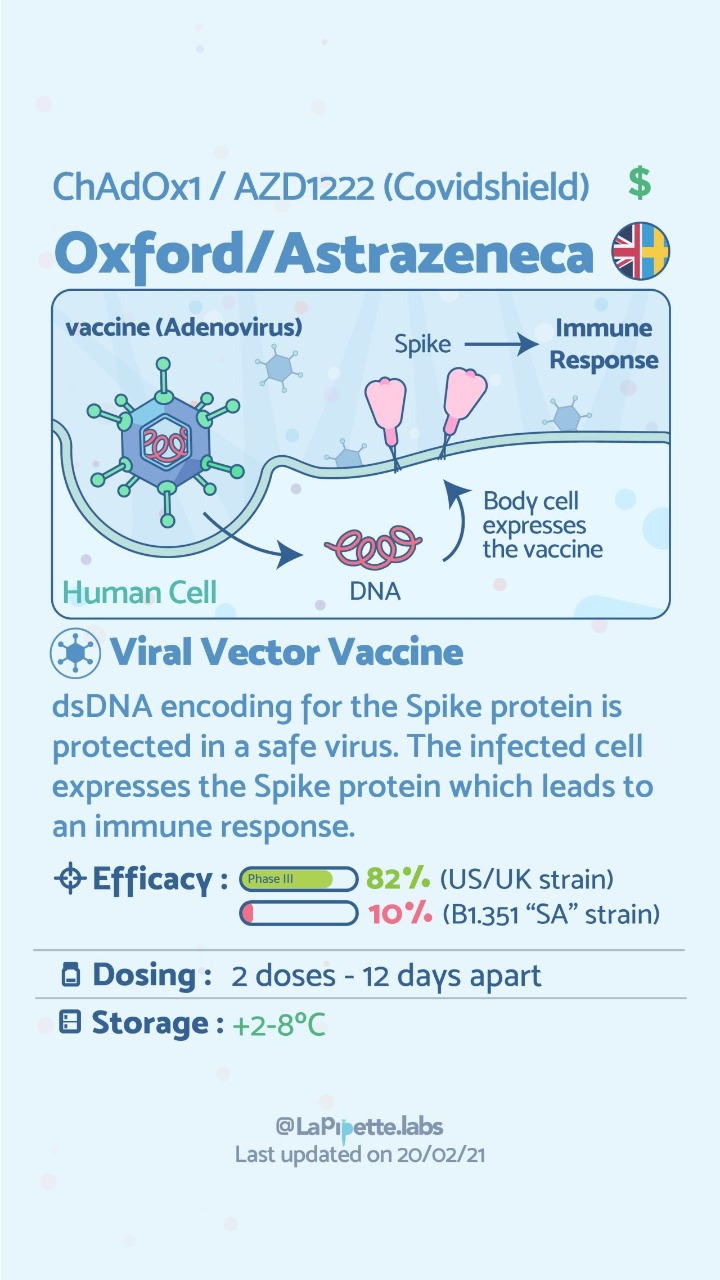
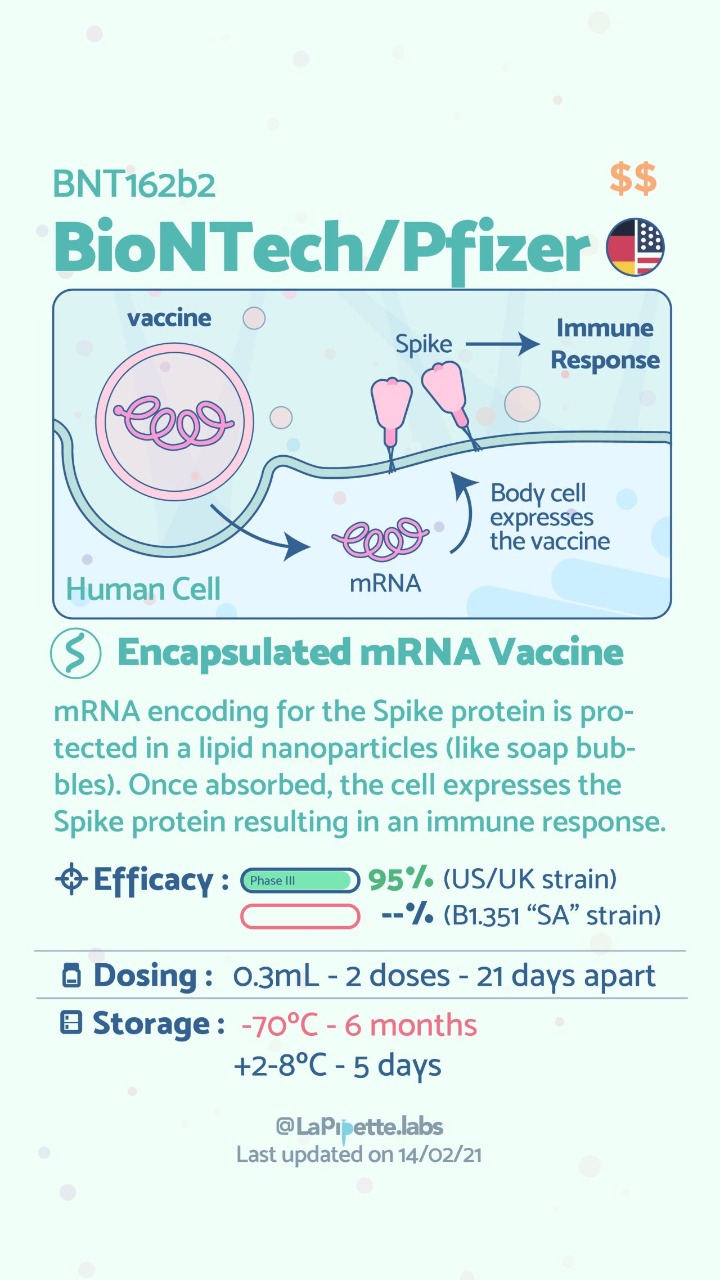
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
Copper Metabolims And Weight Loss Surgery
May 01, 2020 12:31 am
Written By: Osheen Abnous, Maria Vardapetyan, Eric Baghdasaryan
Copper is an essential element to all organisms, and it is a contributor in several enzymes vital to the function of hematopoietic, vascular, and skeletal tissues, as well as the structure and function of the nervous system.
