Category: nutritional deficiencies
Feeding Tube with Duodenal Switch
February 03, 2025 9:53 am
The surgical changes following the revision of the failed gastric bypass to the duodenal switch or a primary duodenal switch require an evident appreciation and understanding of the anatomy and physiology of placing a feeding tube and managing the nutritional status. There are different places where a feeding tube can be placed.
1-A feeding gastrostomy tube endoscopically cannot be placed because of the transected post-pyloric duodenum (The image viewed on a desktop or a laptop allows the scroller on the image to move)
2-An orogastric or nasogastric tube should only use an elemental feeding formula. This is because the food in the stomach is prevented from mixing with the biliopancreatic juices, which will not be adequately absorbed.
3-A feeding Jejunostomy can only be insured surgical post ligament of traits. This cannot be done endoscopically because duodenal switch transaction post pyloric small bowel to prevent mixing of the biliopancreatic secretion.
Additional informationSurvey
December 16, 2023 9:54 am
Vitamin A and Wound healing
December 21, 2020 9:37 am
Night Blindness – Vitamin A Deficiency
Nyctalopia (Night Blindness) An Early Sign of Vitamin A Deficiency with VideoA recent article discusses the types and function of vitamin A. As with the pandemic of COVID-19 continuous to stress our body and mind, we must stay vigilant with our nutritional status. Therefore, Vitamin supplements are critical in maintaining a robust immune system. For some, oral supplements are adequate; others may require injectable forms. If the oral supplements do not correct the vitamin A levels, please contact your primary care or our office to available vitamin A injections.
Overfed But Undernourished
October 01, 2019 11:27 am
Obesity is related to as many as 400,000 deaths each year in the US and it has increasingly been recognized as a risk factor for several nutrient deficiencies. This may seem surprising given the likelihood of over consumption of calories, however these additional calories are not from nutritious sources. One of the main reason for these nutritional deficits is the greater availability of inexpensive foods that are rich in calories and are nutrient deficient. This has led some medical professional to conclude that there is a certain group of people who are overfed but undernourished. Even with the epidemic of the obesity, there is significant nutritional deficiencies noted.
Obese subjects have increased blood volume, cardiac output, adiposity, lean mass and organ size all of which can influence volume of distribution, in addition, treatment for severe obesity involving surgical procedures can worsen these nutrient deficiencies and in some cases may cause new ones to develop.
This table shows the percentage of population below the estimated average requirement (EAR) by body weight status in adults more tan 19 years old, showing that almost 90 to 100 percent of people including normal weight (NW) are below the EAR of vitamin D and Vitamin E.

We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
Vitamin A, Absorption, and Wound Healing
September 25, 2019 8:39 am
Vitamin A is one of the 4 fat soluble vitamins along with vitamin D, Vitamin E and Vitamin K. It is multifunctional and essential which means that it is not produced by the body. In this article we will touch on aspects of Vitamin A absorption and it’s effect on wound healing as well as its metabolism.
We often think of Vitamin A as the critical vitamin for vision, however it has several other roles that related to immune function, protein synthesis, and cellular communication. Vitamin A deficiency is a concern world wide because of the natural of the side effects. Vitamin A deficiency is the leading cause of preventable childhood blindness in the world according to UNICEF and sometimes it may be undetected until there is irreversible damage.
There are 2 chemical forms of vitamin A in diet:
Retinoids (Preformed vitamin A) This group include retinol, retinyl esters, and retinal they are mostly found in animal sources like liver, egg yolk or fish oils.
Carotenoids (Provitamin A) This group includes beta-carotene, alpha-carotene and lycopene, mainly found in plant sources like leafy vegetables or yellow/orange vegetables and fruits.
