Endoscopic sleeve gastroplasty (ESG) differs from Laparoscopic sleeve gastrectomy (LSG).
ESG (Endoscopic Sleeve Gastroplasty) is promoted and advocated as a low-risk, equal alternative to the Laparoscopic Sleeve Gastrectomy, but it is not.
Anatomically speaking:
Endoscopic Sleeve Gastroplasty is an endoscopic procedure performed under general anesthesia. During this procedure, a specialized endoscope is inserted through the mouth into the stomach. Multiple plastic “H”-type anchors are used to create a fold in the stomach, thereby reducing its size. No part of the stomach is removed. Initial limited weight loss occurs as the patient feels full after consuming small volumes of food. This effect resembles what happens with the lap band and gastric balloon, and we know how the story ends with those.
LSG is performed laparoscopically with incisions on the abdomen under general anesthesia. Seventy-five to eighty-five percent of the stomach, along its greater curvature, is removed, eliminating the part of the stomach that produces the Ghrelin hormone, which controls and modulates hunger. This is why patients feel fuller with a smaller volume of food and experience significantly reduced hunger.
Results:
Please read the fine print
The summary results indicate
“Our results suggest that ESG is safe and effective for the treatment of obesity, with durable
long-term results for at least up to 5 years after the procedure. “
When you look at the details of the results, however, it states:
“At 5 years, mean TBWL was 15.9% (95% CI, 11.7-20.5, p < .001) and 90 and 61% of
patients maintained 5 and 10% TBWL, respectively.”
This means that five years after ESG, 90% of the patients have only lost 10% of their TBWL (total body weight loss), and 61% would have lost 10% of their TBW (Total Body Weight).
This serves as an illustration of how actual outcomes are obscured within the fine print, resulting in a lack of attention from individuals seeking the optimal outcome devoid of perceived risk. The same principle applies to the ongoing discourse regarding GLP-1 medications. The genuine risk associated with ESG and PLG-1 is that patients have undergone alterations to their anatomy and physiology without demonstrable results. Several years into contemplating a treatment promising sustained outcomes, we find that the alterations have increased the overall risk.
As a surgeon, I encourage people to always ask questions and demand that scientific proof be provided. I am not opposed to progress; considering the nature of our practice, we have witnessed and have unrgone significant evolution over the past 30 years, transitioning from performing open cases necessitating a hospitalization period of 4 to 6 days to performing the same cases laparoscopically and robotically in some cases outpatient procedures.
The gastrointestinal staplers simultaneously pass six rows of staples and cut in between them to create two secure lines of staples, three rows on each side. The staples come in different thicknesses and lengths for various applications. Staple cartridges that are used for colon surgery are usually thicker tissue staples than those that are used for small bowel stapling.
Different manufacturers have different color coding.
Another question I frequently get asked is, How does a stapler staple and cut at the same time? The stapler needs to be thick enough to not tear through the tissue and provide uniform pressure for control of bleeding and prevent leaks. It can not be too large either.
When stapling on the stomach for sleeve gastrectomy, the stomach wall thickness is different. We use different-sized staples to accommodate the thicker part of the lower stomach toward the thinner part of the stomach where it meets the esophagus.
Stapler and resulting discharged lines of staples.
Semaglutide (Ozempic, Rybelsus, Wegovy, Saxenda) and tripeptide (Mounjaro) treat type II diabetes. They work thru several complex pathways. An observed side effect that has been noted in diabetic patients has been weight loss.
Some have been advocating using the class of medications for weight loss. However, Wegovy is the only medication approved for weight loss in non-diabetic patients.
There is a lot to be discussed here:
1-the use of the medications for weight loss is an off-label use (except Wegovy)- meaning that the FDA did not approve the medication as a weight loss drug.
The practical implication is that the medication’s safety and complication profile in non-diabetic patients looking to lose weight may be unknown and has not been studied.
2-The medication has become available thru compounding pharmacies. It is crucial to appreciate that compounding medications do not meet the same rigor and standards and may, in fact, not be the same formula as the FDA has stated.. This also means that a compounding pharmacy does not approve the medications in several states.