As a crucial metal, copper plays an important role in chemical reactions throughout the human body; this includes the central nervous system. Enzymes are substances that facilitate chemical reactions. There are many copper-dependent reactions in the human body. In humans, the major site of absorption of dietary copper is still unclear. Copper in humans is absorbed in the proximal small bowel, duodenum, and ileum. This is after it has passed the acidic environment of the stomach.
Copper deficiency can be caused by malnutrition, prematurity, parenteral or enteral feeding without copper supplementation, gastrectomy, and excessive zinc therapy. The common causes of copper deficiency have been zinc supplementation, and changes to the PH (acidity) of the stomach. This can be the result of the alteration of the stomach anatomy, and by chronic acid suppression by proton pump inhibitors (antacids), and similar medications. Physicians need to be alert with patients who show signs of copper deficiency or are at a high risk of developing a copper deficiency.
It is important to raise greater awareness about copper deficiency because there is a growing number of patients undergoing surgeries for obesity, as the occurrence of copper deficiency will increase in the future.
Studies of patients who have had weight loss surgery in the past experience common symptoms such as pain involving the feet, gait abnormality (unusual walking), lower limb weakness, and recurrent falls. Common lab results include unusually low serum copper and serum ceruloplasmin levels. In some cases, elevated zinc levels are also present. Treatment includes cupric sulfate infusion until normal copper levels are reached, which then need to be maintained for the future. Vitamin B-12 deficiency has also been reported as a possible cause of myelopathy, which is a nervous system disorder that affects the spinal cord. As stated earlier, neurological damages are often irreversible and cause permanent damage to patients. Early diagnosis from physicians is crucial for patients who have undergone gastric bypass surgery, and the sooner they are diagnosed, the less permanent damage the patient will endure.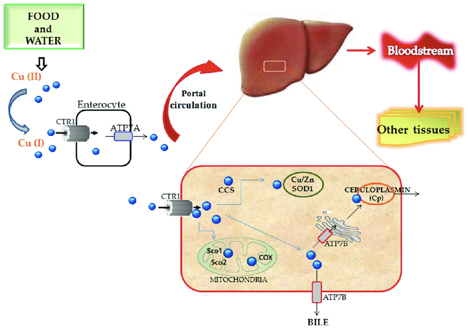
Case Discussions:
A 49-year-old woman had gastric bypass surgery for obesity 24 years age. She presetend with increasing lower limb stiffness and numbness. Additionally she reported tingling of the feet. As her pain continued to increase, she began using a walker, and her symptoms continued to worsen. After undergoing a neurological examination, results showed that the patient had increased lower limb tone and an absent perception of vibration at the toes and ankles. Laboratory results showed that the patient had copper levels barely detectable. This included serum copper and serum ceruloplasmin levels. In addition, the patient had reduced serum carotene (vitamin A) levels.
The patient received cupric sulfate intravenously daily through an 8-week period. After each daily infusion of cupric sulfate, the patient reported to have slight decreases in numbness and an increased tingling sensation. After the 8-week period, lab results showed that serum copper levels were normal and are needed to be maintained. Her night blindness was corrected by vitamin A injections.

In another case, a 53-year-old woman had symptoms of abnormal gait (abnormal walking) and anemia (lack of healthy red blood cells), and was seen for evaluation. The patient complained of pain in the lower legs, which would worsen over time and move up towards her thighs. As her ability to walk continued to worsen, the patient resorted to using a wheelchair. Her medical history consisted of an RYGB surgery for obesity. The only significant supplementation she received was 1000 μg vitamin B12 subcutaneously for several years. She had absent positional and vibratory sensation in the lower extremities to the knee. In addition, touch sensation was decreased. Laboratory examination revealed an elevated serum zinc level, and extremely low serum copper and ceruloplasmin levels.
For treatment, the patient received intravenous copper over a 6-day period, was discharged home, and then received weekly intravenous copper infusions thereafter. After a month of receiving intravenous copper, serum copper levels returned to normal. In addition, the patient’s pain in the lower leg improved, but vibratory sensation remained absent in the same area. Four months after being discharged from the hospital, the patient began walking with a cane.
Fat Soluble Vitamins
April 26, 2020 10:20 am
Written By: Maria Vardapetyan, Eric Baghdasaryan, Osheen Abnous
Vitamins are chemicals that facilitate many processes in the human body such as blood clot formation, good vision, fight infections etc. There are two classes of vitamins. Water soluble vitamins and fat soluble vitamins. Water soluble vitamins dissolve in water. This makes it possible for them to be absorbed through all mucous membranes. Fat soluble vitamins on the other hand do not dissolve or pass through mucous membranes. Fat-soluble vitamins are absorbed in the intestine along with fats in the diet. These vitamins have the ability to be stored in the fat tissues of the human body. Water-soluble vitamins are not stored in the body and have to be taken in daily with the food and dietary supplements. Solubility of a vitamin is not a function of its physical state. There are fat soluble vitamins that have a liquid form and almost all of the water soluble vitamins come in form of pills or powders.
In this article, we are going to focus on fat soluble vitamins. They are all complex molecules made of carbon, hydrogen, and oxygen in different arrangements (see figures 1, 2, 3 and 4). These fat soluble vitamins are vitamin A, D, E and K.
