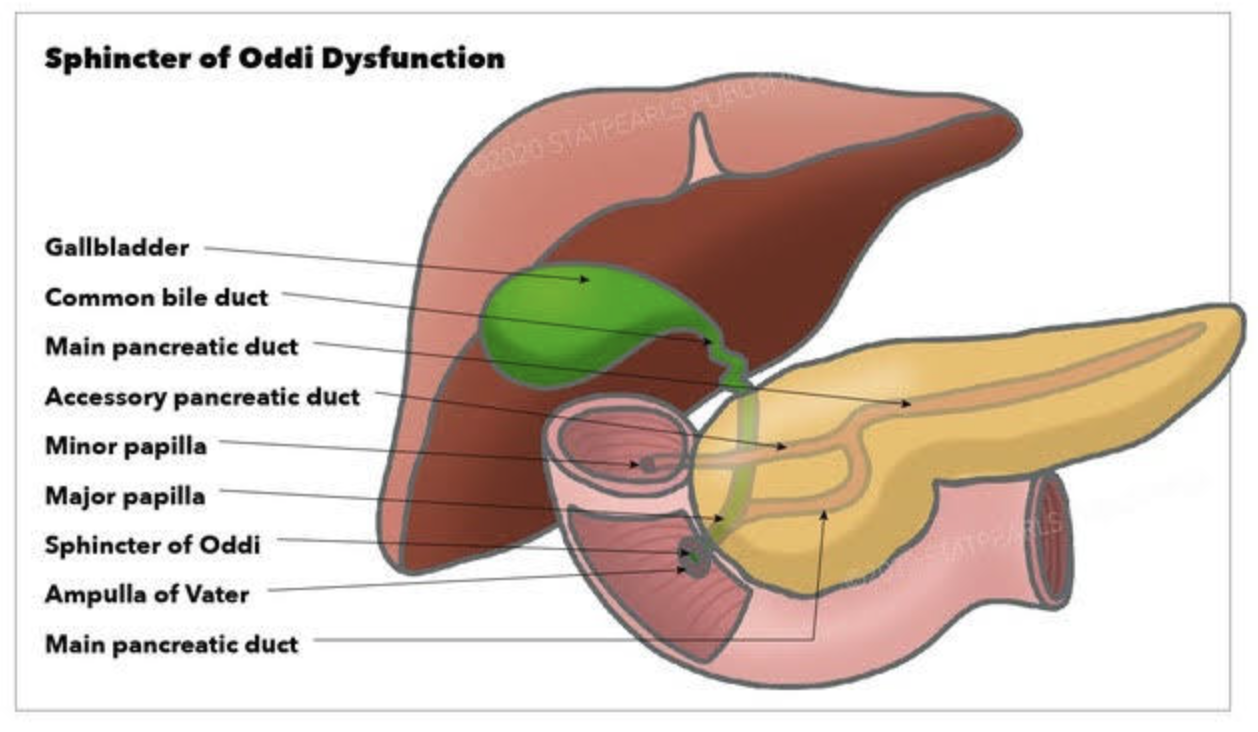
Sphincter of Oddi Dysfunction (SOD) is a clinical syndrome characterized by biliary/ pancreatic pain from abnormal function or obstruction of the.
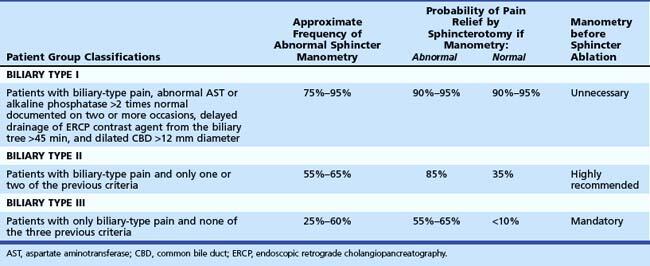
It is commonly considered after cholecystectomy when ongoing biliary-type pain or pancreatitis is present. SOD is classified into three Milwaukee/Rome types based on clinical, laboratory, and imaging criteria. Type I shows objective ductal dilation and enzyme abnormalities, type II has biliary pain with either dilation or enzyme elevation, and type III has biliary-type pain without objective abnormalities.
