Cholangitis refers to infection and inflammation of the bile ducts because of obstruction and introduction of bacteria or other pathogens from the GI tract.
The treatment for biliary cholangitis requires intervention, surgical or advanced gastroenterology, and involves
Hydration with IV fluids,
Broad coverage with IV antibiotics administration and
Drainage procedure (ERCP, papillotomy, Stent placement, Cholecystectomy with common duct exploration, and T-tube placement)
These steps are almost all taking place concurrently and urgently. This is not something a patient waits and sees how it goes- it only goes one direction, from bad to worse. This is not to sound alarmist; a correct diagnosis is critical.
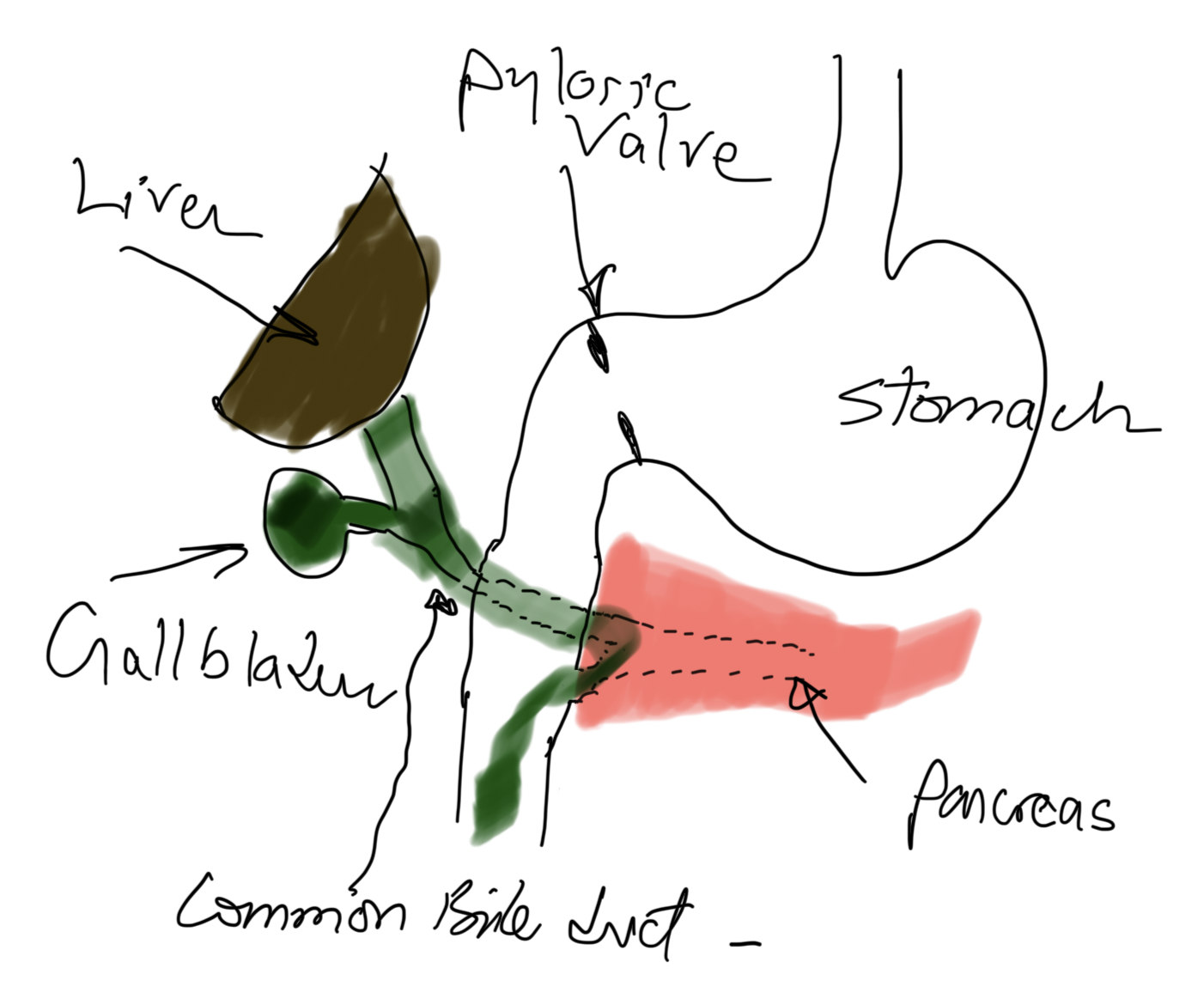
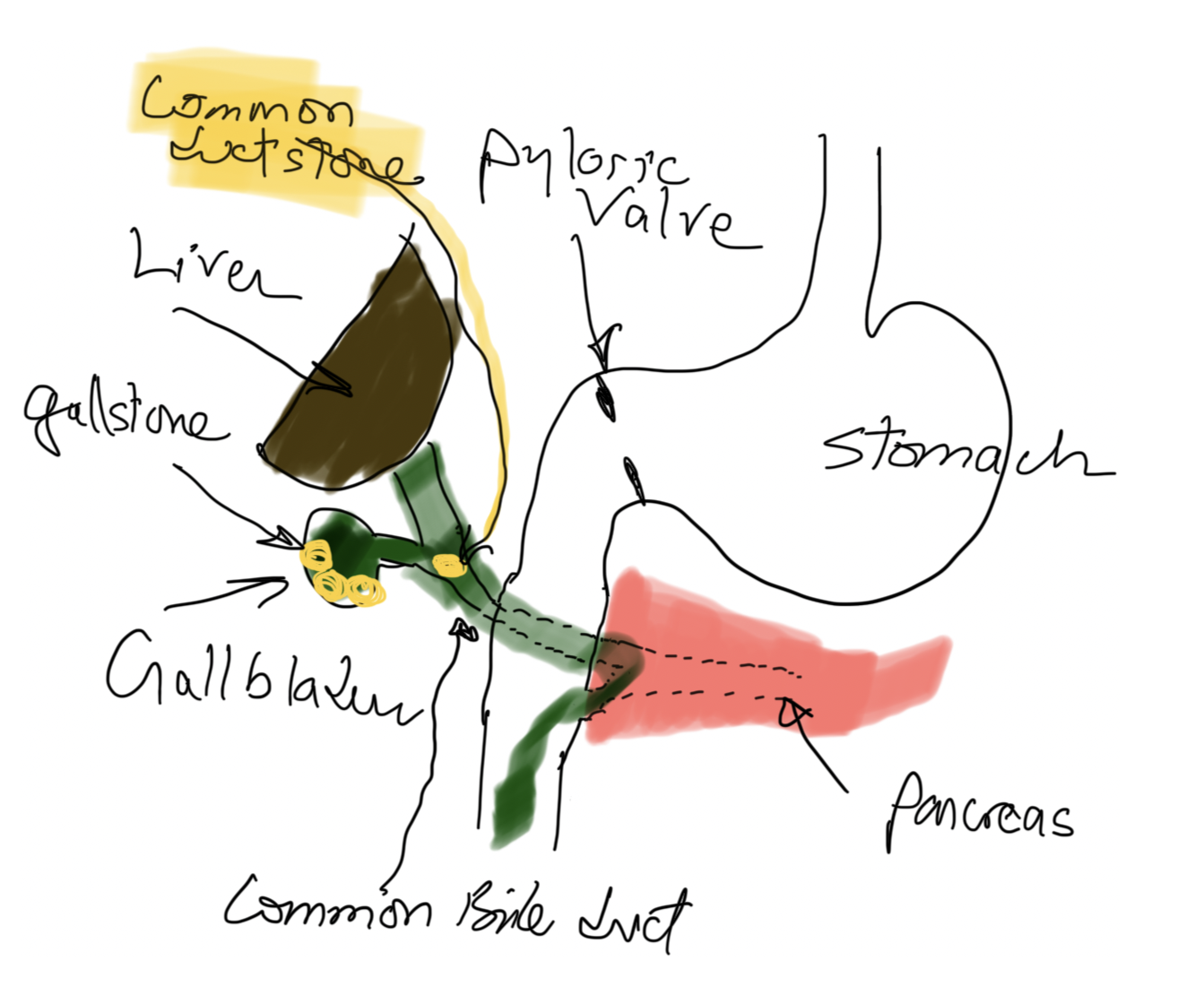
Risk factors for cholangitis may include gallstones that travel down the bile duct and cause jaundice, pancreatitis if passed, immunosuppression, malnutrition, and diabetes, to name a few.