Vitamin A
Vitamin A has a major role in vision, immune function, cell growth, and maintenance of organs such as heart, kidneys, lungs, etc. It plays a pivotal role in the health of our eyes, specifically the retina1. Rhodopsin protein, a major protein that has the leading role in the process of vision, is found in the retina where it allows us to perceive light. This protein requires vitamin A to function properly. Without vitamin A, rhodopsin cannot sense light and thus cannot initiate the process by which vision occurs.

Figure 1: Chemical structure of Vitamin A molecule
Vitamin D
Vitamin D regulates different chemical reactions that are associated with bones, muscles, and the immune system. The simplified way it does this regulation is it helps absorb calcium from dietary nutrients which in turn strengthens the bones, helps neurons exchange signals to move muscles and helps the immune system to fight against viruses and bacteria2.
 Figure 2: Chemical structure of Vitamin D molecule
Figure 2: Chemical structure of Vitamin D molecule
Vitamin E
Vitamin E acts as an antioxidant. Antioxidants are naturally occurring chemicals that neutralize toxic byproducts of many chemical reactions in the human body. When food is consumed and digested, the human body converts it into energy. As a result of metabolism free radicals (toxic byproducts) are formed and are neutralized with the help of vitamin E. In addition, free radicals are also in the environment. Furthermore, vitamin E stimulates the immune system to fight against bacteria and viruses3.
 Figure 3: Chemical structure of Vitamin E molecule
Figure 3: Chemical structure of Vitamin E molecule
Vitamin K
Vitamin K can be obtained from food and dietary supplements. There are two forms of vitamin K: phylloquinone (Vitamin K1), which is found in spinach, kale and other greens and menaquinone-4 (Vitamin K2), which is found in animal products. Vitamin K1 is involved in blood clotting, and Vitamin K2 is involved in bone tissue building. Vitamin K1 is the main Vitamin K in human diet (75-90% of all vitamin K consumed), however, it is poorly absorbed in the body4,5.

Figure 4: Chemical structures of Vitamin K1 and K2 molecules
Absorption of fat soluble vitamins
Polarity describes the inherent charge(positive or negative) or lack of charge for any given substance or molecule. Molecules that are charged are referred to as “polar”, while those that lack charge are “nonpolar”. When discussing solubility, it is important to remember the phrase “like dissolves like”. That means polar (charged) substances like to interact with a polar environment like water, since water contains a slight negative charge. Hence, charged substances are water-soluble. Nonpolar substances on the other hand readily interact with nonpolar environments such as fat, which contains no charge. Therefore, molecules that lack a charge such as vitamins A, D, E, and K are referred to as fat soluble.
Due to their water fearing nature, these fat soluble vitamins cannot simply be absorbed directly into the bloodstream (which is mostly water) like the sugars and amino acids in our diet. As their name suggests, these fat soluble vitamins like to be embedded in fatty droplets, which facilitate their absorption in the following way. Fat soluble vitamins group together with other fat molecules to form fatty droplets, effectively reducing the amount of interaction with the watery environment of the intestines. Therefore, without an adequate amount of fat in your diet, your body is unable to effectively absorb these fat-soluble vitamins. This may be true in an intact anatomy, however, post weight loss surgical patients can not increase their fat soluble vitamin levels by increasing their fat intake. This is due to the fact that a high fat diet causes excessive bowel movement which in turn washes away any vitamins taken by mouth. DS limits fat absorption (thus the great weight loss) which can cause vitamin A and D deficiency that can not be easily corrected with oral supplementation.
As mentioned before, fat soluble vitamins are hydrophobic and nonpolar, which means they are also fat loving or lipophilic. Excess fat soluble vitamins can be stored in the liver and fat tissue. Therefore, these vitamins do not need to be eaten every single day since stores of these vitamins can sustain a person for some time. It may take several weeks or months for our body to deplete these stores of fat soluble vitamins which is why it generally takes a longer amount of time for fat soluble vitamin deficiencies to manifest themselves. The ability to store these fat soluble vitamins in tissues can also lead to vitamin toxicity – marked by an excess of vitamin stores in our body.
Clinical manifestations of A, D, E, K deficiency
| Vitamin | Clinical Deficiency manifestations |
| Vitamin A | Vision Problems
Dryness of the eye |
| Vitamin D | Softening and weakening of the bones
Bone shape distortion Bowed legs (generally in children) Hypocalcemia |
| Vitamin E | Damage to red blood cells
Tissue/organ damage due to inability to supply enough blood Vision problems Nervous tissue malfunction |
| Vitamin K1 | Excessive bruising
Increased bleeding time Small blood clots under nails Increased bleeding in mucous membrane |
| Vitamin K2 | Weak bones
Increased plaque deposits along gumline Arterial calcification |
References
- Office of Dietary Supplements – Vitamin A. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/#. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin D. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminD-Consumer/. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin E. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminE-Consumer/. Accessed April 26, 2020.
- Vitamin K. The Nutrition Source. https://www.hsph.harvard.edu/nutritionsource/vitamin-k/. Published July 2, 2019. Accessed April 26, 2020.
- Beulens JWJ, Booth SL, van den Heuvel EGHM, Stoecklin E, Baka A, Vermeer C. The role of menaquinones (vitamin K₂) in human health. The British journal of nutrition. https://www.ncbi.nlm.nih.gov/pubmed/23590754. Published October 2013. Accessed April 26, 2020.
Diabetes and Weight Loss Surgery
April 06, 2020 5:51 am
The scientific literature is riddled with evidence pointing to the benefit of early metabolic surgery as a superior treatment, remission and possible cure option for diabetes. Unfortunately, the medical education, pharmaceutical companies, primary care healthcare delivery systems and third party payers (health insurance companies) have not caught up with the published data. The American Diabetes Association has changed their guidelines to reflected the benefit for combating diabetes with weight loss surgery.
