The difference between causation, coexistence, and correlation
Causation refers to a condition causing an effect.
Coincidence refers to two conditions present together at the same time, with neither causing the other.
Correlation refers to two conditions that may occur together, with no causation.
Study size refers to the research data on which the information is based. The larger the population size studied, the better the sample data and the more conclusive the results.
Confounding factors.
As I stated before, there is no clear evidence that cholecystectomy causes bile reflux gastritis. That does not mean that patients with bile reflux gastritis have not had a cholecystectomy.
Bile reflux is commonly seen after cholecystectomy, and yet only some develop bile reflux gastritis, why?
Those afflicted with this difficult condition are likely dealing with contributing factors as well, which should not be ignored and addressed.
Let’s discuss the publication:
The Prevalence of Bile Reflux Gastritis Following Cholecystectomy: A Meta-Analysis and Systematic Review.
If we read past the title and conclusion, all of the points 1-4 noted above are outlined, addressed, and discussed in the provided publication.
This study is very small and limited. The review article is based on 135 patients from hundreds of articles that they reviewed from multiple sources, between 2000 and 2004.
In the introduction, the authors clearly indicate that the “…loss of storage function…, loss of neuro hormonal responses causing motility changes in the upper GI may lead to duodenogastric reflux…” They further state that “The mechanism leading to bile reflux following cholecystectomy is not fully understood.” The authors state that cholecystectomy may increase the risk of bile reflux gastritis, but other factors, such as H. pylori, diabetes, motility dysfunction, hormonal changes, and the Sphincter of Oddi, may also be risk factors.
There is no causation, only correlation and coexistence. To be clear, bile reflux gastritis is common after cholecystectomy, but not clear whether it is caused by it.
This leads to a discussion of prevalence and incidence. The prevalence of bile reflux gastritis in a support group for the condition is extremely high, but the incidence in the general population is very small. The authors clearly state that the prevalence is nearly 50%.
Patients who develop bile reflux gastritis may have other contributing factors that should be evaluated. There is no clear evidence that cholecystectomy causes bile reflux gastritis, even though there is a higher incidence than in the general population. This distinction suggests that other risk factors may contribute to the onset of bile reflux gastritis, in addition to cholecystectomy.
There are 4 parathyroid glands which are located behind the thyroid gland, among other functions, are the main regulators of calcium, phosphorous, and magnesium in the blood. Elevations of parathyroid hormone (hyperparathyroidism) can be: 1-Primary, 2-Secondary, 3-Tertiary
Primary hyperparathyroidism means the parathyroid glands themselves are hyperactive. This may involve only one of the four glands: a) an adenoma, a benign tumor that needs surgical removal, or b) hyperplasia, when all 4 glands are hyperactive and/or enlarged, and in some cases, most of the 4 glands need to be removed.
Secondary hyperparathyroidism means that the elevated PTH level is caused by an external regulatory stimulus, such as low calcium, which itself may be due to low vitamin D, low calcium intake, or other causes.
Tertiary hyperparathyroidism is seen only in specific renal failure and transplant patients.
Regardless of the type of hyperparathyroidism, the end result is the same. Because the parathyroid gland aims to maintain normal calcium levels, it will do everything to achieve them. This includes increasing calcium absorption from the GI tract, breaking down bone to increase the blood calcium supply, and increasing calcium reabsorption from the urine.
Distinguishing between primary and secondary is critical, as primary is more likely than not a surgical problem that needs to be addressed. Secondly, it may be responding to metabolic deficiencies (low CA, low Vitamin D) that need to be corrected and take some time.
Not all cases require surgical intervention, as labs (vitamin D, calcium, and alkaline phosphatase) and imaging studies, such as neck ultrasound, CT scan, and Sestamibi scan, provide the information needed to dictate the treatment plan. Please stay up to date with your yearly lab results to catch changes sooner rather than later.
Iron is critical for the production and action of red blood cells. Deficiency of iron may have many causes. These include bleeding from the GI track, inadequate absorption, inadequate intake, and menstrual losses in females.