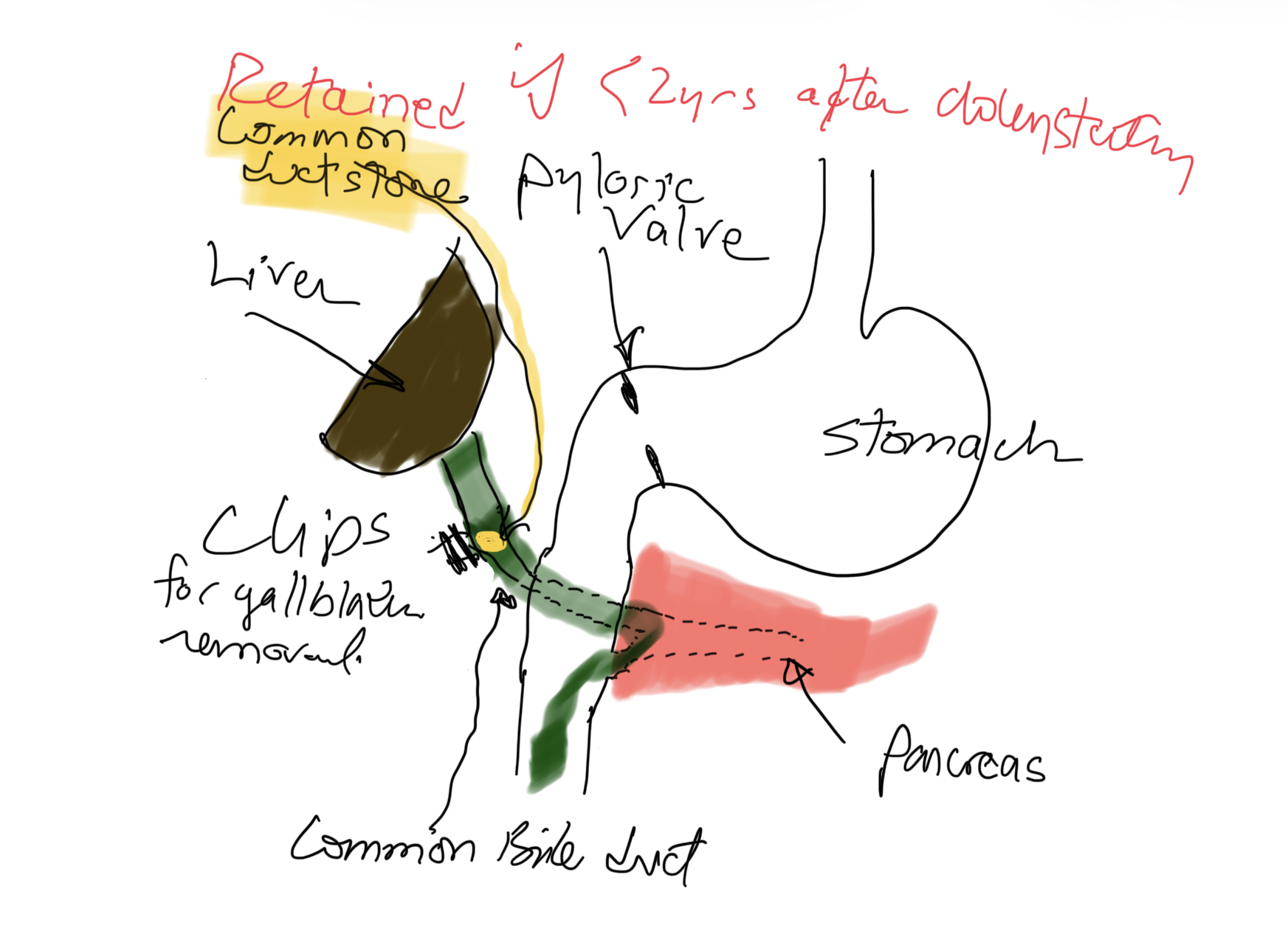
If a patient has gallstones in the bile duct less than 2 years after cholecystectomy, it is a Retained Stone(s), meaning there was a small stone that was not in the gallbladder and was not seen on US, intraoperative cholangiogram, or ERCP (if performed before surgery).
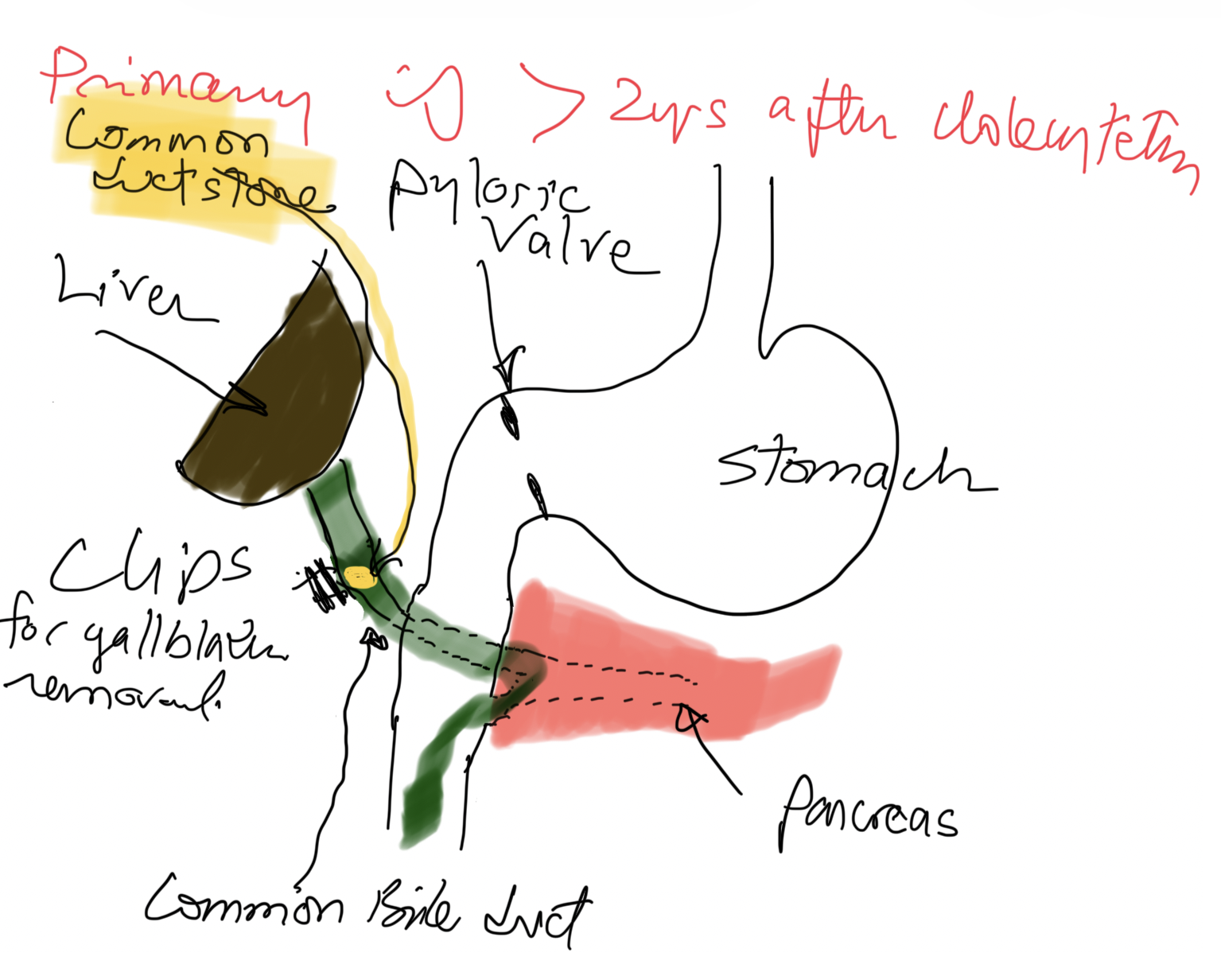