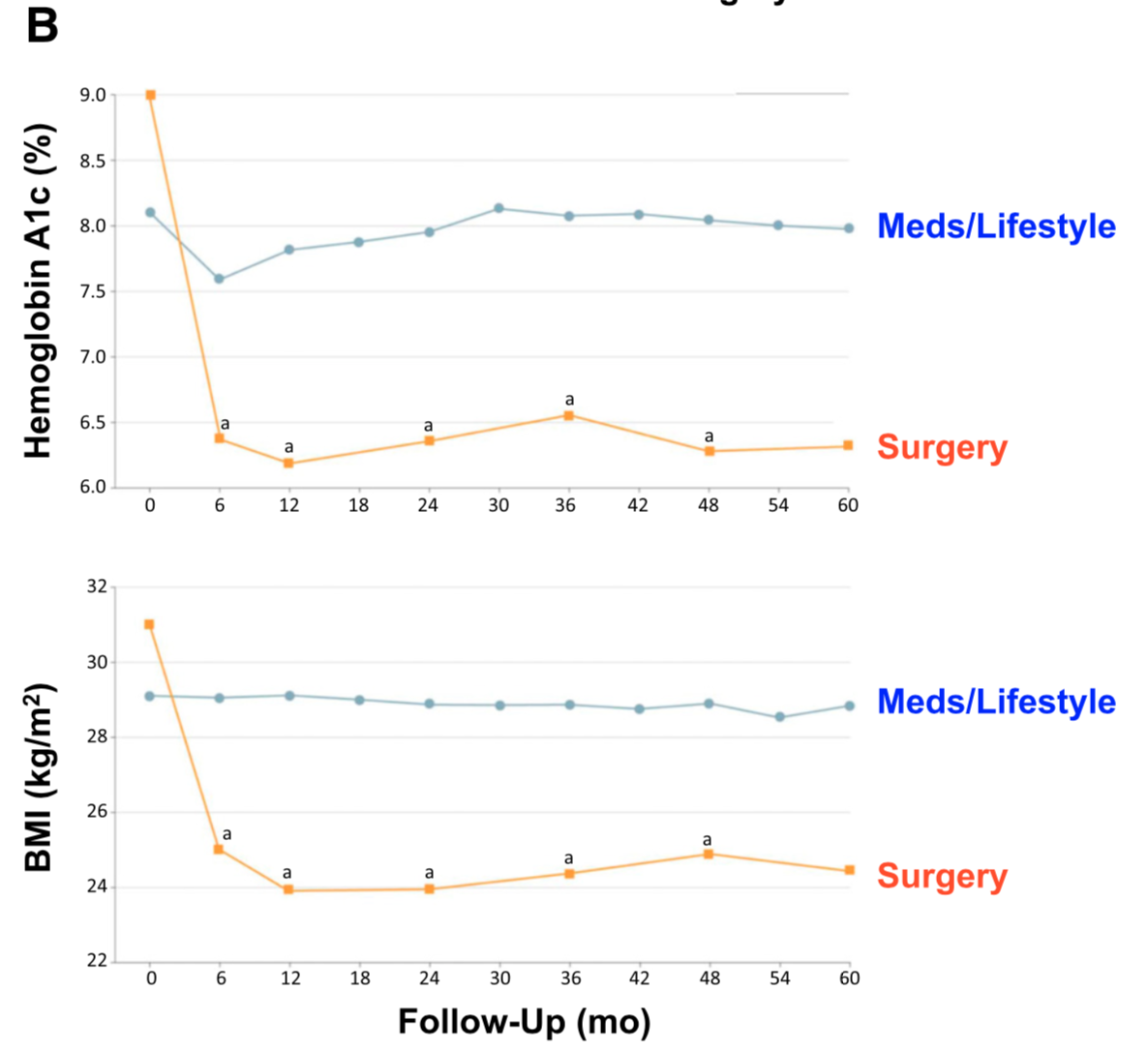
There is ample evidence of the superior outcome of surgery as a treatment option for diabetes when compared to medical managment. Cummings et.al, in a published article in Diabetes Care, showed sustained stabilization of the Hemoglobin A1C six years after surgery. In contrast, there was no significant changes noted in the non-surgical group.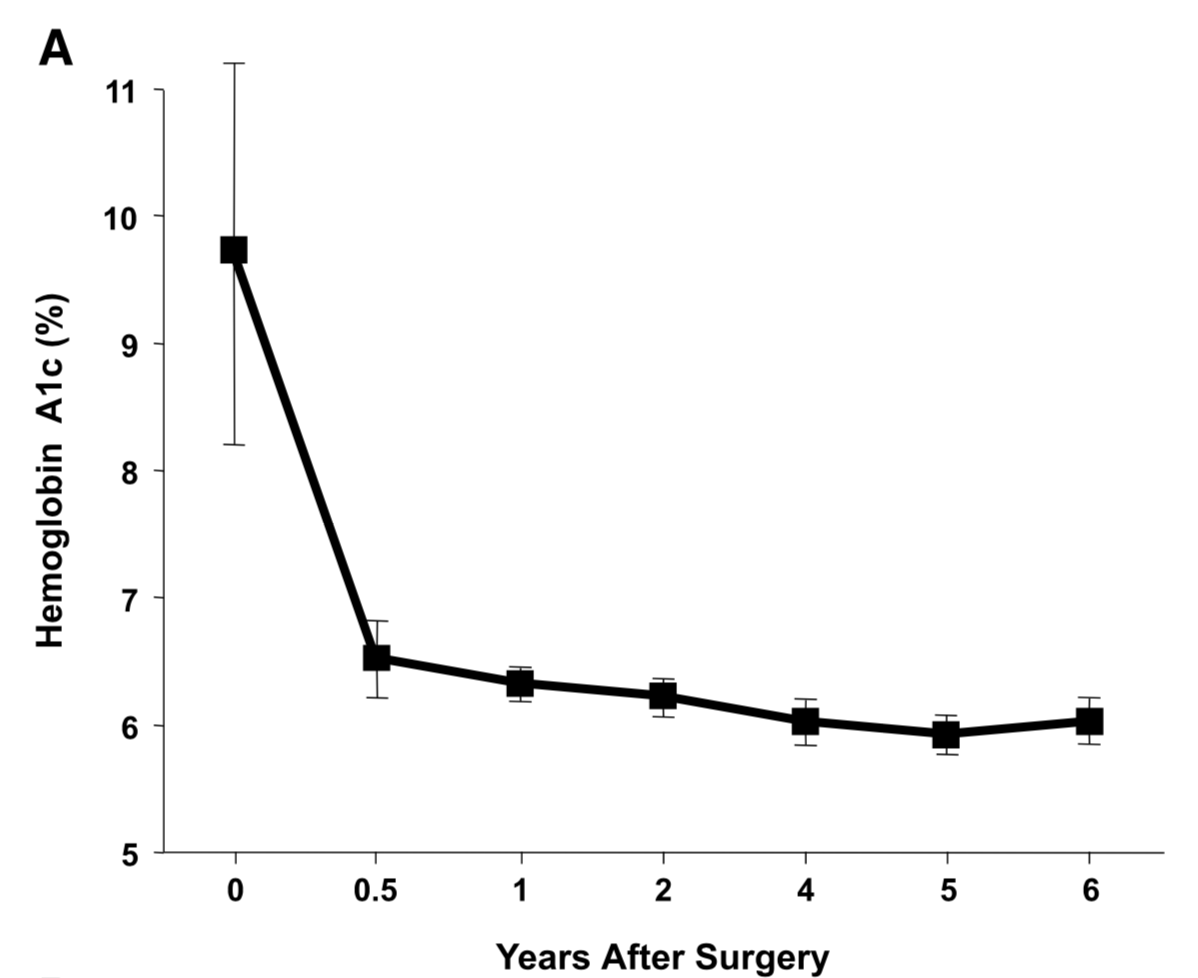
Jans et.al. , in November of 2019 showed that the patients who had NOT been on Insulin, and had metabolic surgery had the highest long term success