3-The most critical issue for me is the lack of a “long-term plan.” It is not clear what would happen when the patient stopped the medication. Will the patient experience weight regain? Will the patient require higher doses of the medication to maintain the weight loss, or will the medication stop working altogether? Unfortunately, we do not have these answers. For those skeptical about my questions, let me remind you that phentermine has significant side effects, and almost all patients experience weight gain when they have to stop the medication because of the cardiovascular complication of medication.
In March 2020, the Federal Food and Drug Administration updated the food labeling requirements. Therefore clarifying the information. This was to simplify and improve the information provided to the consumer.
The benefits of weight loss surgical procedures are undisputed. Over the last decades, as the incidence of obesity has increased, so has the need for effective long-term treatment options. It is no secret that diet and exercise plans are only short-term remedies since none of them provide realistic long-term alternatives. Let’s be clear that a healthy diet and activity level are critical to a healthy body and mind and to the long-term success of weight loss surgery.
A frequent question: How young is too soon for weight loss surgery? We work with our patients to ensure that weight loss surgery will not affect the growth of an adolescent patient with regard to height, bone formation, and hormonal status. Specifically, there are concerns about a female patient’s ability to get pregnant and have children. All the scientific evidence points to the benefits of weight loss surgery and the improved ability to get pregnant and bear the pregnancy to completion. Weight loss positively impacts the ability to get and have a healthy pregnancy leading to a non obese child.
An article recently published demonstrated the benefits of early intervention. Specifically, it showed the improved odds of resolution of diabetes in the younger patients (100% in adolescents, Vs. 75% in adults ) at 24 months post-op.
Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
These meetings are for general topics and/or basic question and answers. If you need a more in-depth meeting we would suggest a video or in-person consultation with Dr. Keshishian. You can request a consultation via this link. Contact Us
Written By: Maria Vardapetyan, Eric Baghdasaryan, Osheen Abnous
Vitamins are chemicals that facilitate many processes in the human body such as blood clot formation, good vision, fight infections etc. There are two classes of vitamins. Water soluble vitamins and fat soluble vitamins. Water soluble vitamins dissolve in water. This makes it possible for them to be absorbed through all mucous membranes. Fat soluble vitamins on the other hand do not dissolve or pass through mucous membranes. Fat-soluble vitamins are absorbed in the intestine along with fats in the diet. These vitamins have the ability to be stored in the fat tissues of the human body. Water-soluble vitamins are not stored in the body and have to be taken in daily with the food and dietary supplements. Solubility of a vitamin is not a function of its physical state. There are fat soluble vitamins that have a liquid form and almost all of the water soluble vitamins come in form of pills or powders.
In this article, we are going to focus on fat soluble vitamins. They are all complex molecules made of carbon, hydrogen, and oxygen in different arrangements (see figures 1, 2, 3 and 4). These fat soluble vitamins are vitamin A, D, E and K.
Vitamin A
Vitamin A has a major role in vision, immune function, cell growth, and maintenance of organs such as heart, kidneys, lungs, etc. It plays a pivotal role in the health of our eyes, specifically the retina1. Rhodopsin protein, a major protein that has the leading role in the process of vision, is found in the retina where it allows us to perceive light. This protein requires vitamin A to function properly. Without vitamin A, rhodopsin cannot sense light and thus cannot initiate the process by which vision occurs.
Figure 1: Chemical structure of Vitamin A molecule
Vitamin D
Vitamin D regulates different chemical reactions that are associated with bones, muscles, and the immune system. The simplified way it does this regulation is it helps absorb calcium from dietary nutrients which in turn strengthens the bones, helps neurons exchange signals to move muscles and helps the immune system to fight against viruses and bacteria2.