If a patient has gallstones in the bile duct more than 2 years after cholecystectomy, they are Primary Biliary Stone(s), meaning the stone(s) formed in the biliary tree after cholecystectomy.
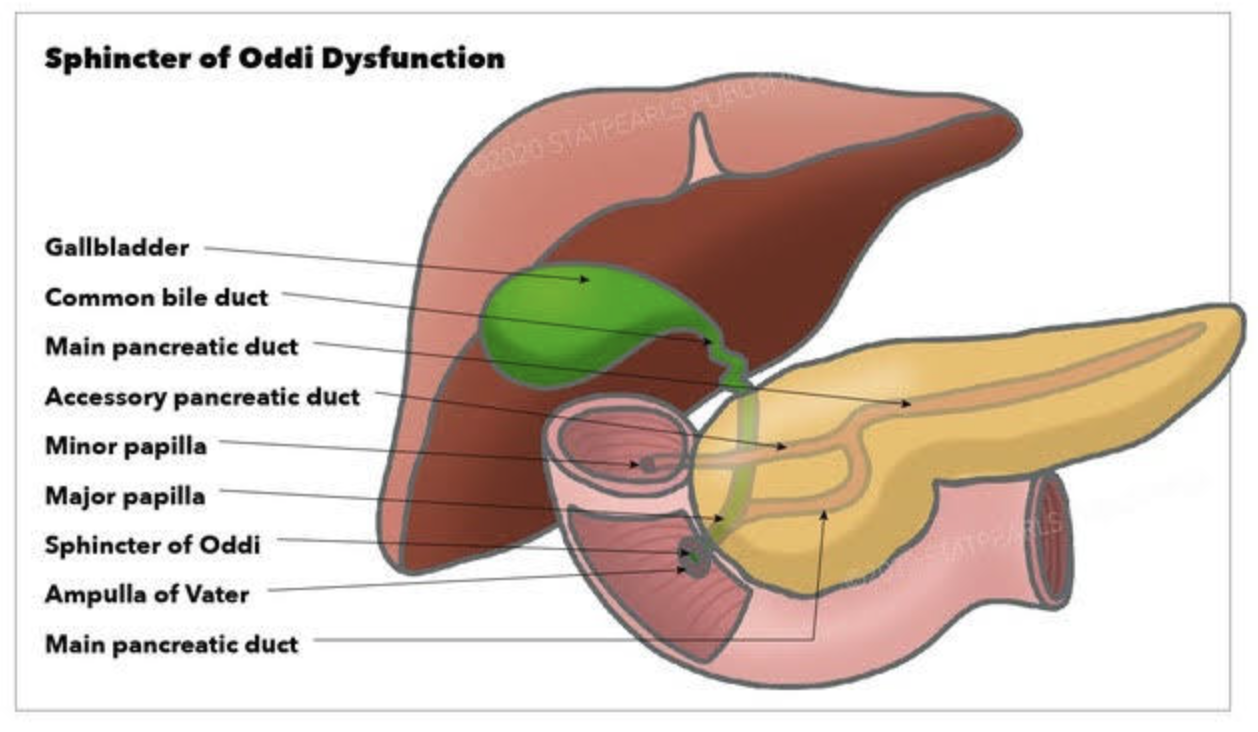
Sphincter of Oddi Dysfunction (SOD) is a clinical syndrome characterized by biliary/ pancreatic pain from abnormal function or obstruction of the.