for resolution and remission of the diabetes. This identifies that having a patient be proactive in their care by having metabolic surgery improves success rates.
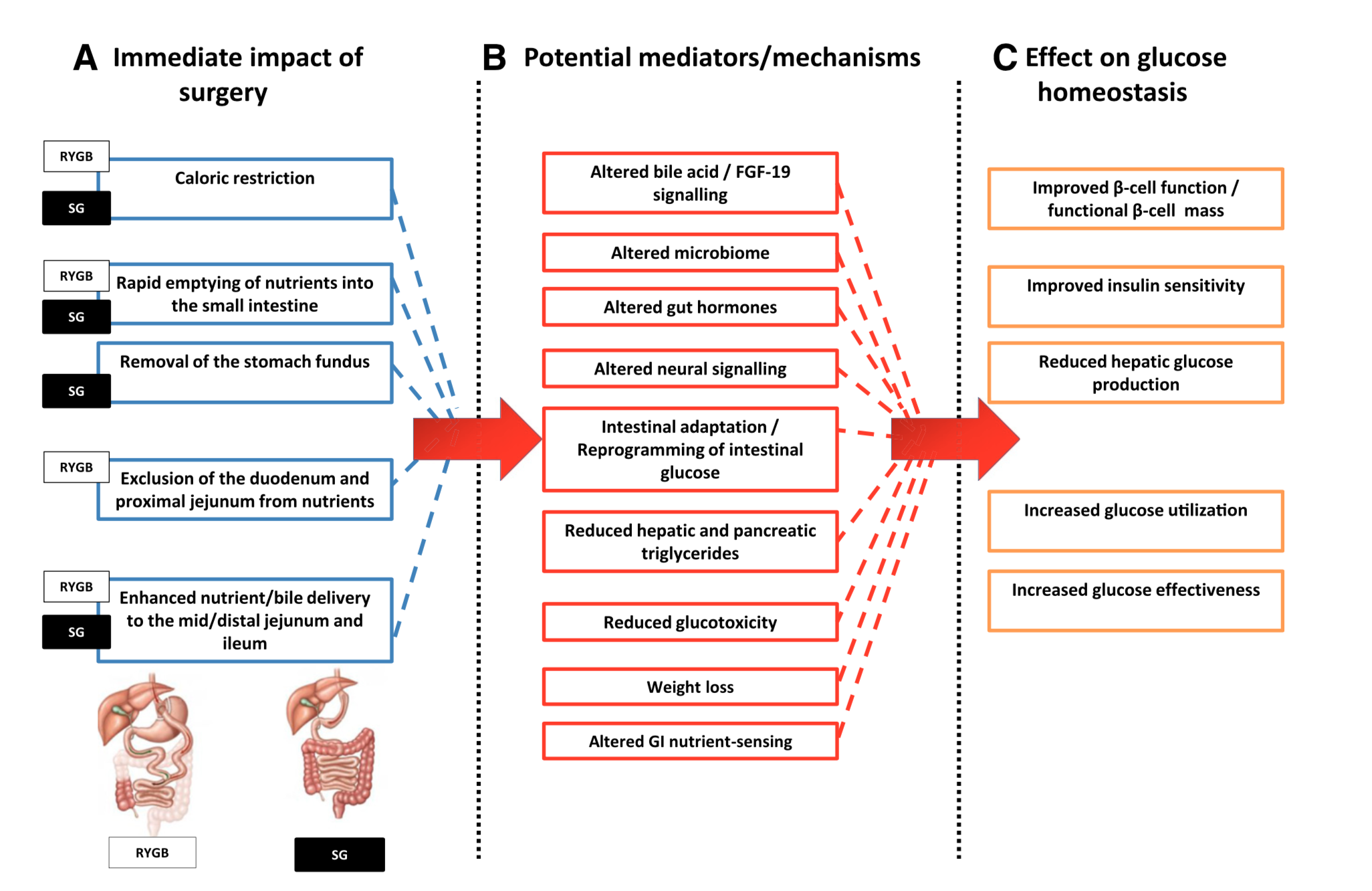
The exact mechanism by which the diabetes is resolved is unclear. The weight loss may play a role. There are numerous hormones and neuroendocrine modulators which control the complex metabolic pathways. Batterham et.al., in Diabetes Care (2016), published a summary overview of the possible mechanism involved in diabetes improvement following metabolic surgery.