Figure 2: Chemical structure of Vitamin D molecule
Vitamin E
Vitamin E acts as an antioxidant. Antioxidants are naturally occurring chemicals that neutralize toxic byproducts of many chemical reactions in the human body. When food is consumed and digested, the human body converts it into energy. As a result of metabolism free radicals (toxic byproducts) are formed and are neutralized with the help of vitamin E. In addition, free radicals are also in the environment. Furthermore, vitamin E stimulates the immune system to fight against bacteria and viruses3.
Figure 3: Chemical structure of Vitamin E molecule
Vitamin K
Vitamin K can be obtained from food and dietary supplements. There are two forms of vitamin K: phylloquinone (Vitamin K1), which is found in spinach, kale and other greens and menaquinone-4 (Vitamin K2), which is found in animal products. Vitamin K1 is involved in blood clotting, and Vitamin K2 is involved in bone tissue building. Vitamin K1 is the main Vitamin K in human diet (75-90% of all vitamin K consumed), however, it is poorly absorbed in the body4,5.
Figure 4: Chemical structures of Vitamin K1 and K2 molecules
Absorption of fat soluble vitamins
Polarity describes the inherent charge(positive or negative) or lack of charge for any given substance or molecule.Molecules that are charged are referred to as “polar”, while those that lack charge are “nonpolar”. When discussing solubility, it is important to remember the phrase “like dissolves like”. That means polar (charged) substances like to interact with a polar environment like water, since water contains a slight negative charge. Hence, charged substances are water-soluble. Nonpolar substances on the other hand readily interact with nonpolar environments such as fat, which contains no charge. Therefore, molecules that lack a charge such as vitamins A, D, E, and K are referred to as fat soluble.
Due to their water fearing nature, these fat soluble vitamins cannot simply be absorbed directly into the bloodstream (which is mostly water) like the sugars and amino acids in our diet. As their name suggests, these fat soluble vitamins like to be embedded in fatty droplets, which facilitate their absorption in the following way. Fat soluble vitamins group together with other fat molecules to form fatty droplets, effectively reducing the amount of interaction with the watery environment of the intestines. Therefore, without an adequate amount of fat in your diet, your body is unable to effectively absorb these fat-soluble vitamins. This may be true in an intact anatomy, however, post weight loss surgical patients can not increase their fat soluble vitamin levels by increasing their fat intake. This is due to the fact that a high fat diet causes excessive bowel movement which in turn washes away any vitamins taken by mouth. DS limits fat absorption (thus the great weight loss) which can cause vitamin A and D deficiency that can not be easily corrected with oral supplementation.
As mentioned before, fat soluble vitamins are hydrophobic and nonpolar, which means they are also fat loving or lipophilic. Excess fat soluble vitamins can be stored in the liver and fat tissue. Therefore, these vitamins do not need to be eaten every single day since stores of these vitamins can sustain a person for some time. It may take several weeks or months for our body to deplete these stores of fat soluble vitamins which is why it generally takes a longer amount of time for fat soluble vitamin deficiencies to manifest themselves. The ability to store these fat soluble vitamins in tissues can also lead to vitamin toxicity – marked by an excess of vitamin stores in our body.
Office of Dietary Supplements – Vitamin A. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/#. Accessed April 26, 2020.
Office of Dietary Supplements – Vitamin D. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminD-Consumer/. Accessed April 26, 2020.
Office of Dietary Supplements – Vitamin E. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminE-Consumer/. Accessed April 26, 2020.
Vitamin K. The Nutrition Source. https://www.hsph.harvard.edu/nutritionsource/vitamin-k/. Published July 2, 2019. Accessed April 26, 2020.
Beulens JWJ, Booth SL, van den Heuvel EGHM, Stoecklin E, Baka A, Vermeer C. The role of menaquinones (vitamin K₂) in human health. The British journal of nutrition. https://www.ncbi.nlm.nih.gov/pubmed/23590754. Published October 2013. Accessed April 26, 2020.