Diagnostic and classification
The SOD spectrum includes biliary, pancreatic, or combined sphincter dysfunction, with symptoms driven by dyskinesia or mechanical obstruction. The term SOD encompasses both functional motility disorders (biliary or pancreatic sphincter dysfunction) and mechanical obstructions such as papillary stenosis.
SOM has been considered the gold standard for diagnosing elevated basal sphincter pressure. It is invasive and carries complications, including pancreatitis. SOM can also not be done in those who have had gastric bypass or duodenal switch operations. Sphincterotomy outcome is not uniform. Consequently, many centers have moved toward empiric endoscopic therapy for appropriately selected patients and toward noninvasive or less invasive diagnostic approaches for others.
Treatment approaches
Endoscopic biliary sphincterotomy (EST) is the most established nonpharmacologic treatment for biliary SOD, particularly in type I and many type II patients with objective ductal dilation and/or enzyme elevation.
In type II SOD, outcomes after EST correlate with objective evidence of obstruction or sphincter hypertension on SOM. Empiric sphincterotomy without manometry is controversial.
Type III SOD has emerged as predominantly functional pain rather than a mechanical obstacle. Alternative management emphasizes risk stratification, noninvasive strategies, and multidisciplinary approaches.
Medical and non-sphincterotomy options (calcium-channel blockers, nitrates, antidepressants, and lifestyle modifications) have been discussed as potential adjuncts or alternatives.
Summary
SOD is a multifactorial biliary and pancreatic sphincter disorder with a spectrum from mechanical obstruction to pure dyskinesia. Type I and II retain treatment relevance, particularly EST for biliary obstruction. Type II management requires clear identification of the cause.
SOM is a diagnostic tool with significant limitations.
Endoscopic sphincterotomy offers meaningful symptom relief in type I and select type II with objective obstruction. It carries a risk of complications, including pancreatitis; risk mitigation strategies are integral to practice. In type III SOD, sphincterotomy generally has limited benefit, necessitating a move toward noninvasive management and careful patient counseling. Patients post- gastric bypass, or duodenal switch, can not have ERCP or SOM done.
Endoscopic sleeve gastroplasty (ESG) differs from Laparoscopic sleeve gastrectomy (LSG).
ESG (Endoscopic Sleeve Gastroplasty) is promoted and advocated as a low-risk, equal alternative to the Laparoscopic Sleeve Gastrectomy, but it is not.
Anatomically speaking:
Endoscopic Sleeve Gastroplasty is an endoscopic procedure performed under general anesthesia. During this procedure, a specialized endoscope is inserted through the mouth into the stomach. Multiple plastic “H”-type anchors are used to create a fold in the stomach, thereby reducing its size. No part of the stomach is removed. Initial limited weight loss occurs as the patient feels full after consuming small volumes of food. This effect resembles what happens with the lap band and gastric balloon, and we know how the story ends with those.
LSG is performed laparoscopically with incisions on the abdomen under general anesthesia. Seventy-five to eighty-five percent of the stomach, along its greater curvature, is removed, eliminating the part of the stomach that produces the Ghrelin hormone, which controls and modulates hunger. This is why patients feel fuller with a smaller volume of food and experience significantly reduced hunger.
Results:
Please read the fine print
The summary results indicate
“Our results suggest that ESG is safe and effective for the treatment of obesity, with durable
long-term results for at least up to 5 years after the procedure. “
When you look at the details of the results, however, it states:
“At 5 years, mean TBWL was 15.9% (95% CI, 11.7-20.5, p < .001) and 90 and 61% of
patients maintained 5 and 10% TBWL, respectively.”
This means that five years after ESG, 90% of the patients have only lost 10% of their TBWL (total body weight loss), and 61% would have lost 10% of their TBW (Total Body Weight).
This serves as an illustration of how actual outcomes are obscured within the fine print, resulting in a lack of attention from individuals seeking the optimal outcome devoid of perceived risk. The same principle applies to the ongoing discourse regarding GLP-1 medications. The genuine risk associated with ESG and PLG-1 is that patients have undergone alterations to their anatomy and physiology without demonstrable results. Several years into contemplating a treatment promising sustained outcomes, we find that the alterations have increased the overall risk.