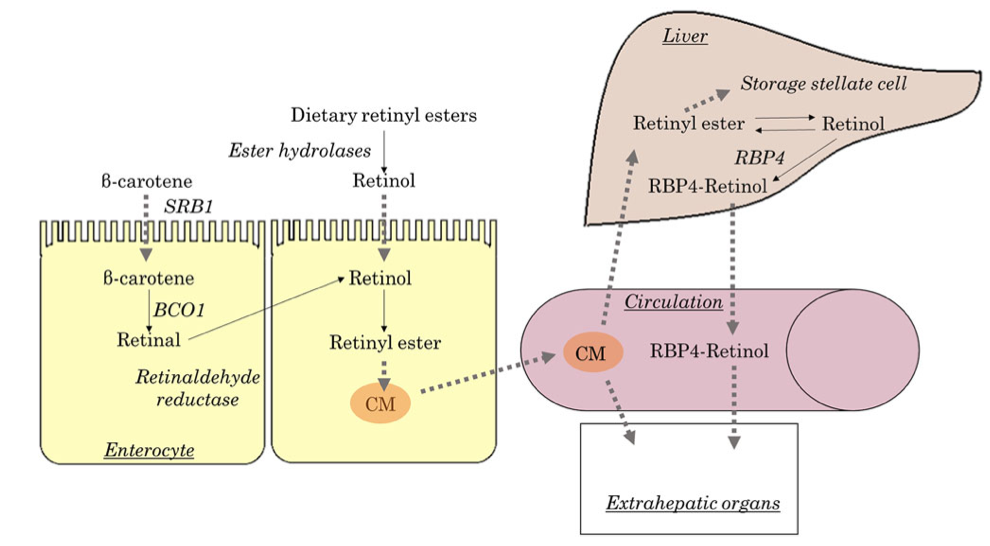
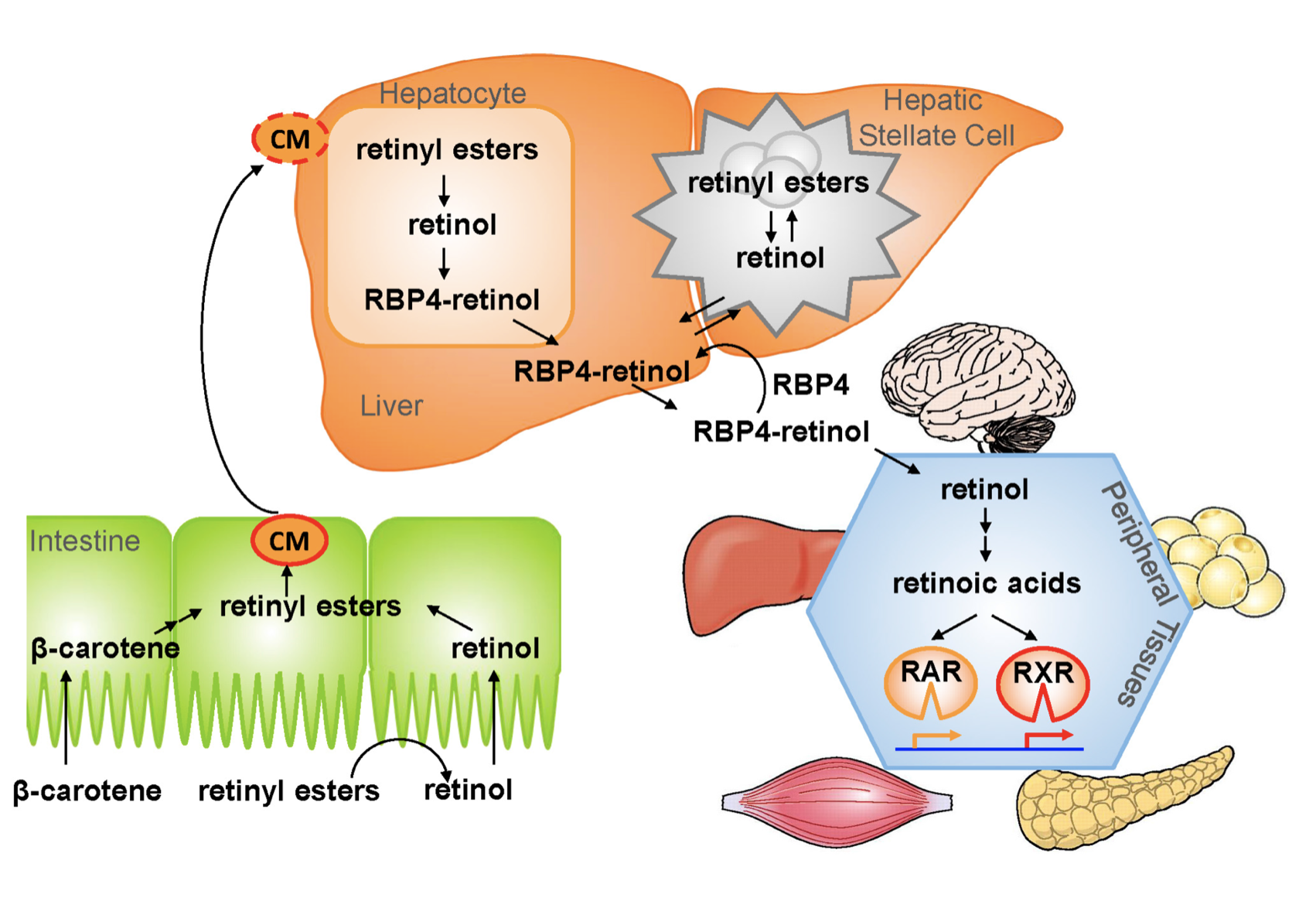
The Physiology of the Vitamin A is as follows:
1.- Ingested food is digested in the stomach where retinyl palmitates (esters) are released from proteins. Retinol and beta-carotene are absorbed directly into the small intestine where retinyl esters and betacarotene are transformed into retinol . Retinol is the most easily absorbed form of vitamin A.