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
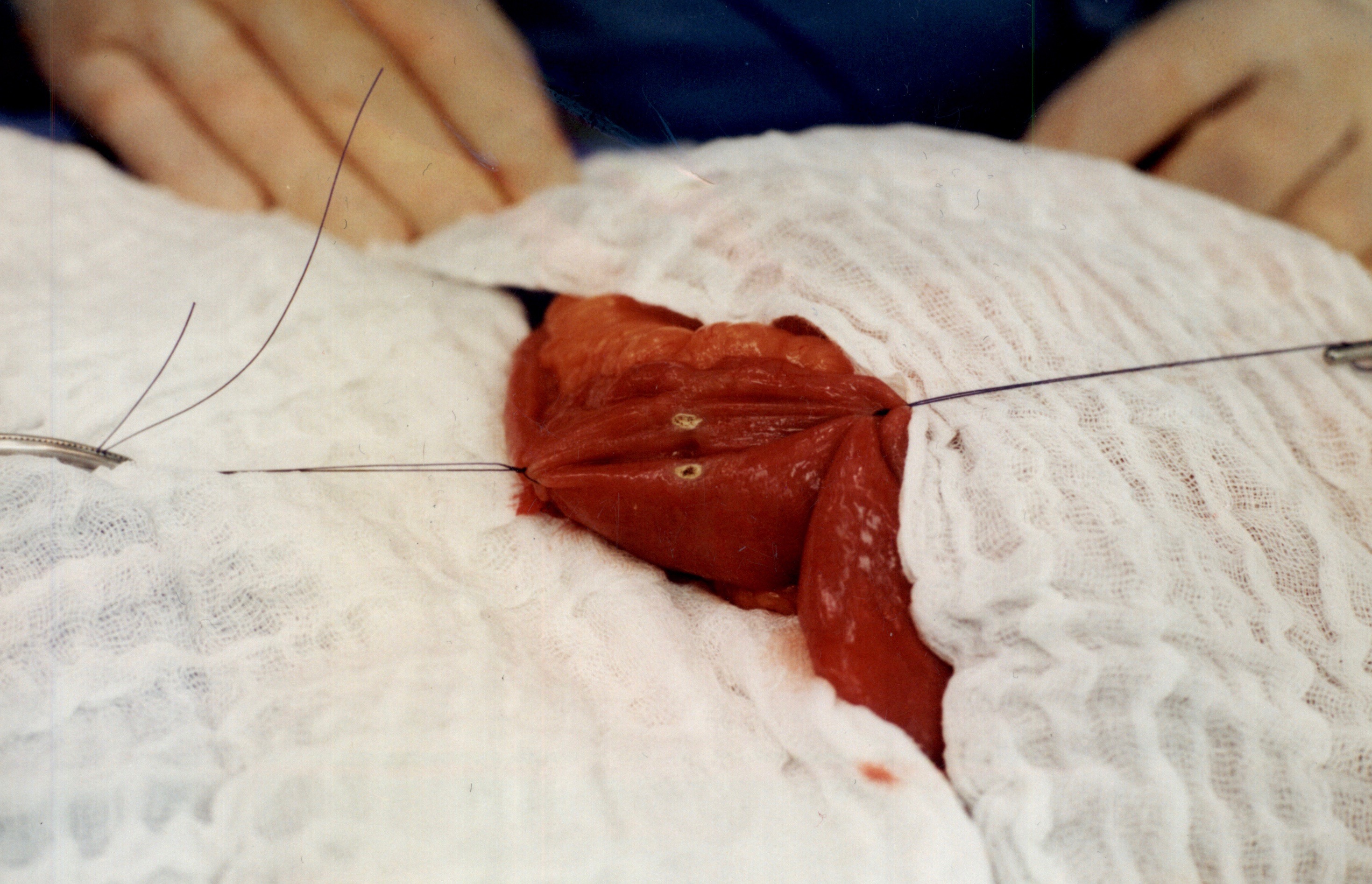
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
The fist step is to align the bowel to be joined.