It’s important to have at least yearly laboratory studies to surveil for abnormalities. Normal results of iron testing may be different for men, women, and children. Iron and TIBC are measured in micrograms per deciliter (mcg/dL). Normal results for iron are:
65 to 175 mcg/dL for men
50 to 170 mcg/dL for women
50 to 120 mcg/dL for children
Normal results for TIBC are 250 to 450 mcg/dL for men and women.
To correct or prevent IDA, iron supplementation is recommend in some patients. Iron absorption is very inefficient. It take a long time to develop IDA and as long if not longer to correct it with oral supplementation. This is why we recommend some patient condor getting iron infusion.
For most, oral supplements are adequate. There are different formulary of iron supplement with varying degree of absorption.
Heme iron and iron bisglycinate have been shown to have much better absorption than ferrous sulfate formulary.
Endoscopic sleeve gastroplasty (ESG) differs from Laparoscopic sleeve gastrectomy (LSG).
ESG (Endoscopic Sleeve Gastroplasty) is promoted and advocated as a low-risk, equal alternative to the Laparoscopic Sleeve Gastrectomy, but it is not.
Anatomically speaking:
Endoscopic Sleeve Gastroplasty is an endoscopic procedure performed under general anesthesia. During this procedure, a specialized endoscope is inserted through the mouth into the stomach. Multiple plastic “H”-type anchors are used to create a fold in the stomach, thereby reducing its size. No part of the stomach is removed. Initial limited weight loss occurs as the patient feels full after consuming small volumes of food. This effect resembles what happens with the lap band and gastric balloon, and we know how the story ends with those.
LSG is performed laparoscopically with incisions on the abdomen under general anesthesia. Seventy-five to eighty-five percent of the stomach, along its greater curvature, is removed, eliminating the part of the stomach that produces the Ghrelin hormone, which controls and modulates hunger. This is why patients feel fuller with a smaller volume of food and experience significantly reduced hunger.
Results:
Please read the fine print
The summary results indicate
“Our results suggest that ESG is safe and effective for the treatment of obesity, with durable
long-term results for at least up to 5 years after the procedure. “
When you look at the details of the results, however, it states:
“At 5 years, mean TBWL was 15.9% (95% CI, 11.7-20.5, p < .001) and 90 and 61% of
patients maintained 5 and 10% TBWL, respectively.”
This means that five years after ESG, 90% of the patients have only lost 10% of their TBWL (total body weight loss), and 61% would have lost 10% of their TBW (Total Body Weight).
This serves as an illustration of how actual outcomes are obscured within the fine print, resulting in a lack of attention from individuals seeking the optimal outcome devoid of perceived risk. The same principle applies to the ongoing discourse regarding GLP-1 medications. The genuine risk associated with ESG and PLG-1 is that patients have undergone alterations to their anatomy and physiology without demonstrable results. Several years into contemplating a treatment promising sustained outcomes, we find that the alterations have increased the overall risk.
As a surgeon, I encourage people to always ask questions and demand that scientific proof be provided. I am not opposed to progress; considering the nature of our practice, we have witnessed and have unrgone significant evolution over the past 30 years, transitioning from performing open cases necessitating a hospitalization period of 4 to 6 days to performing the same cases laparoscopically and robotically in some cases outpatient procedures.
I have frequently been asking what staples are used in sleeve gastrectomy. A stapling device is used with sleeve gastrectomy. This device comes in different shapes and sizes for different bowel thicknesses and applications. However, they all function the same way. The staple cartridges (the part of the stapler that is replaced after each use with a new one) are selected based on the thickness of the segment of the bowel that needs to be stapled and divided.
The stapling and dividing take place simultaneously. The sampler deploys six rows of staples and cuts between them, leaving three rows on one side and three on the opposite side. With the sleeve gastrectomy, this means that the sleeve stomach that is left has three rows of staples, and the segment of the stomach that is removed also has three rows of staples.
Questions that are frequently asked:
1-Can I have a CT or an MRI done? Yes, The titanium staples are safe for both CT and MRI.
2-What are they made from? The staples are made of titanium and alloys, which are non-reactive and safe.
3-How big are the staples? Different staples are of different sizes, mainly in the mm range; see the tip of the pencil in the image for the relative size.