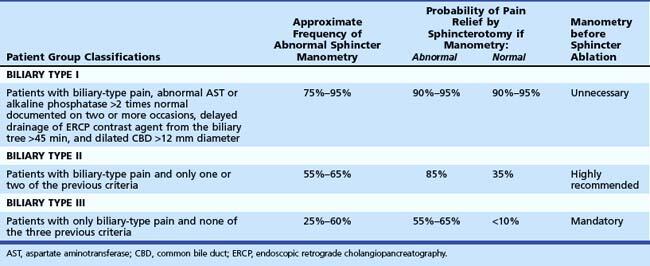
It is commonly considered after cholecystectomy when ongoing biliary-type pain or pancreatitis is present. SOD is classified into three Milwaukee/Rome types based on clinical, laboratory, and imaging criteria. Type I shows objective ductal dilation and enzyme abnormalities, type II has biliary pain with either dilation or enzyme elevation, and type III has biliary-type pain without objective abnormalities.
Diagnostic and classification
The SOD spectrum includes biliary, pancreatic, or combined sphincter dysfunction, with symptoms driven by dyskinesia or mechanical obstruction. The term SOD encompasses both functional motility disorders (biliary or pancreatic sphincter dysfunction) and mechanical obstructions such as papillary stenosis.
SOM has been considered the gold standard for diagnosing elevated basal sphincter pressure. It is invasive and carries complications, including pancreatitis. SOM can also not be done in those who have had gastric bypass or duodenal switch operations. Sphincterotomy outcome is not uniform. Consequently, many centers have moved toward empiric endoscopic therapy for appropriately selected patients and toward noninvasive or less invasive diagnostic approaches for others.
Treatment approaches
Endoscopic biliary sphincterotomy (EST) is the most established nonpharmacologic treatment for biliary SOD, particularly in type I and many type II patients with objective ductal dilation and/or enzyme elevation.
In type II SOD, outcomes after EST correlate with objective evidence of obstruction or sphincter hypertension on SOM. Empiric sphincterotomy without manometry is controversial.
Type III SOD has emerged as predominantly functional pain rather than a mechanical obstacle. Alternative management emphasizes risk stratification, noninvasive strategies, and multidisciplinary approaches.
Medical and non-sphincterotomy options (calcium-channel blockers, nitrates, antidepressants, and lifestyle modifications) have been discussed as potential adjuncts or alternatives.
Summary
SOD is a multifactorial biliary and pancreatic sphincter disorder with a spectrum from mechanical obstruction to pure dyskinesia. Type I and II retain treatment relevance, particularly EST for biliary obstruction. Type II management requires clear identification of the cause.
SOM is a diagnostic tool with significant limitations.
Endoscopic sphincterotomy offers meaningful symptom relief in type I and select type II with objective obstruction. It carries a risk of complications, including pancreatitis; risk mitigation strategies are integral to practice. In type III SOD, sphincterotomy generally has limited benefit, necessitating a move toward noninvasive management and careful patient counseling. Patients post- gastric bypass, or duodenal switch, can not have ERCP or SOM done.
There are 4 parathyroid glands which are located behind the thyroid gland, among other functions, are the main regulators of calcium, phosphorous, and magnesium in the blood. Elevations of parathyroid hormone (hyperparathyroidism) can be: 1-Primary, 2-Secondary, 3-Tertiary
Primary hyperparathyroidism means the parathyroid glands themselves are hyperactive. This may involve only one of the four glands: a) an adenoma, a benign tumor that needs surgical removal, or b) hyperplasia, when all 4 glands are hyperactive and/or enlarged, and in some cases, most of the 4 glands need to be removed.
Secondary hyperparathyroidism means that the elevated PTH level is caused by an external regulatory stimulus, such as low calcium, which itself may be due to low vitamin D, low calcium intake, or other causes.
Tertiary hyperparathyroidism is seen only in specific renal failure and transplant patients.
Regardless of the type of hyperparathyroidism, the end result is the same. Because the parathyroid gland aims to maintain normal calcium levels, it will do everything to achieve them. This includes increasing calcium absorption from the GI tract, breaking down bone to increase the blood calcium supply, and increasing calcium reabsorption from the urine.
Distinguishing between primary and secondary is critical, as primary is more likely than not a surgical problem that needs to be addressed. Secondly, it may be responding to metabolic deficiencies (low CA, low Vitamin D) that need to be corrected and take some time.