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
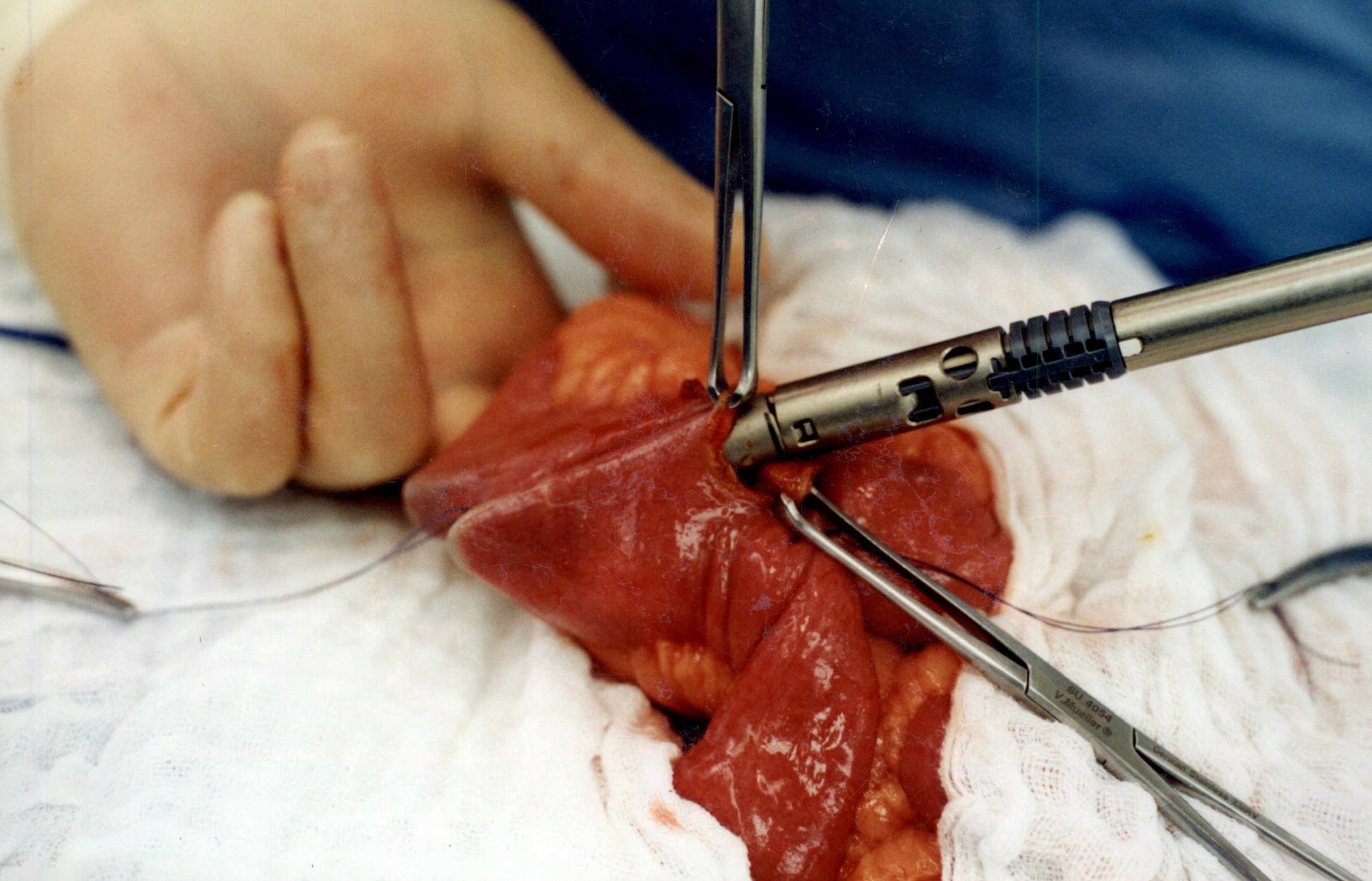
The stapler is then fired in opposite directions to create wide anastomosis.
When the stapler is fired in opposite direction, a very wide anastomosis is created.