2.-That retinol absorbed by the enterocytes in the ileum (small intestine) along with bile is then transported to the liver with the help of chylomicrons a protein that transports fat.
3.-Fifty to 80% of the vitamin A is stored in the liver and the remaining is deposited into adipose tissue, lungs and kidneys.
4.-When stored retinol is released from the liver into the circulation to target organs, it is bound to plasma retinol-binding protein (RBP4) a transporting protein produced by the liver that requires ZINC, which is synthesized by the liver; This complex is stabilized by transthyretin (TTR), which reduces renal excretion.
Retinol is a crucial component for reproduction, embryological development, cellular differentiation, growth, protein synthesis, and immunity in the form of retinoic acid and vision in the form of retinal.
One of Vitamin A additional roles is in epithelial health of skin and mucous membranes. It increases epithelial turnover which is crucial during would healing. It also has anti-oxidative effects which prevent cell damage and can prevent or reverse the effects of other damaging agents. In addition to these benefits it has also been associated with increasing collagen, fibronectin, keratinocytes and fibroblast, all important in wound tissue structure. There have been some studies that suggest giving higher doses of Vitamin A in patients with non or slow healing wounds.
It is important to remember that we have documents delayed diagnosis of adult vitamin A deficiency leading to significant night blindness in adults. It is critical that the patients and their primary care physicians are acutely aware of this possibility. In majority of the patients with low vitamin A, post weight loss surgery, aggressive supplementations, including injections need to be considered as a part of the treatment regimen.
We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
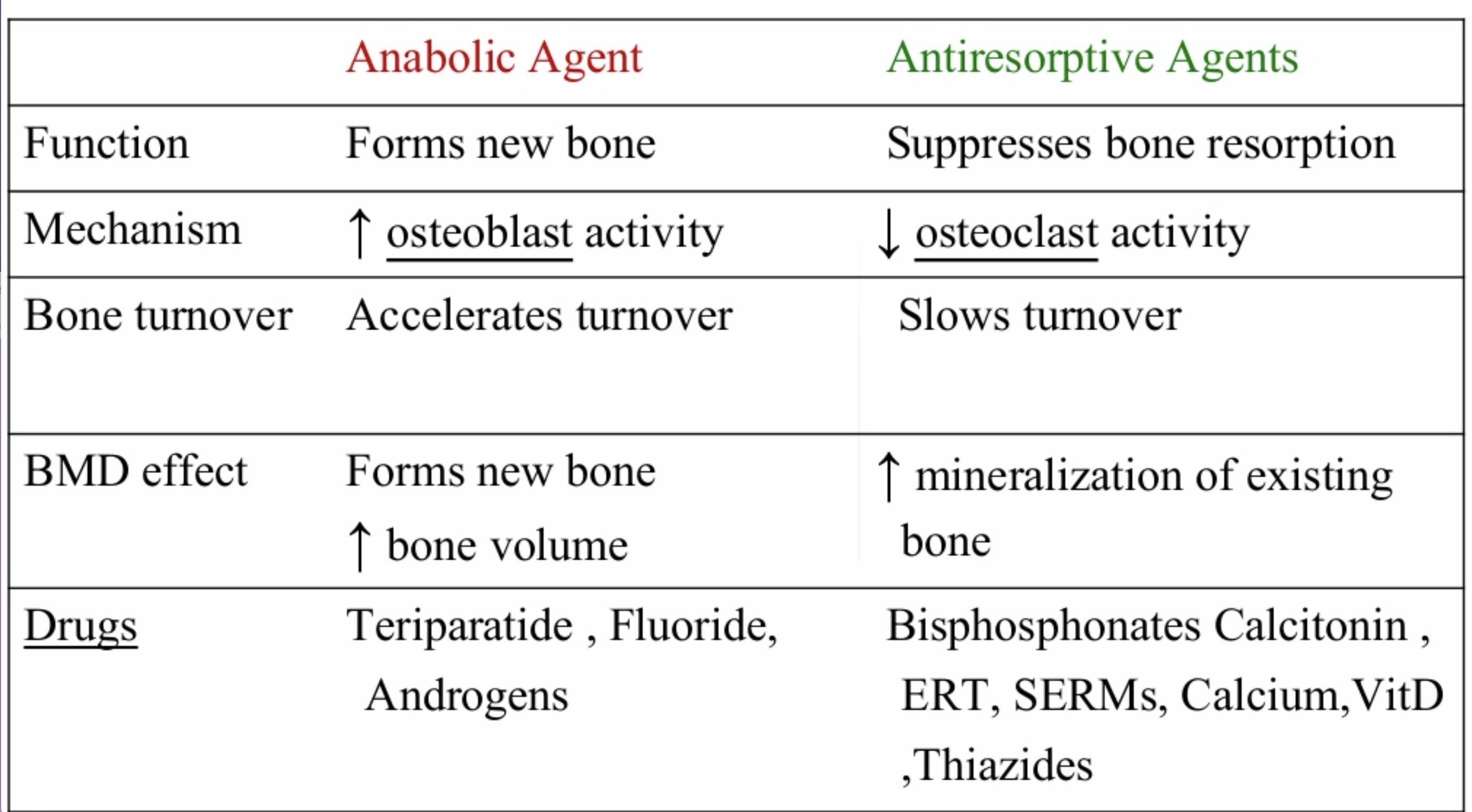
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
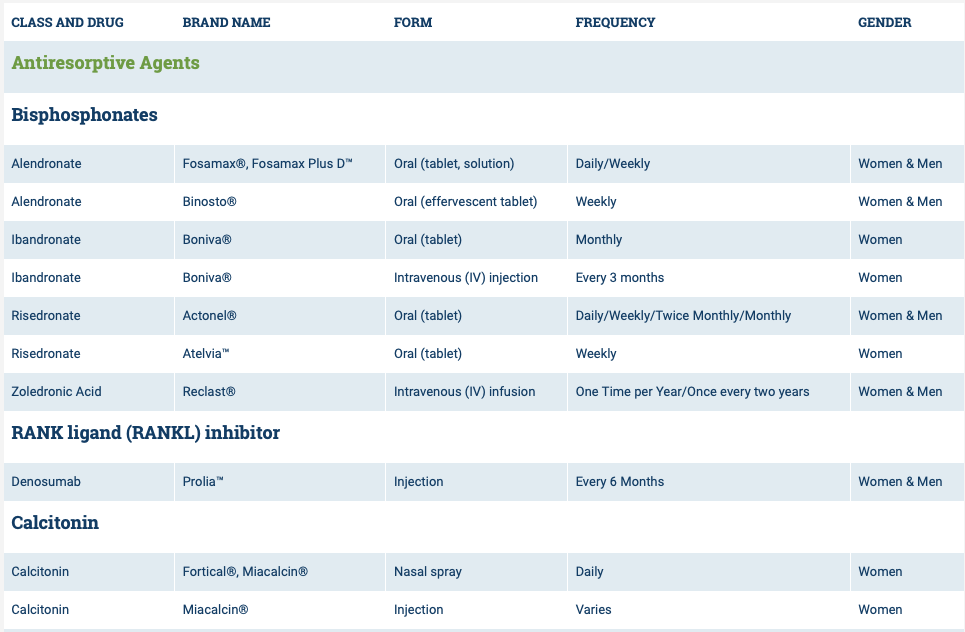
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
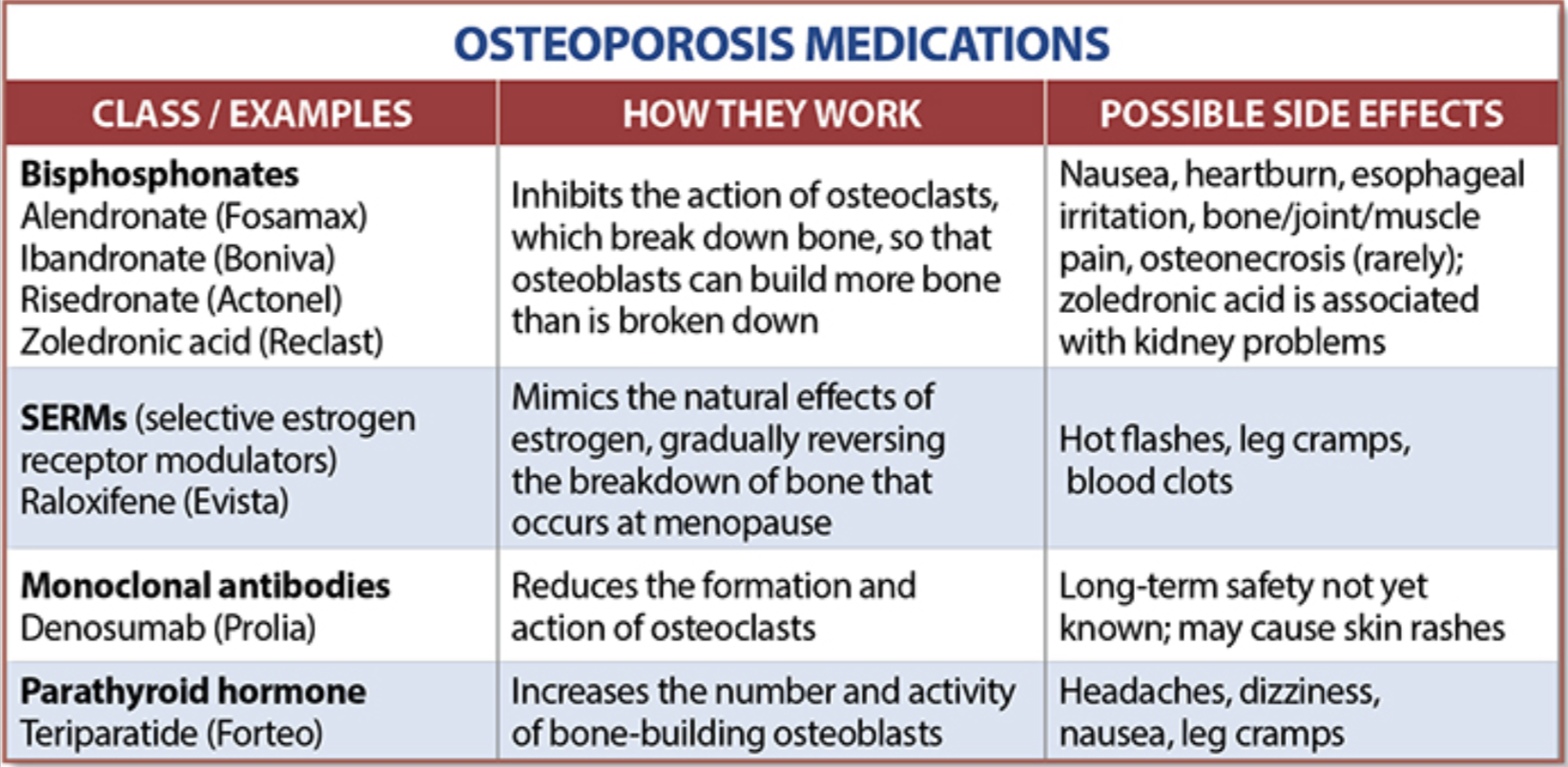
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
Dental Resources
February 24, 2017 10:55 am
You may have heard that I will be giving a lecture at the California Dental Association’s 2017 meeting. In preparation for the lecture, I have come across some excellent information with the assistance of and dental resources from Dr. Armen Mardirossian of Mardirossian Periodontics and Implants.
The following Dental Resources are part of many of the resources I have used to complete this lecture series for the Dental Association. Periodontal disease can effect every body system and should be addressed to avoid further damage and complications. We can not over emphasize the importance of good dental care. In addition, following weight loss surgery, supplementation of vitamins and minerals is extremely important. Always seek the care of a professional when dealing with dental issues or other physical symptoms.
We are sharing these resources with our patient population in order to shed some light on this topic. You can also find a previous webinar on the topic of Dental Issues After Weight Loss Surgery here.
Dental Resources document.

Thank you Dr. Mardirossian for your assistance.