Patients are frequently asked to explain why they take high fat- or water-soluble vitamin doses. They are have often been scared by their well meaning healthcare providers that their higher levels of vitamin supplements will end up with vitamin toxicity.
Let’s clarify one point: there is such a thing as too much vitamin.
However, the point that is often overlooked in teaching within professional schools (medical, nursing, pharmacy, etc.) and drug manufacturers is that recommendations are based on “how much to take” and not how much is needed to keep a patient’s blood level in the normal range.
This table highlights how toxicity is described and what requirements are recommended. Vitamin toxicity is seen rarely in post-weight loss surgical patients who take them proactively in as many doses as needed to get their blood levels in the normal range. I see more patients in the office who suffer from low vitamin levels, such as vitamin D and A levels (duodenal switch and sleeve), than any patient with high or toxic levels of any vitamins.
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wegovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity
Radiology film of normal position and a slipped LapBand
SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
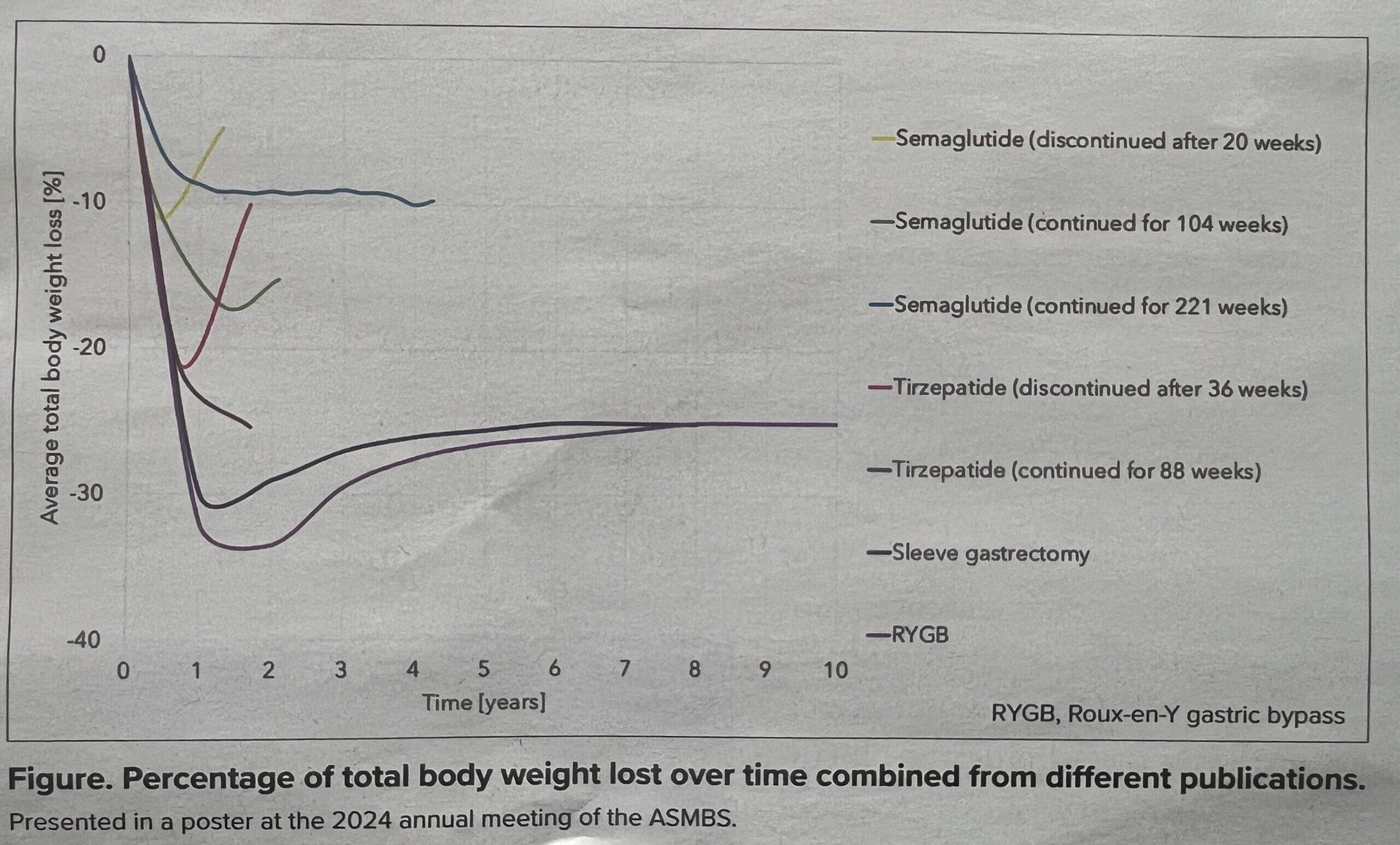
Similar to many previous attempts, the simple and cheap route does not necessarily produce sustained desirable results. This recent article below summarizes a presentation made at the 2024 Annual Meeting for ASMBS. I may not agree with some of the researcher’s conclusions, but the data presented supports what we have said all along: that the GLP-1 class of medication does not produce durable and adequate weight loss.
