Category: calcium
Types of HyperParathyroidism
February 20, 2026 4:05 pm
There are 4 parathyroid glands which are located behind the thyroid gland, among other functions, are the main regulators of calcium, phosphorous, and magnesium in the blood. Elevations of parathyroid hormone (hyperparathyroidism) can be: 1-Primary, 2-Secondary, 3-Tertiary

Primary hyperparathyroidism means the parathyroid glands themselves are hyperactive. This may involve only one of the four glands: a) an adenoma, a benign tumor that needs surgical removal, or b) hyperplasia, when all 4 glands are hyperactive and/or enlarged, and in some cases, most of the 4 glands need to be removed.
Secondary hyperparathyroidism means that the elevated PTH level is caused by an external regulatory stimulus, such as low calcium, which itself may be due to low vitamin D, low calcium intake, or other causes.
Tertiary hyperparathyroidism is seen only in specific renal failure and transplant patients.
Regardless of the type of hyperparathyroidism, the end result is the same. Because the parathyroid gland aims to maintain normal calcium levels, it will do everything to achieve them. This includes increasing calcium absorption from the GI tract, breaking down bone to increase the blood calcium supply, and increasing calcium reabsorption from the urine.
Distinguishing between primary and secondary is critical, as primary is more likely than not a surgical problem that needs to be addressed. Secondly, it may be responding to metabolic deficiencies (low CA, low Vitamin D) that need to be corrected and take some time.
Not all cases require surgical intervention, as labs (vitamin D, calcium, and alkaline phosphatase) and imaging studies, such as neck ultrasound, CT scan, and Sestamibi scan, provide the information needed to dictate the treatment plan. Please stay up to date with your yearly lab results to catch changes sooner rather than later.
Vitamin D and COVID 19
June 13, 2020 4:40 pm
There has been extensive discussion on the importance of Vitamin D published over the last few years in regards to bone health, immune health and Calcium physiology. The importance of vitmain D and bone structure has been discussed extensively. It is also important in the absorption of Calcium. It further plays role in immune modulation.
What is new is the possible correlation of Vitamin D and COVID 19. Recently it is been shown that low vitamin D may increase the risk of a poor outcome with Covid-19 exposure and infection.
There are different standard recommendation for the Vitamin D levels.
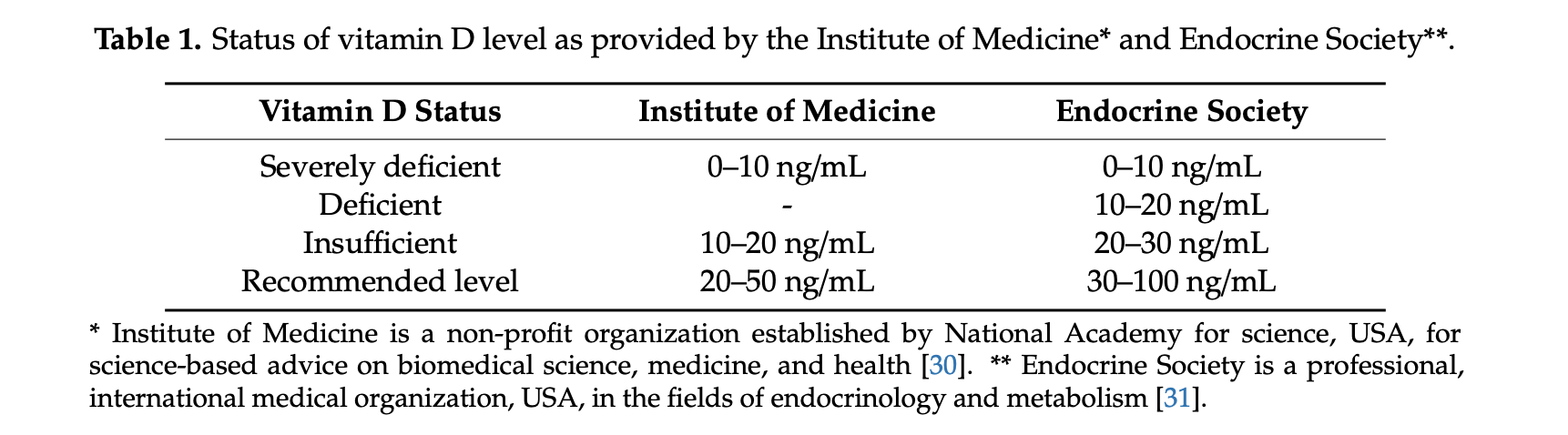
In our practice we aim to maintain a Vitamin D level of 0ver 60 in post weight loss surgical patients.