Dual Testimonial: Cameron’s Gastroparesis surgery & Scott’s Revision of a Duodenal Switch
February 01, 2016 8:04 am
In 2015, I came into contact with the most unique, passionate, urgently responsive; talented beyond belief and caring surgeon I have ever met. Our oldest son who is a 21-year-old cancer survivor, has had nearly five years of medical nightmare as diagnosed with severe gastroparesis resultant from his vagal nerve being severed during a previous Nissen Fundoplication surgery. We didn’t find out that this had happened until nearly two years later and only after a 4 hour gastric emptying test showed that Cameron’s stomach was only about 30% emptied after four hours (should be empty after an hour) due to gastroparesis.
I had heard about Dr. Keshishian on a Bariatric support group page on which I post and get great advice. The surgeon back in Central, IL where we live told us that Cameron needed a subtotal gastrectomy to remove 80% of his stomach! This sounded radical and no way in the world was that going to happen. I was given Dr. Keshishian’s email address so I could consult with him for his advice. It was a Saturday morning around 7 AM Central time when I sent off an email to Dr. Keshishian detailing Cameron’s medical history and current issues. I was in hoping that his office would get the email on Monday and hopefully get back to me within a week. I went out to my kitchen to get a cup of coffee and when I returned I had a missed call with a California area code. Yep, it was Dr. Keshishian. I called back and we talked for 45 minutes. He suggested several things and told me that any good general surgeon in my area could do surgery on Cameron and fix him, well that was the only time he was wrong. We couldn’t find anyone in our area who would do the surgery.
So we talked and agreed that Cameron needed a Roux-en Y drain put in place to physically drain his stomach by way of gravity (not for any weight loss as very little small bowel was bypassed). Dr. Keshishian got us in the next week and we flew out to Glendale where he met with Cameron for an examination on that Monday. On Tuesday, Dr. Keshishian performed surgery to fix Cameron’s herniated diaphragm, loose Nissen wrap, performed the Roux-n Y limb and anastomosis to the stomach. Dr. Keshishian also found a Meckel’s diverticulum (a congenital small bowel defect that can cause internal bleeding and serious issues). The following Sunday, Cameron developed severe pain due to chronic pain from his Cancer treatment and 12 subsequent surgeries, many on his abdomen. Dr. Keshishian saw Cameron in the ER and spent 3 hours fixing Cameron’s pain issue and making sure he was medically sound so we could fly home the next day.
Today, Cameron has very little to no issues which you wouldn’t have believed possible six months earlier. In the past, he had violent retching, dry heaving and bad nausea daily which had him severely incapacitated and very depressed due to a feeling of hopelessness and pain from the Gastroparesis. He didn’t believe he had a chance at a normal life but Dr. Keshishian gave Cameron his life back. We are eternally grateful for your huge heart and talent Dr. Keshishian. Thank you!
During our time in Glendale in 2015 for Cameron’s surgery Dr. Keshishian and I began discussing my situation. I had been given a virgin Duodenal Switch performed by a surgeon in Illinois in September of 2013. A year later in 2014 and 180 lbs lighter, I ended up in the hospital as I was passing out. I had a resting heart rate of 35 BPM, a blood pressure in the 75/40 range and incredibly bad labs including anemia, low copper, low zinc, and dangerously low albumin and total protein. A full cardiac work up was completed and I spent a week in intermediate care. Why? I was extremely malnourished even though I was consuming 200-250 grams of protein daily! Why was I malnourished? Because my original surgeon performed a “cookie cutter DS” on me where he didn’t measure my small bowel and arbitrarily gave this 6’2 man a 100 cm common channel and a 150 cm Alimentary limb. Way too short on the AL! Had the Hess method been followed (the only way the DS should be allowed to be completed) my CC would have been 100 cm (that was okay) but my Alimentary channel should have been 275 cm! Simply put, my absorbing portion of small bowel was 34% and the Biliopancreatic limb (non-absorbing) was 66%. It should have been a 50/50 ratio with 100 cm CC, 275 cm AL and a 375 cm BPL. In order to combat my severe malnutrition that September of 2014 I went on a pancreatic enzyme (CREON) to assist my nutrient absorption. I was taking with meals right around 400,000 IU’s of CREON (a boat load) and this was barely keeping my nutrients in range and lab values barely in range. After speaking with Dr. Keshishian, he recommended that I give it until around September of 2015 to see if my absorption increased enough to where a revision wouldn’t be required. Towards the end of July, I all of the sudden lost nearly 20 pounds in two weeks from my already frail and scrawny body. I saw my surgeon in Peoria as I was very alarmed; and I had been having bad cramping and other issues point to a possible bowel obstruction His exact words to me were “see me in 30 days, you are like the DS poster boy of good nutrition”. As you can imagine I found that completely unacceptable and soon as I was out of that appointment I emailed Dr. Keshishian. He told me that if I couldn’t get a revision ASAP I would need to immediately go on TPN. Two weeks later my wife and I landed at LAX and were in Glendale on Monday morning for an exam with Dr. Keshishian.