There are a number of overlapping and sequential layers for possible reasons why diabetes resolves after weight loss/metabolic surgery. These may be directly related to surgery and the reduction of the calorie intake or absorption. It may also involve the neuroendocrine modulators.
What can be said definitively is that early surgical intervention is best and most likely the only permanent solution to type II diabetic resolution. There is no medical justification in not considering metabolic surgery in diabetic patients who may also have difficulty with meaning a BMI< 35.
Length of Bowel : Hess or No Hess
March 22, 2020 5:58 pm
“…What is the length of my common channel” is probably one of the frequently asked questions about the duodenal switch operation in the office. This usually comes up at the initial consult when patients repost credible sources such as Dr. Google and Dr. Facebook for patient with different bowel length have done well or not so after duodenal switch operation. Dr. Hess described the Duodenal Switch by using total bowel length measurements and creating the common channel as a percentage of the total small bowel length. However, it seems that this is being done less and less.
This leads to my explanation that is on the website
Hess calculator : Bowel Length Calculator
How the actual measurements matters: Bowel length video link
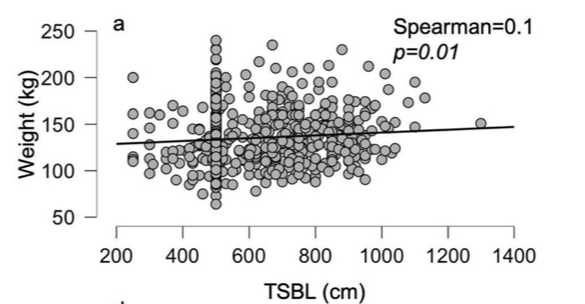
In 2019, Bekheit et.al published a very interesting study comparing total small bowel length (TSBL) to a number of variables such as height, weight, sex and BMI. They identified a few loose correlations. Male patient have longer TBSL than females. There was correlation between TSBL and height stronger in males than females but not statistically significant.
In Conclusion they reported ” Despite statistical significance of the correlation between the TSBL and the height and weight of the included participants, the correlation seems to have no clinical meaning since the effect size is negligible. ”
As I have previously discussed this Making the common and alimentary length standard for every duodenal switch patient will make some loose too much and other not enough weight.
Figure 1 shows TSBL on the horizontal axis, and height, weight, BMI and Age on the vertical axis. For the most part what they all show is that one can not predict how long a patients bowel is by any of the measures that we take in the office as a part of the routine exam.
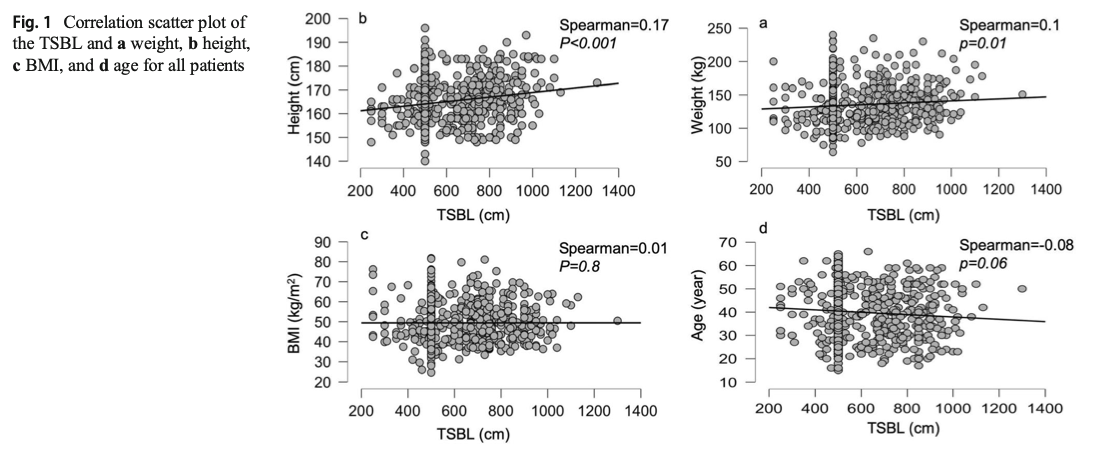
This raises, the concerns that I had raised previously. How could two similar patients who have the same weight, age, sex and BMI have the same surgery and expect the same result if one of them has TSBL of 400 cm and the other one 800cm?
