Category: Hernia Repair
Articles
March 22, 2020 6:57 pm
Long Term Health Implications of PPI Use, Antacids
November 19, 2019 12:38 pm
The FDA had initially approved almost all PPI’s, and antacids with an explicit limit placed on the duration of the therapy, which ranged in days to weeks. At that time there were no long term studies done on the health benefits, or side effects of the long term use of the PPI.
This Summary Letter outlines all the concerns dating back to 2011. I have found the information in this letter a good overview of the supporting medical evidence and lack of any long term data in regards to long term PPI.
The FDA made changes in the Black Box warning of the PPI medications. This was done with the mounting evidence and the health concerns of long term PPI use.
PPI’s have been shown to have detrimental long term side effects. It is prudent that a patient is continuously monitored and evaluated for identification of the possible underlying causes of the reflux, that may be the reason for the PPI use. There are a whole host of potential causes of reflux and other options for treatment.
There have been numerous studies recently published:
It can lead to increase risk of fractures and in a large study from the VA system it has been associated with the risk of premature death
Gastroesophageal Reflux: Bile Vs. Acid
May 14, 2019 12:52 pm
Gastroesophageal (GE) reflux is the condition when the stomach contents are able to “reflux” back through an incompetent lower esophageal sphincter (LES) into the esophagus.
Gastroesophageal reflux Disease (GERD) is a clinical condition caused by long-standing reflux that results in microscopic and visible changes to the inner lining of the esophagus and esophageal mucosa.
GERD is nondescript as to the cause of the condition. It only states that the stomach contents have been irritating the lining of the esophagus on a chronic basis. This can be caused by an anatomical abnormality of the GE junction (hiatal hernia) or may be related to dysfunction of the LES. Other possible causes of GERD may be infection (H. Pylori), environmental (stress), and dietary (nicotine, alcohol, caffeine, spicy food) in origin.
So far, we have not clarified the chemical nature of the refluxed content.
In Acid Reflux, the relative acid overproduction of acidic secretion and the exposure of the esophageal mucosa need to be addressed. This is accomplished by acid suppression medications, anti-histamine (H2 blockers), and Proton pump inhibitors (PPIs). The physiology and the mechanism involving this condition are well understood. As a surgeon, however, I do see patients who should have had surgical intervention. The initial mode of therapy for a patient with documented acid reflux and or symptomatic hiatal hernia is placing them on medication. These patients are then recommended to have a related upper endoscopy. Patients who do not improve or where deterioration of the esophageal mucosa and the presence of precancerous cells are referred for surgical intervention.
Bile Reflux, contrary to acid reflux, may have tiny, if anything, to do with the LES. The symptoms experienced by the patient may be as after related to the excessive bile in the stomach, which is seen frequently
after cholecystectomy, or in those patients with a dysfunctional gallbladder (low EF on HIDA scan).
The treatment of Bile reflux is Duodenal Switch without the associated sleeve gastrectomy component in addition to repair of hiatal hernia if present. Ann Surg. 2007 Feb; 245(2): 247–253.
Adhesions, Internal Hernia And Bowel Obstruction
December 15, 2018 2:35 pm
Adhesions are fibrous bands of scar tissue that form during the healing process. Following surgery, many people live normally with this scar tissue. However, they are also the cause of bowel obstruction when the adhesions form in such a way that causes a segment of the bowel to either get trapped, or form a “knot”. In both of those cases, the end result is a partial narrowing or a complete blockage of the intestines. This is called bowel obstruction.
Without treatment, the blocked parts of the intestine can die, leading to serious issues. However, with prompt medical care, intestinal obstruction often can be successfully treated.
Other causes of bowel obstruction:
- In children, the most common cause of intestinal obstruction is telescoping of the intestine (intussusception).
- Intussusception telescoping of the interstine
- Hernias — portions of intestine that protrude into another part of your body
- Inflammatory bowel diseases, such as Crohn’s disease
- Diverticulitis — a condition in which small, bulging pouches (diverticula) in the digestive tract become inflamed or infected
- Twisting of the colon (volvulus)
- Impacted feces
- Colon Cancer
In patients who haven’t Bariatric / weight loss surgery or an untouched GI track, bowel obstruction may manifest itself by symptoms of loss of appetite, constipation, nausea, vomiting, enlarged abdomen, abdominal pain, cramping, with no passage of gas or bowel movements.