There are a number of theories as to how the Vitamin D deficiency may play a role in this. An emerging observation is that low Vitamin D may cause abnormal and excessive blood clot formation. Mohammad et. al. in 2019 published a study on the association of low vitamin D and “…Pathogenesis of Thrombosis”
This pathologic blood clot formation in COVID-19 patients may explain the extensive lung injury and multi system organ failure in some patient. It is also one of the reason that some COVID-19 patients have loss limbs or appendages.
Please follow all supplement recommendations based on your laboratory studies and all COVID-19 recommendations. We would recommend frequent hand washing, surface cleaning, social distancing, and wearing face masks as the most basic precautions and increase precautions based on your health status.
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
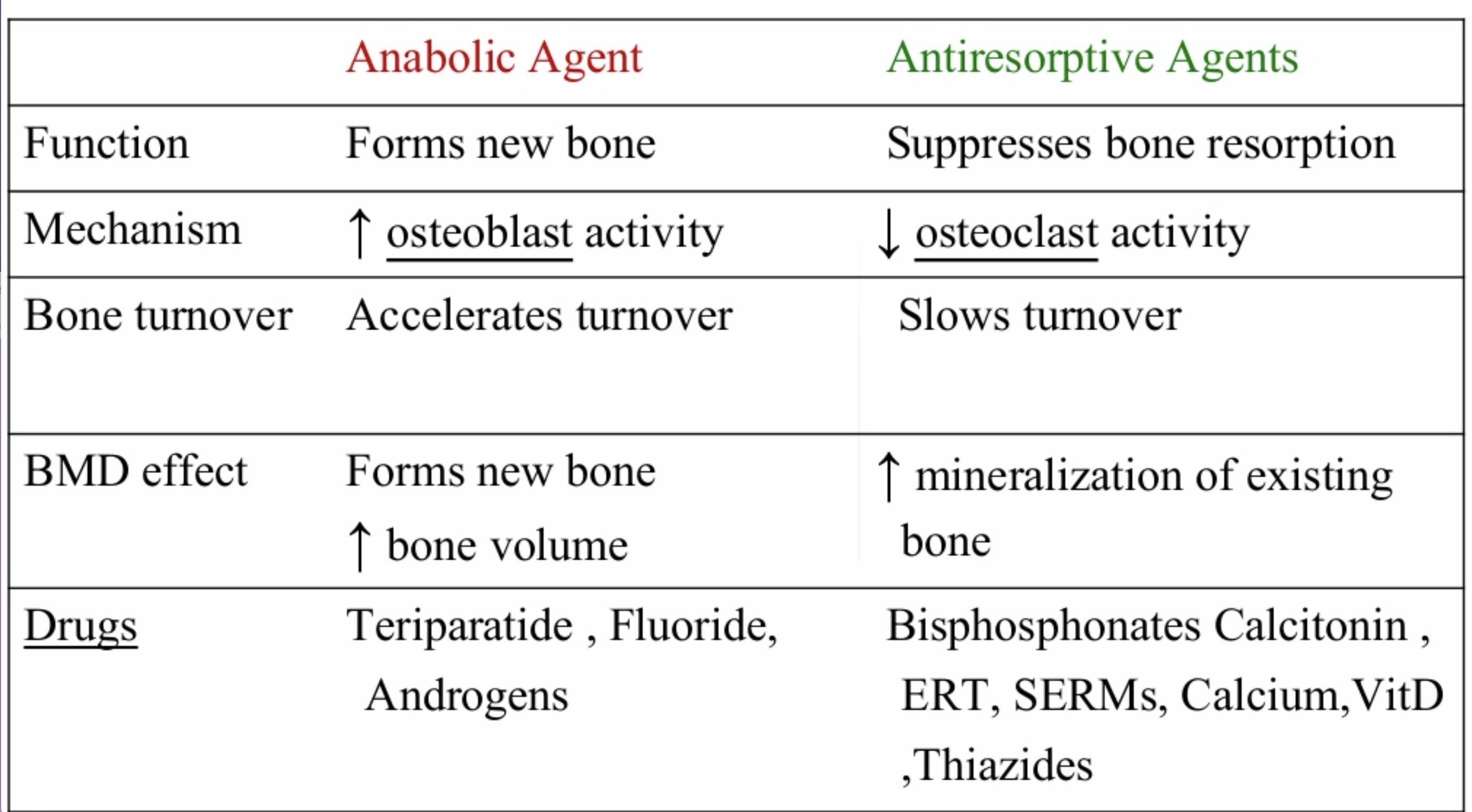
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
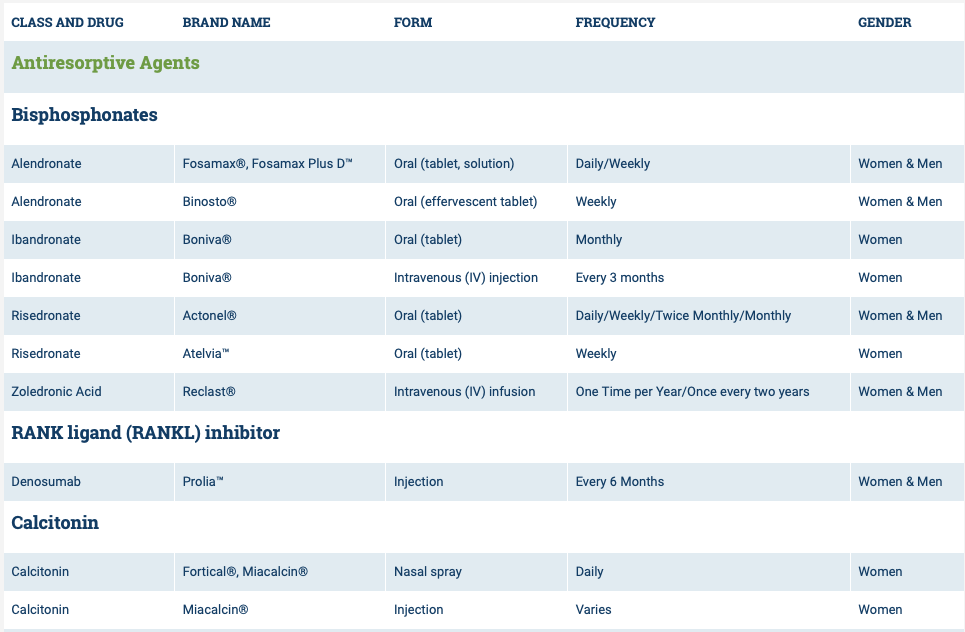
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

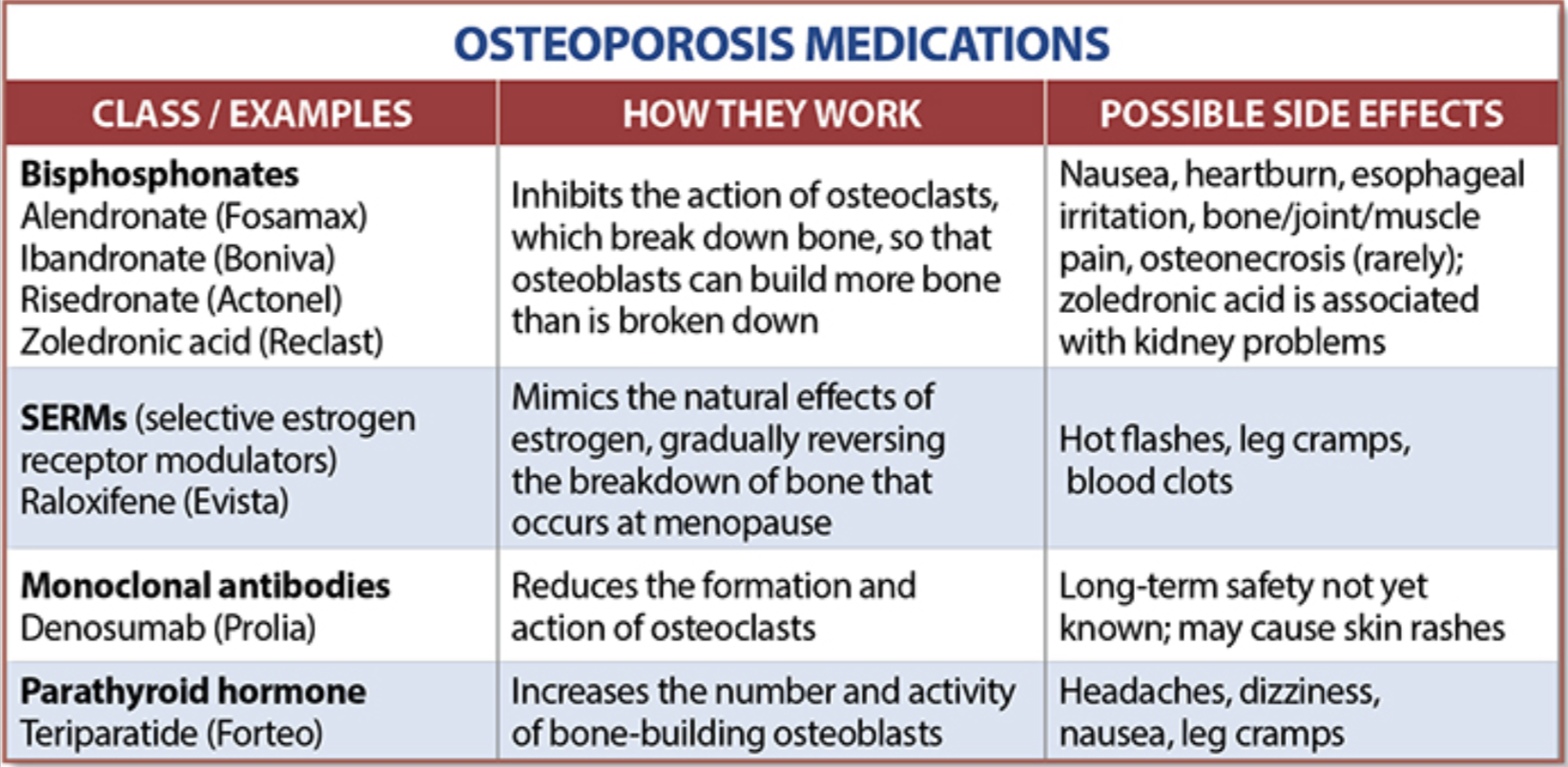
The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium
Magnesium Questions
May 11, 2016 6:07 am
Since our Webinar on Magnesium, I have received several Magnesium Questions recently regarding Magnesium deficiency. There is some evidence that calcium deficiency can not be corrected with an underlying magnesium deficiency. This may be due to the fact that magnesium is essential to converting Vitamin D to it’s active form and more information here. The active form of Vitamin D is needed to actively transport Calcium within the cell. This may be the confusion that calcium absorption needs magnesium. It is not needed directly but rather indirectly via Vitamin D.
Other cofactors needed in Vitamin D metabolism are:
Zinc (high doses antagonist with Magnesium and Copper)
Boron (raises Magnesium blood levels)
Vitamin K2
Vitamin A in small amounts
Further information regarding bone health and nutrients here.
Some important facts about Magnesium are:
- It is Absorbed in the distal Jejunum and Ileum (small intestines) and to some degree the colon.
- Plays an important role in Parathyroid Hormone synthesis which is also acted upon by Vitamin D
- Vitamin D increases Magnesium absorption
- All enzymes that metabolize Vitamin D require Magnesium
- Magnesium has a positive effect on Vitamin D deficiency.