The job Dr. Keshishian did describing what he was going to do, and of course this was a visual presentation with Dr. Keshishian drawing (you know Dr K’s love of drawing) out for us what he was going to do. He thoroughly explained for my wife and I so she was comfortable with what was going to happen and we fully understood what he was going to do. Doc also found an umbilical hernia that he was going to repair and I had an anal fissure as well that wouldn’t heal so we discussed what he would do to examine and possibly fix during my revision surgery. The next day Dr. Keshishian performed surgery where he fixed the umbilical hernia, measured my total small bowel length to determine appropriate channel lengths and found an repaired a huge mesenteric defect (intestinal hernia and Dr K has a picture of my guts with the huge hole in the mesentery that he has posted on his blog discussing intestinal hernias and blockages), fixed my fissure (Thank you!) and put in a side by side anastomosis that effectively lengthened my AL by 125 cm and my CC by 25 cm worth of absorption. This put my absorbing intestine to BPL ratio where it should have been in the first place (50/50 ratio).
I am pleased to say that I immediately went off the CREON and my absorption and subsequently my lab values improved tremendously. At surgery on August 18, 2015 I weighed a whopping 170 lbs. Today I am weighing in at 183 pounds and well on my way to Dr. Keshishian’s suggested optimal weight target of 205.
Dr. Keshishian is absolutely amazing and the best in the world when it comes to performing the Duodenal Switch and revision to DS Surgery (Band to DS, RnY to DS, Channel extending revision to DS). I would recommend Dr. Keshishian to any patient who needs a virgin Duodenal Switch to get their health back and especially to those who were sold a garbage RnY or Crapband procedure that ultimately failed you (it failed you, you did not fail). In fact, I am trying very hard to convince my brother and Step Mother to fly to Glendale and have Dr. Keshishian perform a Duodenal Switch on them. They very much need it for their health and Dr. Keshishian is the best in the world having performed over 2,000 DS procedures.
I don’t say this lightly. Ara, you are one of the finest human beings I have ever had the good fortune of knowing and your surgical skills are second to none. I really do admire and love this gentleman like a brother and consider him to be a friend. Thank you for using your incredible skill to fix my health issues resultant from the failed cookie cutter Duodenal Switch I was given two years earlier by another surgeon. Had I met you back then and knew what I know now, you would have performed my virgin DS and I would not have suffered for two plus years. Thank you from the bottom of my heart, Dr. K!
Neuromuscular Disease After Weight Loss Surgery
June 08, 2015 11:30 am
Weight loss surgical procedures may result in varying degrees of nutritional deficiencies. Some of these nutritional deficiencies may cause neuromuscular disease if left untreated, these include vitamins, minerals, and protein. The long-term effect of these deficiencies may presents as neuromuscular conditions including, weakness, numbness, confusion and all others if not-diagnosed and untreated. It is important to note that all weight loss surgical procedures require lifetime vitamin, mineral supplements and protein monitoring and possible supplements.
The table below outlines some of the specific neurological and neuromuscular disease complications following bariatric surgery. The most common deficiencies seen with the duodenal switch operation are fat soluble vitamin deficiencies. These include, Vitamin A, D, E and K. Duodenal Switch patients need oral supplements of Dry “Water Miscible” type of Vitamin A, D, E, and K based on their laboratory studies and needs.


The neurological deficiencies are manifested much more frequently with the Gastric Bypass than the duodenal switch operation. The most common nutritional deficients are that of B1, B12, Folate deficiencies that are common in Gastric Bypass. A list of possible neurologic deficiencies and there associated symptoms were summarized by Becker (2012). Another article with Nutritional Neuropathies.
Nutritional deficiencies are seen in a number of illnesses including weight loss surgery patients.
Zinc InformationExclusive Member Content
April 17, 2015 7:22 am