However, patients who have had a weight loss surgery (Duodenal Switch, or the Gastric Bypass) because of the parallel limbs of the small bowel, the symptoms outlined above may not present. The diagnosis of a bowel obstruction, when suspected, should be identified with CT scan of the abdomen and pelvis with Oral and IV contrast. A CT scan with no oral contrast or water instead of oral contrast is inadequate and may lead to a delay in diagnosis and surgical intervention. Examples of Bowel Obstruction CT findings were discussed previously.
The treatment for an internal hernia and adhesions causing a bowel obstruction depending on the severity may range from observation to surgical intervention in order to release the small bowel from the constraints of the adhesions.
Reflux and Hiatal Hernia
April 17, 2017 9:41 am
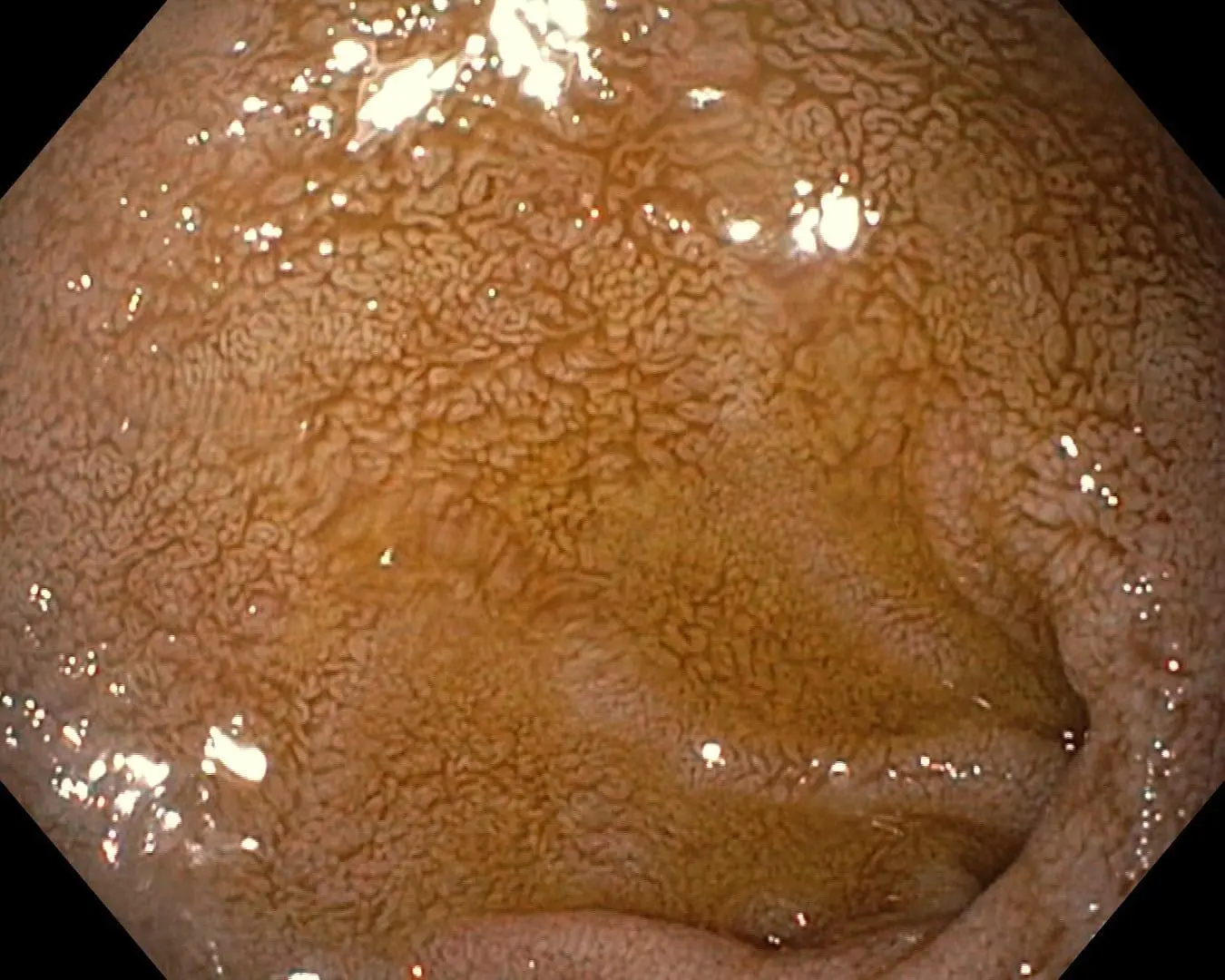
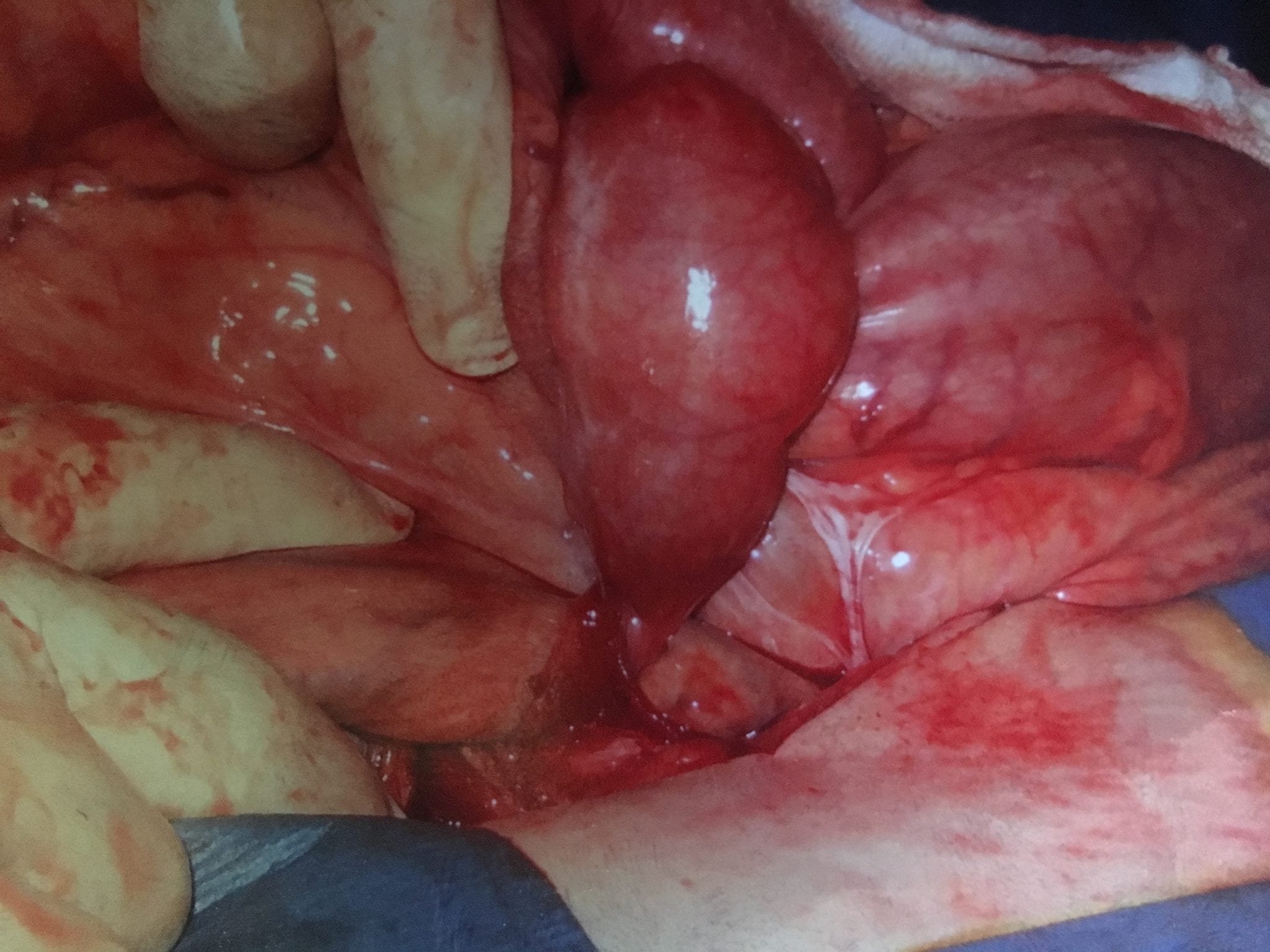
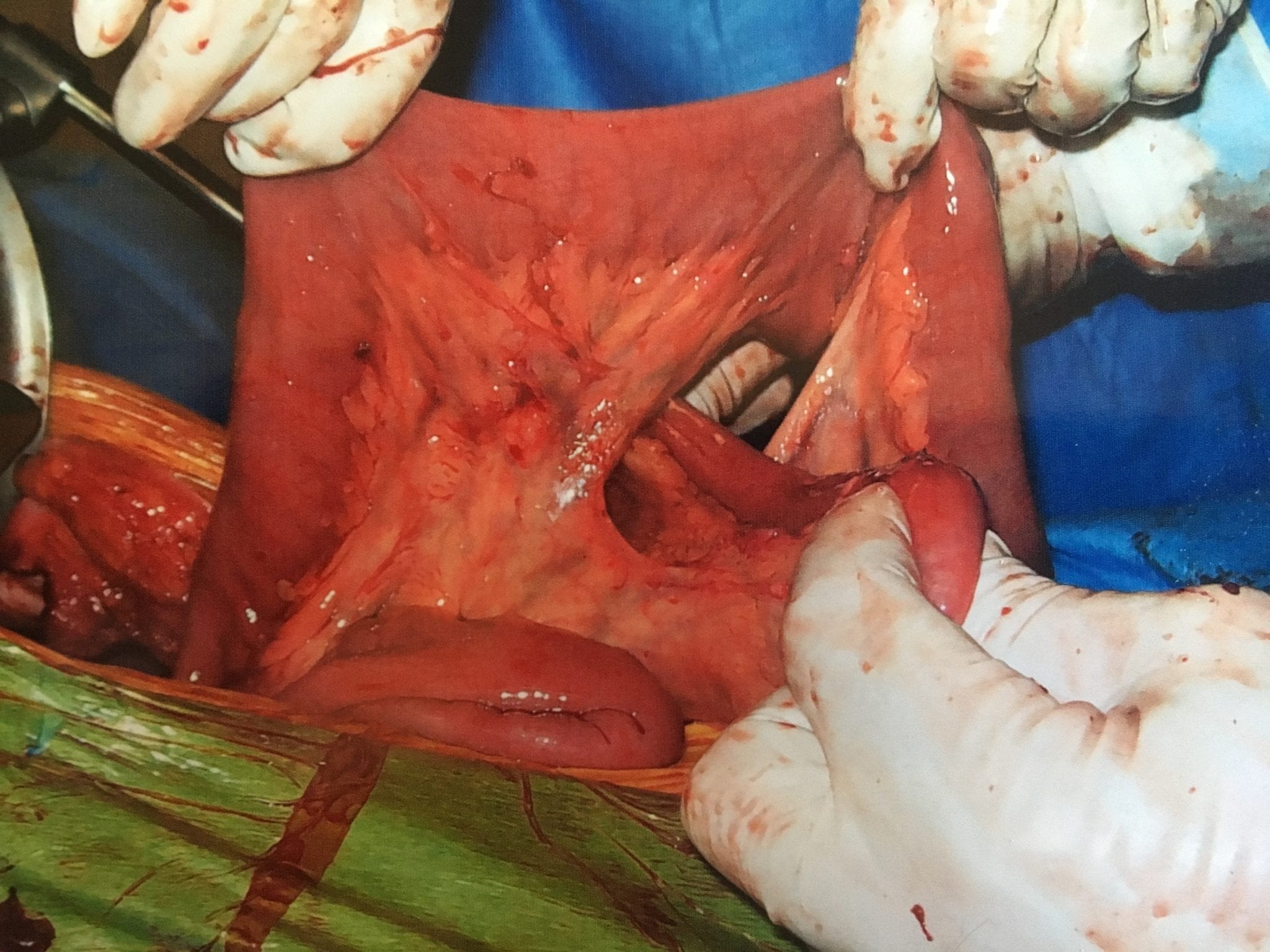
One of the leading reasons for Gastro-esophageal reflux disease (GERD) is a physical defect called a Hiatal hernia. The esophageal Hiatus is the opening in the diaphragm where the esophagus enters from chest cavity allowing the esophagus to pass into the abdominal space. If the opening in the diaphragm is much larger than the esophagus, it will result in reflux of the stomach secretions and food from the stomach into esophagus. *Note: Graphic surgical pictures below
Hiatal Hernia Causes:
- heavy lifting
- coughing
- obesity
- injury
- persistent vomiting
- age related
Reflux and Hernia Symptoms:
- sour taste
- reflux
- heartburn
- belching
- chest or abdominal pain
- difficulty swallowing
- vomiting
- no symptoms


The treatment includes dietary changes, medication and in those who do not improve surgery.