As a surgeon, I encourage people to always ask questions and demand that scientific proof be provided. I am not opposed to progress; considering the nature of our practice, we have witnessed and have unrgone significant evolution over the past 30 years, transitioning from performing open cases necessitating a hospitalization period of 4 to 6 days to performing the same cases laparoscopically and robotically in some cases outpatient procedures.
The gastrointestinal staplers simultaneously pass six rows of staples and cut in between them to create two secure lines of staples, three rows on each side. The staples come in different thicknesses and lengths for various applications. Staple cartridges that are used for colon surgery are usually thicker tissue staples than those that are used for small bowel stapling.
Different manufacturers have different color coding.
Another question I frequently get asked is, How does a stapler staple and cut at the same time? The stapler needs to be thick enough to not tear through the tissue and provide uniform pressure for control of bleeding and prevent leaks. It can not be too large either.
When stapling on the stomach for sleeve gastrectomy, the stomach wall thickness is different. We use different-sized staples to accommodate the thicker part of the lower stomach toward the thinner part of the stomach where it meets the esophagus.
Stapler and resulting discharged lines of staples.
I have frequently been asking what staples are used in sleeve gastrectomy. A stapling device is used with sleeve gastrectomy. This device comes in different shapes and sizes for different bowel thicknesses and applications. However, they all function the same way. The staple cartridges (the part of the stapler that is replaced after each use with a new one) are selected based on the thickness of the segment of the bowel that needs to be stapled and divided.
The stapling and dividing take place simultaneously. The sampler deploys six rows of staples and cuts between them, leaving three rows on one side and three on the opposite side. With the sleeve gastrectomy, this means that the sleeve stomach that is left has three rows of staples, and the segment of the stomach that is removed also has three rows of staples.
Questions that are frequently asked:
1-Can I have a CT or an MRI done? Yes, The titanium staples are safe for both CT and MRI.
2-What are they made from? The staples are made of titanium and alloys, which are non-reactive and safe.
3-How big are the staples? Different staples are of different sizes, mainly in the mm range; see the tip of the pencil in the image for the relative size.
The surgical changes following the revision of the failed gastric bypass to the duodenal switch or a primary duodenal switch require an evident appreciation and understanding of the anatomy and physiology of placing a feeding tube and managing the nutritional status. There are different places where a feeding tube can be placed.
1-A feeding gastrostomy tube endoscopically cannot be placed because of the transected post-pyloric duodenum (The image viewed on a desktop or a laptop allows the scroller on the image to move)
2-An orogastric or nasogastric tube should only use an elemental feeding formula. This is because the food in the stomach is prevented from mixing with the biliopancreatic juices, which will not be adequately absorbed.
3-A feeding Jejunostomy can only be insured surgical post ligament of traits. This cannot be done endoscopically because duodenal switch transaction post pyloric small bowel to prevent mixing of the biliopancreatic secretion.
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wegovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity
Radiology film of normal position and a slipped LapBand
SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
Hello
Weight loss surgical results are dependent on several variables. These include patient-specific conditions as well as the type of surgery. The primary objective of this study is to evaluate if there is any value in the specific pre-operative workup mandated by health insurance plans and the long-term outcome of the weight loss surgical procedures. The secondary result of the study is to compare the surgical outcomes of the different weight loss procedures.
We hope you can spare a few minutes to complete the survey if you have received it. If you have not seen the study, please check your spam junk folder for an email that contains the link from our office.
We wish you a happy and healthy holiday season.
Date-entry instruction Video
As the COVID-19 pandemic is charting its course into 2022, as health care providers, we have had to adapt and adjust to the transient and shifting environment. Testing for COVID-19 has been in place, and is now part of the standard for preoperative work-up. In addition, covid testing will likely be part of screening any surgical procedure for the foreseeable future.
The challenge of pandemic control is the large pockets of populations in the US and worldwide that do not have protection against the virus and are not vaccinated. Vaccination provides the only proven long-term protection against COVID-19 infection and its long-term persistent health effect. In addition, the complication rate reported in scientific journals is negligible compared to the complication and death rate from the COVID-19 infection.