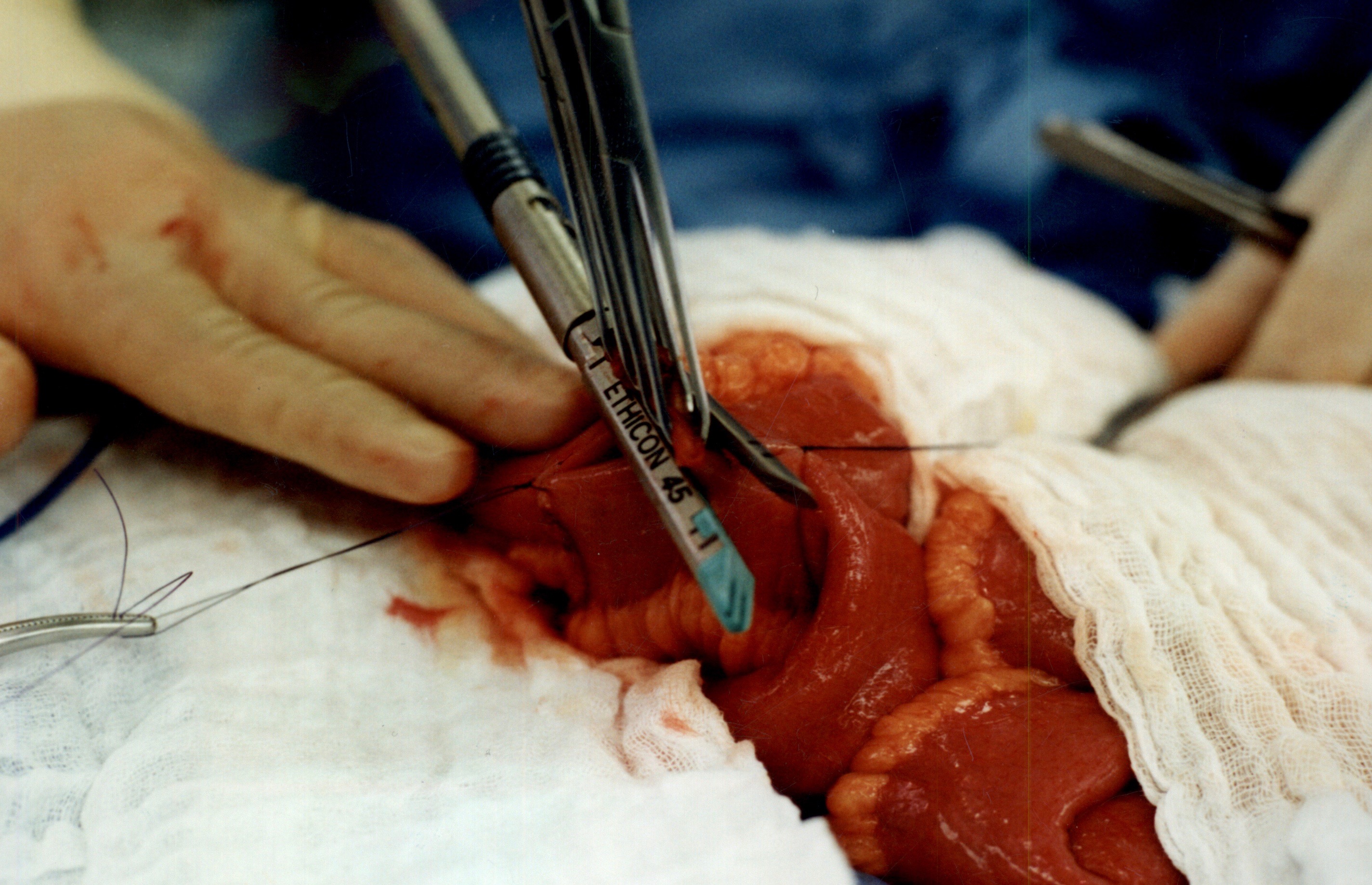
Closing the opening that was made
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.