Sleeve And Weight Regain
July 22, 2019 9:50 am
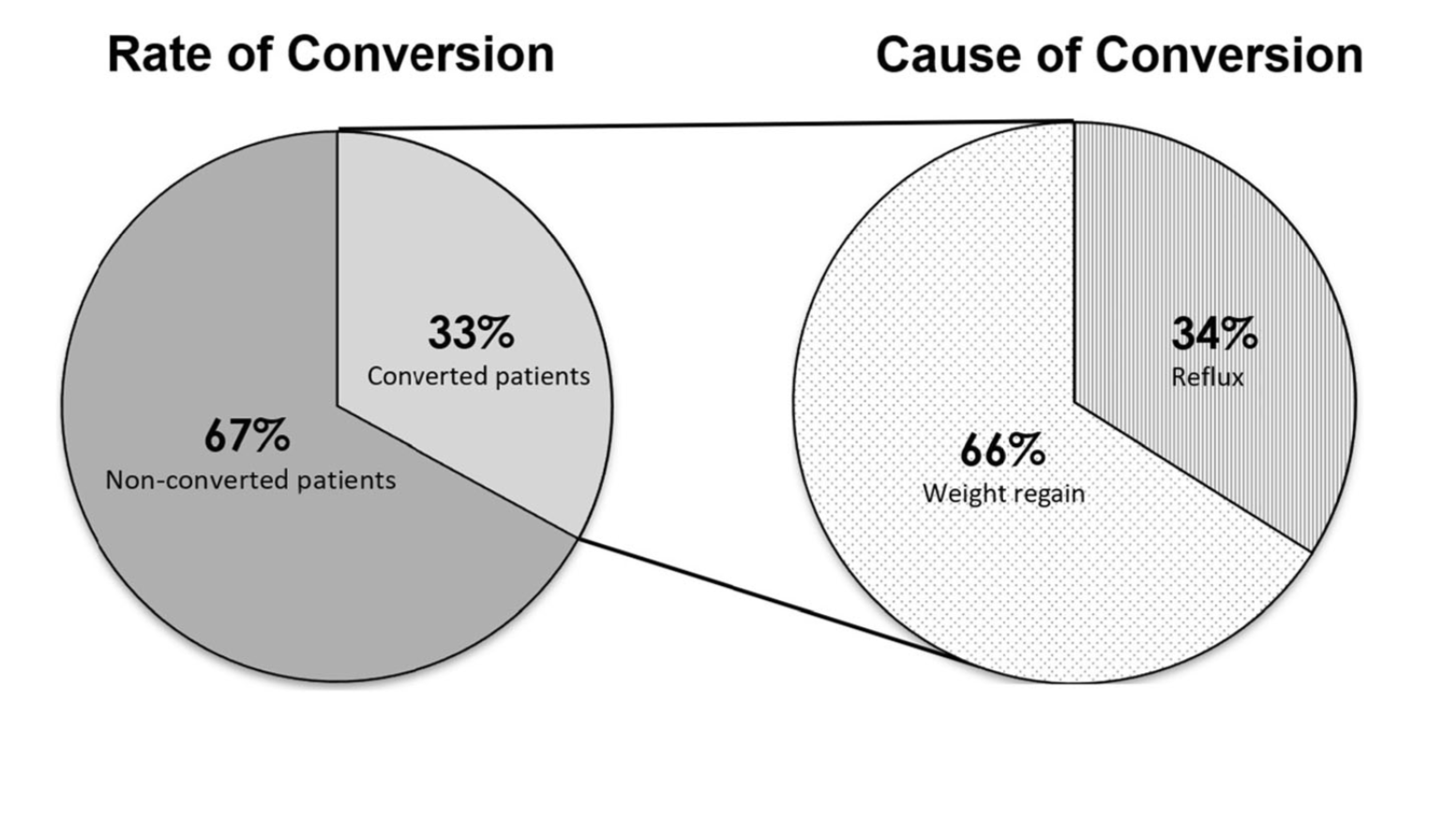
Sleeve Gastrectomy Failure
May 07, 2019 12:53 pm
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