There are implications of covid infection and general anesthesia published in peer-reviewed journals. The increased risk of general anesthesia after covid infection is related to the severity of the initial infection and the extent of the treatment required, and the persistence of the post covid symptoms, including shortness of breath, fatigue, and laboratory finding elevated inflammatory markers. Long after resolution of the acute COVID-19 symptoms, the most common persistent complaints are fatigue, shortness of breath, Joint and chest pain; and all these increase the risk of post-operative complications (Carfì et al., 2020)
The required delay for surgery may be as short as 2-4 weeks to as long as six months or longer if the persistent symptoms are present. Surgery may not be avoidable in a critical life-threatening situation and may be necessary even with a much-increased risk of complication (Collaborative, 2020). Recovery post-COVID-19 may not be complete with the resolution of the initial symptoms (Dexter et al., 2020)
Recent publications and scientific presentations have also shown the protection that weight loss surgery and maintained weight loss provide in those who come down with the COVID-19 infection (Aminian et al., 2021). However, the rate of weight gain, lack of weight loss is worse for weight loss surgical patients post COVID-19 disorder (Bullard et al., 2021; Conceição et al., 2021). Furthermore, patients with COVID-19 infection post weight loss are at a higher risk of malnutrition (di Filippo et al., 2021; Kikutani et al., 2021). Up to 40% of patients have malnutrition if hospitalized with COVID (Anker et al., 2021).
To summarize, Weight loss and weight loss surgery reduce the severity of the initial COVID-19 infection. However, it increases malnutrition risk, requiring nutritional support and surgical interventions in non-responsive cases.
REFERENCES:
Aminian, A., Fathalizadeh, A., Tu, C., Butsch, W. S., Pantalone, K. M., Griebeler, M. L., Kashyap, S. R., Rosenthal, R. J., Burguera, B., & Nissen, S. E. (2021). Association of prior metabolic and bariatric surgery with severity of coronavirus disease 2019 (COVID-19) in patients with obesity. Surgery for Obesity and Related Diseases, 17(1). https://doi.org/10.1016/j.soard.2020.10.026
Bullard, T., Medcalf, A., Rethorst, C., & Foster, G. D. (2021). Impact of the COVID-19 pandemic on initial weight loss in a digital weight management program: A natural experiment. Obesity, 29(9). https://doi.org/10.1002/oby.23233
Conceição, E., de Lourdes, M., Ramalho, S., Félix, S., Pinto-Bastos, A., & Vaz, A. R. (2021). Eating behaviors and weight outcomes in bariatric surgery patients amidst COVID-19. Surgery for Obesity and Related Diseases, 17(6).
Di Filippo, L., De Lorenzo, R., D’Amico, M., Sofia, V., Roveri, L., Mele, R., Saibene, A., Rovere-Querini, P., & Conte, C. (2021). COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clinical Nutrition, 40(4). https://doi.org/10.1016/j.clnu.2020.10.043
Kikutani, T., Ichikawa, Y., Kitazume, E., Mizukoshi, A., Tohara, T., Takahashi, N., Tamura, F., Matsutani, M., Onishi, J., & Makino, E. (2021). COVID-19 infection-related weight loss decreases eating/swallowing function in schizophrenic patients. Nutrients, 13(4). https://doi.org/10.3390/nu13041113
The benefits of weight loss surgical procedures are undisputed. Over the last decades, as the incidence of obesity has increased, so has the need for effective long-term treatment options. It is no secret that diet and exercise plans are only short-term remedies since none of them provide realistic long-term alternatives. Let’s be clear that a healthy diet and activity level are critical to a healthy body and mind and to the long-term success of weight loss surgery.
A frequent question: How young is too soon for weight loss surgery? We work with our patients to ensure that weight loss surgery will not affect the growth of an adolescent patient with regard to height, bone formation, and hormonal status. Specifically, there are concerns about a female patient’s ability to get pregnant and have children. All the scientific evidence points to the benefits of weight loss surgery and the improved ability to get pregnant and bear the pregnancy to completion. Weight loss positively impacts the ability to get and have a healthy pregnancy leading to a non obese child.