- Magnesium and calcium are antagonist to each other on a cellular level (work against each other) They use an overlapping transport system for reabsorption within the kidneys and thereby compete with each other. Magnesium may also bind to calcium binding sites and intracellular protein binding sites due to their similarity.
- Calcium supplements can decrease Magnesium absorption.
- It Activates digestive enzymes for protein, fat and carbohydrate metabolism.
- Essential for protein synthesis
- Stores and moves energy acquired from digestion.
- Regulates Calcium via Vitamin D and increasing urinary excretion of calcium
Factors inhibiting Magnesium absorption:
- PPI
- Fiber
- Phytates
- Excessive unabsorbed fatty acids
- Calcium
- Phosphorus
- Protein

In summary, post Bariatric patients are at risk for magnesium deficiency and it plays an important role in overall health and bone health. Our practice recommends Magnesium Glycinate as the form for supplementation in at least a 2:1 ration with calcium. An example is: Calcium 2000mg daily to Magnesium Glycinate 1000mg daily. (Supplement based on your laboratory studies) We hope that this blog has answered some of your Magnesium Questions.
Pregnancy And Weight Loss Surgery
November 21, 2015 5:34 pm
This is not a substitution for formal medical advise that should be given to any patient by their bariatric surgeon and and OB/GYN familiar and experienced in the care of female patients with history of weight loss surgery. This is information that we provide our patients when we are notified of their pregnancy.
We recommend and instruct to take all precautions to avoid getting pregnant within the first 18 to 24 months following weight loss surgery. There is a significant amount of information about preferable birth controls, those to avoid, and additional pertinent information on our website.
Women who become pregnant after Weight Loss Surgery (WLS) should receive specific attention from their obstetrician because of the high risk nature of their pregnancy. Please make sure that you share this information with your OB/GYN. Many patients have become pregnant and delivered health babies after Duodenal switch (DS) without difficulty, but you do need to be watched more closely. The scientific study favor patients getting pregnant after DS when their weight loss , and nutritional markers have stabilized (18 months or longer) and not before. You also need to make sure you are taking all necessary vitamins, minerals and protein.
The first trimester is a very important time in the development of the fetus. Most organs and structures of the fetus are formed in the first trimester and therefore it is imperative that you pay close attention to your nutrition and your nutritional supplements.
You should continue to take your general multivitamins, other vitamins, minerals and your calcium as you were taking prior to getting pregnant. In addition, you should also take what will be prescribed by your OB/GYN. Do not substitute your prenatal vitamin and any other supplements that you are prescribed by your OB/GYN with what you were prescribed by our office. Each patient’s situation is individualized and additional changes or supplementations may be needed based on the advice of your surgeon and OB/GYN. Multiple fetus pregnancies require additional vitamin, mineral and protein needs.
A good prenatal vitamin should contain these:
Vitamin C – is essential for tissue repair, wound and bone healing and increases the body’s resistance to infection. For mother and baby this vitamin is essential daily as it is the agent that holds newly formed cells together. Helps baby to grow and builds strong bones and teeth. It is also instrumental in the body’s ability to absorb iron.
Vitamin D – promotes general growth. It maintains proper levels of calcium and phosphorus thus helping to build baby’s bones and teeth.
B Vitamins (thiamine, vitamin B6, riboflavin) – Thiamine converts carbohydrates into energy for mother and baby and is essential for baby’s brain development. It also aids in normal functioning of the nervous system and heart. If deficient during pregnancy, a baby is at risk for beriberi, a serious heart ailment. Vitamin B6 is also vital to develop your baby’s brain and nervous system. Riboflavin helps the body to produce energy. It promotes growth, good vision and healthy skin for mom and is important for the development of the baby’s bone, muscle and nervous system.
Folic Acid – is one of the B Vitamins that is needed to produce red blood cells. It helps synthesize DNA, is conducive to normal brain functions and is a critical part of spinal fluid, thus making it one of the few nutrients known to prevent neural tube defects such as spina bifida.
Calcium – your developing baby needs this mineral to grow strong bones and teeth, healthy nerves and muscles and to develop normal heart rhythm and blood clotting.