SAN DIEGO-Bariatric surgery far outperforms lifestyle interventions and glucagon-like peptide-1 (GLP-1) medications at maintaining weight loss, according to a meta-analysis presented at the 2024 annual meeting of the American Society for Metabolic and Bariatric Surgery.
With results from six randomized controlled trials, three systematic reviews, and more than 40,000 patients, the study is the first synthesis of its kind.
“The analysis included two systematic reviews of bariatric surgery, one of Roux-en-Y gastric bypass including8,665 patients and one of sleeve gastrectomy including 6,095 patients: a single systematic review or lifestyle interventions including 723 patients; and six randomized controlled trials of GLP-1 medications, including four studies of semaglutide with a total of 11,871 patients and two of tirzepatide with 3,209 patients.
Lifestyle interventions were the least effective treatment, the investigators found, producing a mean total body weight loss of 7.4% at the end of the treatment period, followed by a mean per-month weight regain of 0.14%, with participants reaching their pre-intervention weights within 4.1 years.
GLP-1 medications proved more effective. Weekly semaglutide injections for 20 weeks and tirzepatide for 36 weeks produced a mean total body weight loss of 10.6% and 21.1%, respectively. Roughly half of the weight lost was regained within a year after stopping injections; with continued injections, weight loss plateaued after 17 to 18 months, at 14.9% for semaglutide and 22.5% for tirzepatide.
Outcomes after surgery were significantly better. Gastric bypass surgery and sleeve gastrectomy resulted in a mean total body weight loss of 31.9% and 29.5%, respectively, one year after surgery. Accounting for weight regained in the decade after surgery, both procedures produced a stable total body weight loss of approximately 25%.
While the results demonstrate a striking difference favoring surgery, lead investigator Megan Jenkins, MD, a bariatric surgeon at NYU Langone Medical Center in New York City, emphasized that surgery and medication ought to be viewed not in opposition but through a holistic lens as options and potential complements based on the needs of each patient.
“One of the big benefits of these new medications is that it’s helped us to treat obesity as a chronic disease,” Dr. Jenkins said. “We’ve always treated it that way, but I think the medical field has had trouble truly seeing it as a chronic disease. Like diabetes and high blood pressure, for example, which have always been treated with a combination approach.
The benefits of weight loss surgical procedures are undisputed. Over the last decades, as the incidence of obesity has increased, so has the need for effective long-term treatment options. It is no secret that diet and exercise plans are only short-term remedies since none of them provide realistic long-term alternatives. Let’s be clear that a healthy diet and activity level are critical to a healthy body and mind and to the long-term success of weight loss surgery.
A frequent question: How young is too soon for weight loss surgery? We work with our patients to ensure that weight loss surgery will not affect the growth of an adolescent patient with regard to height, bone formation, and hormonal status. Specifically, there are concerns about a female patient’s ability to get pregnant and have children. All the scientific evidence points to the benefits of weight loss surgery and the improved ability to get pregnant and bear the pregnancy to completion. Weight loss positively impacts the ability to get and have a healthy pregnancy leading to a non obese child.