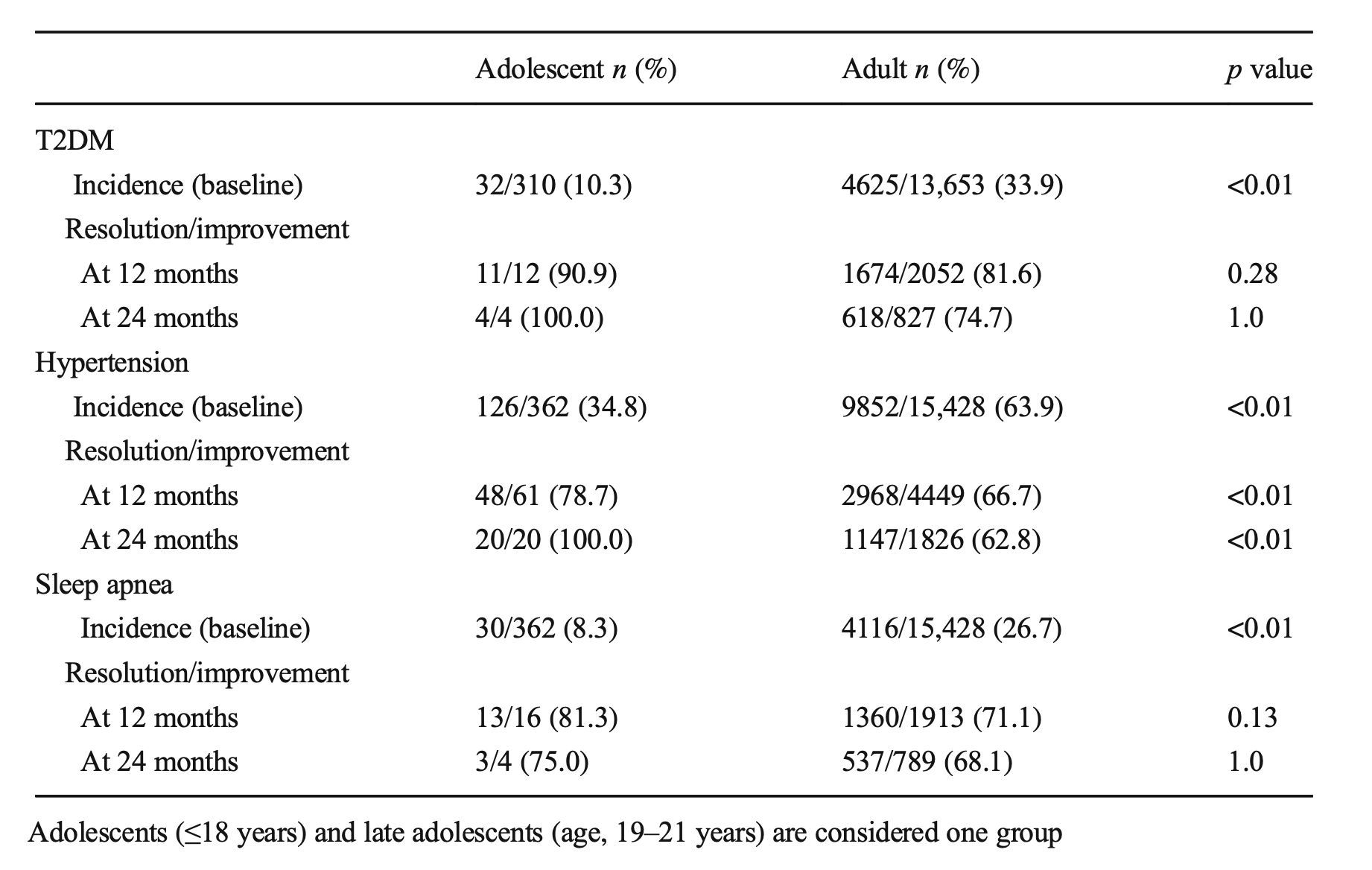
An article recently published demonstrated the benefits of early intervention. Specifically, it showed the improved odds of resolution of diabetes in the younger patients (100% in adolescents, Vs. 75% in adults ) at 24 months post-op.
Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
These meetings are for general topics and/or basic question and answers. If you need a more in-depth meeting we would suggest a video or in-person consultation with Dr. Keshishian. You can request a consultation via this link. Contact Us