Potassium – is a mineral that helps maintain fluid balance in the body. This mineral helps regulate blood pressure, nerve impulses and muscle contractions.
Vitamin A – is important for cell growth, healthy skin and mucous membranes, and resistance to infections. It benefits red blood cell production in both mother and baby. This vitamin is essential for postpartum tissue repair.
Copper – a trace mineral found in all plant and animal tissues; it’s essential for forming red blood cells-a key process during pregnancy, when your blood supply doubles. Copper also aids tissue growth, glucose metabolism, and growth of healthy hair. It also helps form a baby’s heart, skeletal and nervous systems, arteries, and blood vessels.
Pantothenic Acid – is a trace mineral that regulates the body’s adrenal activity, antibody production, and the growth and metabolism of protein and fats. If you are deficient in this vitamin during pregnancy your baby’s growth may be slowed. This trace mineral is required for many essential functions, including growth, appetite regulation, digestion, wound healing, and the maintenance of collagen and elastin which may explain why some doctors think it may also help prevent stretch marks, one of the banes of pregnancy.
Iron – makes red blood cells, supplies oxygen to cells for energy and growth and builds bones and teeth. In pregnancy this mineral is so crucial because the body must produce extra blood to support the growing baby. During pregnancy you will need double the recommended daily allowance of iron to insure your health and that of your baby’s.
More often than not, many expectant mothers find taking a prenatal vitamin increases nausea in early pregnancy and sometimes beyond. If this happens, ask your doctor or midwife to change your formula or it may help to change how and when you take your vitamin. It is sometimes helpful to take your prenatal vitamins before you go to bed at night. If swallowing a large pill is difficult, cut it in half. In any event just like your mother said all those years, don’t forget to take your vitamin.
The following are important vitamin and nutritional components throughout the pregnancy but in particular the first trimester.
- Folic Acid: one of the B vitamins has been found to prevent neural tube defects (NTD). Increased intake of folic acid reduces the risk of NTDs such as anencephaly and spina bifida (open spine) by as much as 50 to 70% if women take enough before conception and in the early months of pregnancy. Take your general multivitamin and prenatal vitamin every day.
- Vitamin A: important to prevent blindness in the fetus. Vitamin A levels should be drawn and monitored prior to becoming pregnant and during the pregnancy to ensure adequate intake. You may need to take additional Vitamin A in a Dry water-soluble form such as Biotech Vitamin A 25. Please contact your surgeons office if your Vitamin A levels are below normal, or have not been drawn recently.
- Vitamin D: important for bone growth and formation. Vitamin D levels should be drawn prior to becoming pregnant and during the pregnancy to ensure adequate intake. Dry water-soluble form of Vitamin D3 such as Biotech D3 50. There is some research that adequate Vitamin D levels help protect against pre-term labor and an increase in preeclampsia risk.
- Protein: necessary in all structural formation of the fetus and the mother needs to increase protein intake by a minimum of 30 grams daily. Protein is need in nearly all fetal tissue formation.
The second and third trimesters are important in the growth, development and formation of bone structure and the overall growth of the fetus. It is important at this point to continue taking a minimum of 1500 mg Calcium (or what was prescribed by your surgeon), increased protein intake, your multivitamin, prenatal vitamin and any other supplements prescribed by your OB/GYN or surgeon. You may also need to increase your calorie intake with nutritious foods included in a healthy, well balance diet.
If you have any questions please contact your surgeon or the OBGYN. Your surgeon should also be willing to discuss any concerns that you or your OB/GYN may have with them.
Here is an discussion about the outcome of pregnancy after weight loss surgery.
In general we also advice against certain types of birth control because of the associated weight gain reported by the manufacturers. This is a decision that needs to be made after considering all potential side effects including the potential weight related issues. Ease of use should not be the only variable.
As indicated at the beginning of this blog, the information provided here is not a substitute for your nutritional evaluation by your bariatric surgeon or an experienced OB/GYN.