Not all cases require surgical intervention, as labs (vitamin D, calcium, and alkaline phosphatase) and imaging studies, such as neck ultrasound, CT scan, and Sestamibi scan, provide the information needed to dictate the treatment plan. Please stay up to date with your yearly lab results to catch changes sooner rather than later.
There have been numerous fad-type treatments promising easy, quick, low-risk, non-surgical treatment over the years, offered for the treatment of obesity. HCG injection, Phen-fen, Lap band, Orlistat (Xenical), Gastric balloon, GLP-1, and now endoscopic gastroplasty. The one thing they all have in common is the reported short-term outcome comparable to the long-term outcome of the surgery. Surgery has the longest history for sustained weight loss with data going back decades showing long term comorbidity resolution.
GLP-1, GIP class of medication reports the outcome 1-2-3 years compared to the 15-30 years outcome of the weight loss surgical procedures. These articles also fail to emphasize the high cost and comprehensive long-term risk with injections or pills taken daily or weekly.
Now to the latest fad: The results of the endoscopic gastroplasty are reported to be in the form of a 3-5-year interval. What these alternative low-risk treatments also have in common is the emphasis placed on short-term resolution of comorbidities and weight loss. The 5-year weight-loss rate is a dismal 11.8% (Total Body Weight Loss, %TBWL) (Lahooti et al., 2025). A 300-lb. person with gastroplasty will be down 34 lbs. in 5 years – compared to 100 lbs. following sleeve gastrectomy. Not surprisingly, the Endoscopic gastroplasty was found to have a 2.6% rate of serious adverse events (SEA) (Singh et al., 2019). Yet, the patients are under the impression that since gastroplasty is not a surgical procedure and no incisions are made, there are no serious risks.
One of the original first studies (Abu Dayyeh et al., 2022) also presented a set of data that one has to read the detailed findings to appreciate how poor the performance of the procedure is:
“Findings:Between Dec 20, 2017, and June 14, 2019, 209 participants were randomly assigned to ESG (n=85) or to control (n=124). At 52 weeks, the primary endpoint of mean percentage of EWL was 49·2% (SD 32·0) for the ESG group and 3·2% (18·6) for the control group (p<0·0001). Mean percentage of total bodyweight loss was 13·6% (8·0) for the ESG group and 0·8% (5·0) for the control group (p<0·0001), and 59 (77%) of 77 participants in the ESG group reached 25% or more of EWL at 52 weeks compared with 13 (12%) of 110 in the control group (p<0·0001). At 52 weeks, 41 (80%) of 51 participants in the ESG group had an improvement in one or more metabolic comorbidities, whereas six (12%) worsened, compared with the control group, in which 28 (45%) of 62 participants had similar improvement, whereas 31 (50%) worsened. At 104 weeks, 41 (68%) of 60 participants in the ESG group maintained 25% or more of EWL. ESG-related serious adverse events occurred in three (2%) of 131 participants, without mortality or need for intensive care or surgery.”
1-This study is about 85 patients having the endoscopic gastroplasty and 124 patient only being on diet (they compared the endoscopic gastroplasty (ESG) to diet and exercise, not sleeve gastrectomy)
2-at one year, the ESG group had lost 49.2% of the EWL (if needed to lose 100 lbs, only lost 49.2lbs)
These are examples of how patients need to educate and inform themselves beyond the headlines and ask the tough questions.
GLP-1/GIP class of medication has been promoted for everything under the sun (a little exaggeration here to make the point). Even though it may be true that many comorbidities resolve with any form of weight loss, we also know from weight-loss surgical data that many of these comorbidities return with weight gain. Which is why, in my opinion, it is deceptive to talk about the resolution of comorbidities with very little weight loss from alternative procedures such as lap band, gastric balloon, or endoscopic gastroplasty, when we know the comorbidities are resolved only when the weight loss is maintained long term.
Weight loss is maintained by Lap band adjustment (with the associated cost- and hopefully not having complications such as slipped band or continuous nausea and vomiting) or by replacing the gastric balloon every 6 months (how does that make sense), or by having the daily or weekly injection or pills of GLP-1, GIP class of medications with the risk of side-effects and the costs associated with these medications. All of this in the backdrop of near-certain weight gain when the lap band must be removed, or the gastric balloon is not reinserted, or the GLP-1 GIP medication is stopped (primarily because of the complication)
Weight-loss surgical procedures, such as Duodenal Switch, gastric sleeve, and Gastric bypass, are not risk-free. However, they have continually been shown to deliver sustained weight loss over decades.
As a surgeon with decades of experience with operating on patients with failed lap bands, endoscopic gastroplasties, GLP-1-GIP medications, and gastric balloons, one thing is common that patients say is how little they knew about their options. Patients who consider only the short-term outcome and perceive the least risk will require secondary treatment, which will deliver a more definitive result.