Hiatal hernia repair includes tightening of the dilated opening of the esophageal hiatus by re-appoximating the separated muscle fibers of the right and the left crus. This tightens the defect in the diaphragm and helps prevent part of the stomach or stomach contents from entering the chest cavity.
You can find further information and dietary changes regarding Hiatal Hernia and GERD here, including information unique to weight loss surgery and Hiatal Hernia. You can also find further surgical information, as well as a surgical video here.
BMI Threshold for Ventral Hernia Repair
July 21, 2016 2:48 pm
“After Ventral Hernia Repair (VHR), complications are most likely to occur in patients with BMI ≥ 40 kg/m2. This subset of patients also had a significantly higher risk of undergoing surgery for a recurrent hernia, suggesting that this group of patients is likely to experience adverse outcomes after VHR and should be counseled to consider bariatric surgery prior to attempts at VHR.” Information on Bariatric Surgery here.
Read more of the original article here….
A hernia is present when part of an internal organ or tissue bulges through a defect or weak area in the belly wall (fascia). The type of hernia you have depends on where it is and how it occurs. Ventral Hernias are named after the location in the body they occur. A ventral hernia is a bulging of the abdominal wall anteriorly. When the hernia is located at the site of a pervious surgical scar then it is called an incisional hernia. A hernia can occur at any location of the abdominal wall however. Further information regarding incisional hernia here.

A Ventral Hernia can develop due to straining, lifting or increased abdominal pressure and is a weakening of the abdominal wall. Usually fat and internal organs bulge outside the facsia that holds the internal organs within the abdominal cavity. This type of hernia can be asymptomatic or cause pain with pressure or exertion. If left untreated, they can become larger or become incarcerated requiring emergent surgical intervention. Dr. Ara Keshishian performs ventral hernia repairs using a laparoscopic technique that may or may not require mesh repair. Mesh is place behind the defect in the abdomonial wall and extends past the hernia edges. Mesh is used to re-enforce the abdominal wall and allowing the healing tissue to form a sturdy foundation to help prevent reoccurrence of the hernia. Videos of Ventral Hernia Repairs here.
Failure of Anti-Reflux Procedures
September 28, 2015 7:13 am
A recent study Published in JAMA Surgery, quoted rate of 10-20% of patients who have had anti-reflux surgical procedures will have recurrence of his symptoms within the research data. There are numerous studies that have identified predictive factors leading to return of the symptoms after surgical intervention. Some of these predictive factors are improper diagnosis, inadequate work up and technical issues.
Due to the significant rise of sleeve gastrectomy as well as a high failure rate of the lap band, we have seen several patients presenting with significant reflux disease after weight loss surgery. There is a little scientific data regarding the failure of anti-reflux procedures in patients who have had previous weight loss surgical operations. In our practice, however, we have extensive experience with anti-reflux operations in patient who have had previous weight loss surgeries including Gastric Bypass, Adjustable Gastric Banding, Sleeve Gastrectomy and Duodenal Switch operation.
Improper diagnosis, inadequate work up, and technical issues have been cited as possible causes for recurrence of symptoms in patients who have not had weight loss surgery. One could assume that those variables are still a factor in addition to other factors resulting from a previous weight loss surgery. The complications of a previous weight loss surgery can not be under-estimated; an example would be a patient with significant esophageal motility issues directly related to an Adjustable Gastric Band. Other situations that exacerbate symptoms of reflux are an hour glass shaped sleeve or a stricture mid stomach post Sleeve Gastrectomy or Duodenal Switch.


In our experience, some patients have responded well with anti-reflux surgical procedures and mesh placement if indicated after a compete work up with has included and upper endoscopy, upper GI series, manometry and Ph studies. Any patient with symptoms of reflux after weight loss surgery, should be evaluated, and a complete work up should be performed to establish the proper treatment options. It is not wise to have patients be treated with proton pump inhibitors as a default treatment without a complete work up for any patient with reflux. These class of medications have significant side effects associated with them. Furthermore, prolonged reflux is a factor in development of Barret’s Esophagus, a pre-cancerous condition.