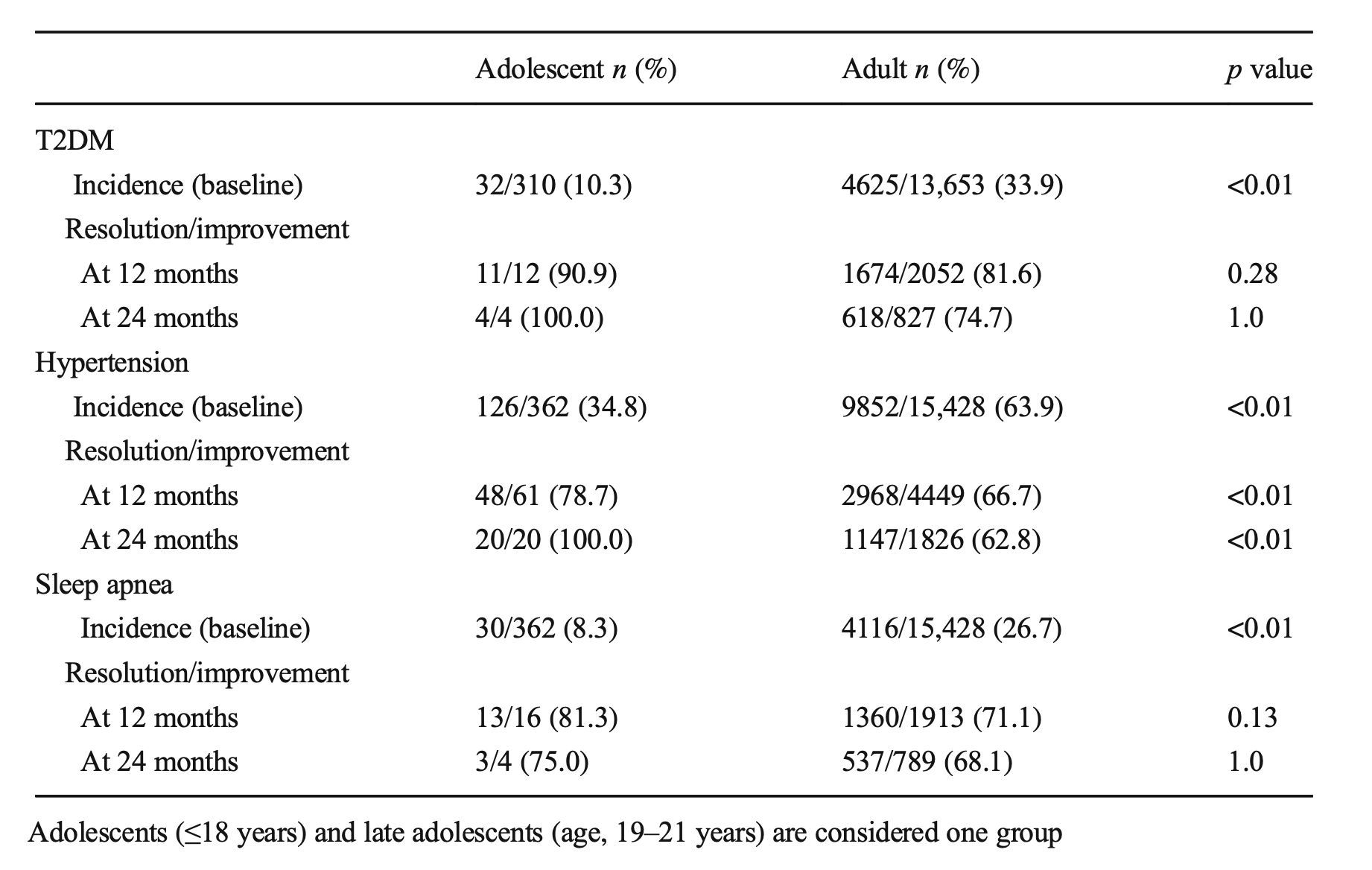
An article recently published demonstrated the benefits of early intervention. Specifically, it showed the improved odds of resolution of diabetes in the younger patients (100% in adolescents, Vs. 75% in adults ) at 24 months post-op.
Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
These meetings are for general topics and/or basic question and answers. If you need a more in-depth meeting we would suggest a video or in-person consultation with Dr. Keshishian. You can request a consultation via this link. Contact Us