References
Abu Dayyeh, B. K., Bazerbachi, F., Vargas, E. J., Sharaiha, R. Z., Thompson, C. C., Thaemert, B. C., Teixeira, A. F., Chapman, C. G., Kumbhari, V., Ujiki, M. B., Ahrens, J., Day, C., Acosta, A. J., Badurdeen, D., Buttar, N. S., Clark, M. M., Eaton, L., Ghanem, O., Grothe, K., … Wilson, E. B. (2022). Endoscopic sleeve gastroplasty for treatment of class 1 and 2 obesity (MERIT): a prospective, multicentre, randomised trial. Lancet (London, England), 400(10350), 441–451. https://doi.org/10.1016/S0140-6736(22)01280-6
Lahooti, A., Westerveld, D., Johnson, K., Aneke-Nash, C., Baig, M. U., Akagbosu, C., Hanscom, M., Buckholz, A., Newberry, C., Herr, A., Schwartz, R., Yeung, M., Sampath, K., Mahadev, S., Kumar, S., Carr-Locke, D., Aronne, L., Shukla, A., & Sharaiha, R. Z. (2025). Improvement in obesity-related comorbidities 5 years after endoscopic sleeve gastroplasty: a prospective cohort study. Gastrointestinal Endoscopy, 102(1), 26–36. https://doi.org/10.1016/J.GIE.2024.12.017
Singh, S., Hourneaux de Moura, D. T., Khan, A., Bilal, M., Ryan, M. B., & Thompson, C. C. (2019). Safety and Efficacy of Endoscopic Sleeve Gastroplasty Worldwide for Treatment of Obesity: A Systematic Review and Meta-analysis. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Bariatric Surgery, 16(2), 340. https://doi.org/10.1016/J.SOARD.2019.11.012
The Endoscopic Gastroplasty ESG – not to be confused with the Laparoscopic Sleeve Gastrectomy- was “endorsed” by the American Society for Metabolic and Bariatric Surgery (ASMBS) as an acceptable tool for treatment of obesity.
Patients need to understand that endoscopic gastroplasty ESG and sleeve gastrectomy LSG are not the same procedure and do not deliver the same outcome. Let’s not forget that we have seen this before with Fen Phen, Lap Band, Realize Band, Gastric balloon, GLP-1, and GIP, where low-risk, simple, and otherwise benign procedures and medications were found to be ineffective at best or to cause irreversible long-term complications at worst.
In EG, the stomach is folded, whereas in LSG, a significant portion of the stomach is removed.
The ASMBS, even in their press releas,e has highlighted:
(e.g., sleeve gastrectomy, gastric bypass) when it comes to expected weight loss or metabolic
impact, it does fall within a treatment continuum that includes lifestyle therapy, obesity
management medications (OMMs), and metabolic and bariatric surgery and should be available
to patients through bariatric and metabolic surgeons.
In my opinion, as supported by the published literature and the summary of the ASMBS position statement, endoscopic gastroplasty may be an appropriate procedure for some patients with the understanding that the weight loss is slower and less than that of the sleeve gastrectomy.
Endoscopic sleeve gastroplasty (ESG) differs from Laparoscopic sleeve gastrectomy (LSG).
ESG (Endoscopic Sleeve Gastroplasty) is promoted and advocated as a low-risk, equal alternative to the Laparoscopic Sleeve Gastrectomy, but it is not.
Anatomically speaking:
Endoscopic Sleeve Gastroplasty is an endoscopic procedure performed under general anesthesia. During this procedure, a specialized endoscope is inserted through the mouth into the stomach. Multiple plastic “H”-type anchors are used to create a fold in the stomach, thereby reducing its size. No part of the stomach is removed. Initial limited weight loss occurs as the patient feels full after consuming small volumes of food. This effect resembles what happens with the lap band and gastric balloon, and we know how the story ends with those.
LSG is performed laparoscopically with incisions on the abdomen under general anesthesia. Seventy-five to eighty-five percent of the stomach, along its greater curvature, is removed, eliminating the part of the stomach that produces the Ghrelin hormone, which controls and modulates hunger. This is why patients feel fuller with a smaller volume of food and experience significantly reduced hunger.
Results:
Please read the fine print
The summary results indicate
“Our results suggest that ESG is safe and effective for the treatment of obesity, with durable
long-term results for at least up to 5 years after the procedure. “
When you look at the details of the results, however, it states:
“At 5 years, mean TBWL was 15.9% (95% CI, 11.7-20.5, p < .001) and 90 and 61% of
patients maintained 5 and 10% TBWL, respectively.”
This means that five years after ESG, 90% of the patients have only lost 10% of their TBWL (total body weight loss), and 61% would have lost 10% of their TBW (Total Body Weight).
This serves as an illustration of how actual outcomes are obscured within the fine print, resulting in a lack of attention from individuals seeking the optimal outcome devoid of perceived risk. The same principle applies to the ongoing discourse regarding GLP-1 medications. The genuine risk associated with ESG and PLG-1 is that patients have undergone alterations to their anatomy and physiology without demonstrable results. Several years into contemplating a treatment promising sustained outcomes, we find that the alterations have increased the overall risk.