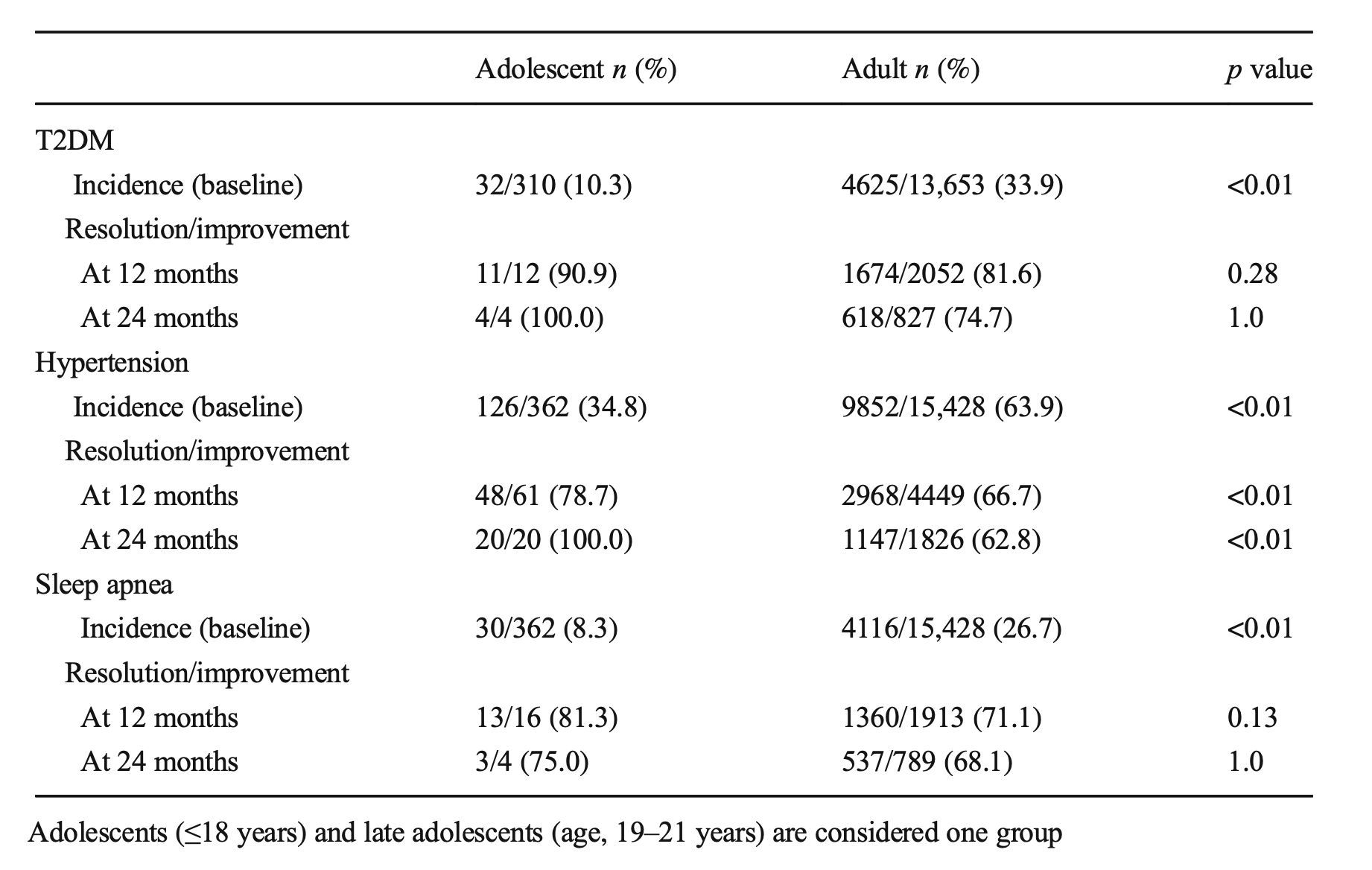

 Figure 2: Chemical structure of Vitamin D molecule
Figure 2: Chemical structure of Vitamin D molecule Figure 3: Chemical structure of Vitamin E molecule
Figure 3: Chemical structure of Vitamin E molecule