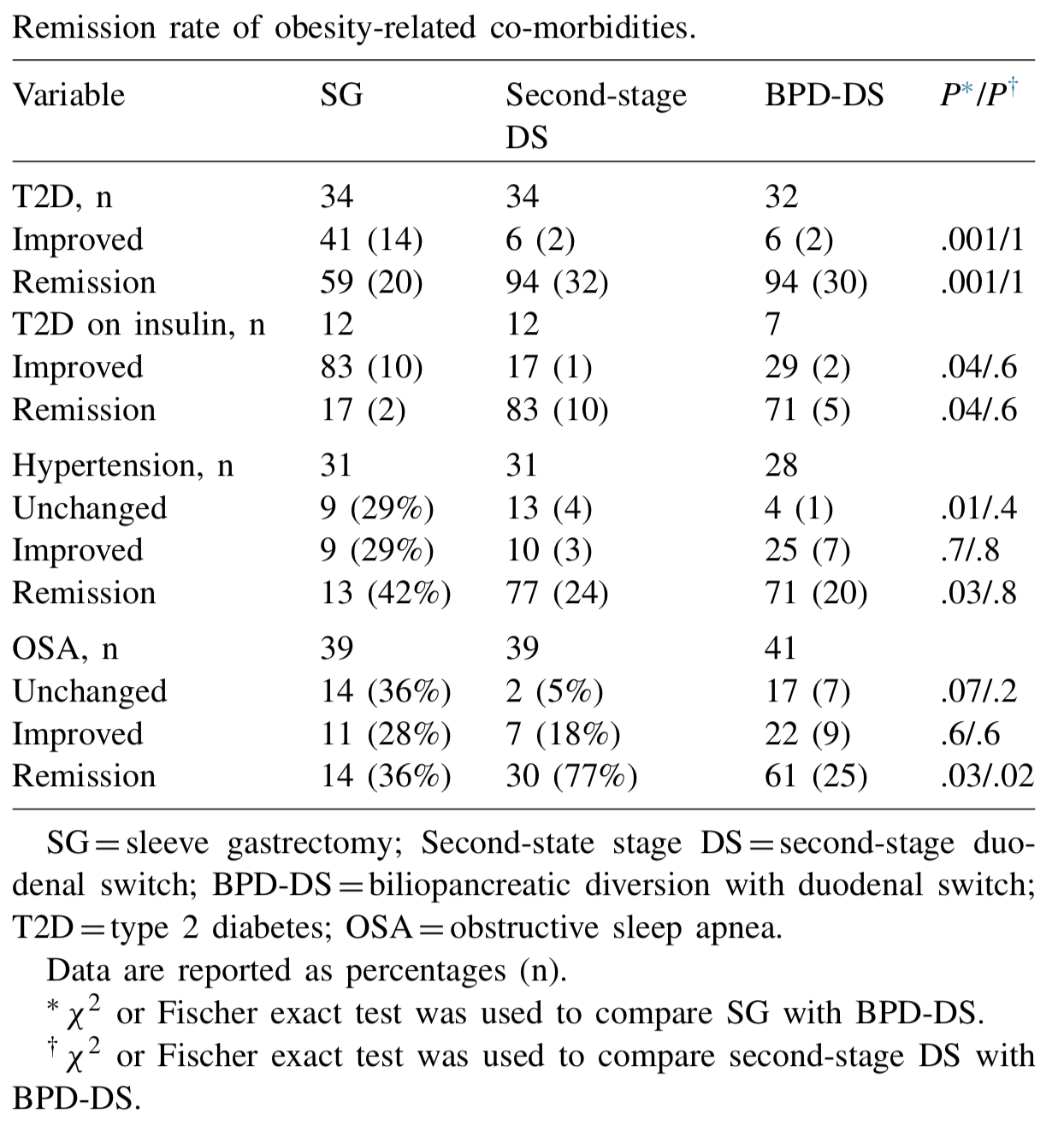
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss. 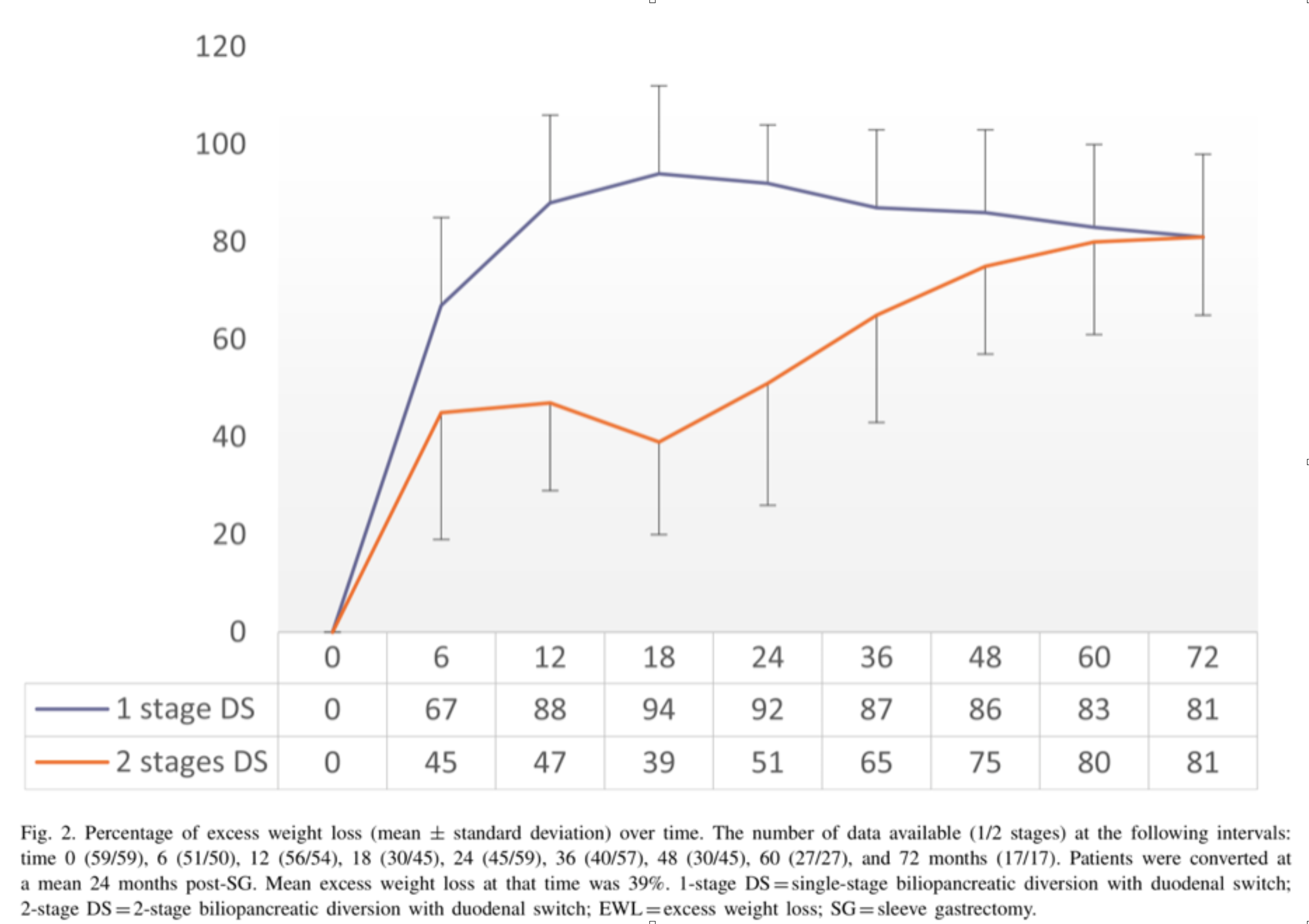
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.