Bowel Length in Duodenal Switch
November 09, 2015 6:25 am
Malnutrition is one of the most feared complication of the duodenal switch operation. It may present years after surgery. What is common is a mix of nutritional deficiencies which include fat soluble vitamins, and protein calorie malnutrition. These all point to possible excessive shortening of the common channel. In my practice we have seen patients that have had lengthening of their common channel to improve their metabolic picture. What is very obvious to us, is that we see disproportionately higher number of cases coming to us for revision from practices where the common and alimentary lengths are done as a “standard” numbers with no specific adjustments made for the patient, their anatomy and situation. I have said for years, that the length of the bowel that is measured to be become the common and the alimentary limb should be a percentage of the total length of small bowel, rather than a pre-determined measurement. Here is a visual description of how this works.
If a common channel and the alimentary limb is measured to be a percent of the total length then the chance of protein calorie malnutrition is minimized since this will take into account the bowels absorptive capacity which is being reduced. This decrease in the absorption is done as a fraction of the total length.
Raines et al. published a study in 2014, that showed how small bowel length is related more closely to a patient’s height and not weight. And yet, some surgeons totally based the length of the common channel and the alimentary limb arbitrarily based on the patient pre operative BMI and nothing else. Could this be the cause of why I see some patients coming to us for revision of their duodenal switch for malnutrition?
Calcium – Revisited !Exclusive Member Content
October 05, 2015 8:06 am
Zinc InformationExclusive Member Content
April 17, 2015 7:22 am
Vitamin K1
April 08, 2015 7:16 pm
Vitamin K1 is a found in dark green leafy vegetables, asparagus, brussels sprouts, some grains, olive oil, prunes, soy bean oil, and canola oil. The body has limited storage capacity for Vitamin K and uses a recycle system to reuse it.
Vitamin K1 is a fat-soluble vitamin that after Duodenal Switch is not as easily absorbed due to the limiting contact of the food product with the bile until the common channel. Bile is needed to absorb fatty acids and fat-soluble vitamins.
Duodenal Switch patients in need of Vitamin K1 supplements should take “Dry” or water miscible type of Vitamin K1, such as Biotech brand. The patients laboratory studies will determine if a patient requires Vitamin K1 supplement. Duodenal Switch patients should have laboratory studies drawn and evaluated at least on a yearly basis. Vitamin K works in a delicate balance with other supplements and should be monitored by a physician, in at risk people.


Vitamin K1 is most know for it’s coagulation effect and the clotting cascade. Vitamin K1 works with calcium and proteins in order to accomplish coagulation synethesis. Care should be taken with Vitamin K supplementation and anti-coagulation (blood thinners) therapy. Please see your physician regarding any supplementation of Vitamin K and blood thinner medications.
A discovery of Vitamin K dependent proteins has led to research on Vitamin K1 in bone health. Bone matrix proteins, specifically osteocalcin, undergo gamma carboxylation with calcium much the way coagulation factors do; this process also requires Vitamin K. Osteocalcin is a Gla-protein that is regulated by Vitamin D. The calcium binding ability of osteocalcin requires several Vitamin K carboxylations to exert it’s effects on bone mineralization.

In adults, the causes of Vitamin K1 deficiency include the following :
Chronic illness
Malnutrition
Alcoholism
Multiple abdominal surgeries
Long-term parenteral nutrition
Malabsorption
Cholestatic disease
Parenchymal liver disease
Cystic fibrosis
Inflammatory bowel disease
Medications: Antibiotics (cephalosporin), cholestyramines, warfarin, salicylates, anticonvulsants, Cefamandole, cefoperazone, salicylates, hydantoins, rifampin, isoniazid, barbiturates, and certain sulfa drugs, higher Vitamin E can antagonized Vitamin K)
Massive transfusion
Disseminated intravascular coagulation (DIC) – Severe
Chronic kidney disease/hemodialysis
Additional information: https://lpi.oregonstate.edu/infocenter/vitamins/vitaminK/
Intake of Vitamin K1 and K2 and bone fracture risk
As always, discuss with your physicians and/or surgeon any changes in medications and supplements. This is not meant to be an all inclusive discussion of Vitamin K.