As a surgeon, I encourage people to always ask questions and demand that scientific proof be provided. I am not opposed to progress; considering the nature of our practice, we have witnessed and have unrgone significant evolution over the past 30 years, transitioning from performing open cases necessitating a hospitalization period of 4 to 6 days to performing the same cases laparoscopically and robotically in some cases outpatient procedures.
Imaging technology has evolved dramatically since Dr. Roentgen’s first X-ray was taken in December 1895. Our understanding of the science of radiation has changed exponentially. However, there is significant evidence that overutilizing radiation-related diagnostic studies is unnecessary. Several factors, including medico-legal and financial concerns, likely drive this.
There is a new publication that has documented the increased risk of cancer associated with excessive radiation caused by diagnostic testing.
We should all ask the question before ordering and submitting to a diagnostic examination that involves radiation:
What information am I trying to get?
Have I had a similar test done? And if so, do I have access to the records and images?
This is why I always recommend that patients maintain the report, the images, and all the radiologic studies they get done so they are readily available to them and their healthcare providers. This helps to reduce the amount of imaging radiation a patient may be exposed to.
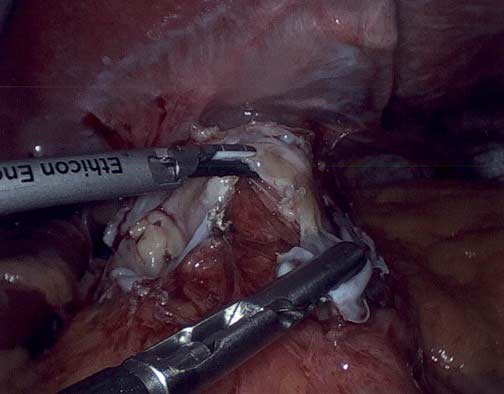
The gastrointestinal staplers simultaneously pass six rows of staples and cut in between them to create two secure lines of staples, three rows on each side. The staples come in different thicknesses and lengths for various applications. Staple cartridges that are used for colon surgery are usually thicker tissue staples than those that are used for small bowel stapling.
Different manufacturers have different color coding.
Another question I frequently get asked is, How does a stapler staple and cut at the same time? The stapler needs to be thick enough to not tear through the tissue and provide uniform pressure for control of bleeding and prevent leaks. It can not be too large either.
When stapling on the stomach for sleeve gastrectomy, the stomach wall thickness is different. We use different-sized staples to accommodate the thicker part of the lower stomach toward the thinner part of the stomach where it meets the esophagus.
Stapler and resulting discharged lines of staples.
Patients are frequently asked to explain why they take high fat- or water-soluble vitamin doses. They are have often been scared by their well meaning healthcare providers that their higher levels of vitamin supplements will end up with vitamin toxicity.
Let’s clarify one point: there is such a thing as too much vitamin.
However, the point that is often overlooked in teaching within professional schools (medical, nursing, pharmacy, etc.) and drug manufacturers is that recommendations are based on “how much to take” and not how much is needed to keep a patient’s blood level in the normal range.
This table highlights how toxicity is described and what requirements are recommended. Vitamin toxicity is seen rarely in post-weight loss surgical patients who take them proactively in as many doses as needed to get their blood levels in the normal range. I see more patients in the office who suffer from low vitamin levels, such as vitamin D and A levels (duodenal switch and sleeve), than any patient with high or toxic levels of any vitamins.
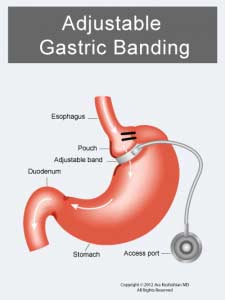
The Lap Band was approved in the US in 2001 (BMI> 40). The following studies used only small samples and examined short-term efficacy and safety. They were then performed to consider the utility of the Laob band for patients with lower BMI (BMI 30-40).
Noe the frequent complications of nausea, difficulty swallowing, pain, and reflux-which may sound familiar to a lot of patients who have had and still have the Lap Band.
Numerous US and international studies have been published over the years, including short-term and long-term studies. The summary outcome has been the same, with only a few exceptions.
The Lap Band does not result in long-term sustained weight loss.
Lap band has significant complications, some of which may not be reversible.
The lap band can be removed, but eroding the banc to the stomach is not easy.
Let’s ask the question: why would the slogan of a product be that “it’s easily reversible”? Under what circumstances would anyone want the life-saving device to be removed for the original condition (obesity) return? The answer is when the complications are worse than the condition itself.
Adjustable Gastric Band Easily Reversible?
Removing the band is not easy, and extensive dissection is often needed to remove the capture (scar tissue) that forms around the band.
My recommendation is: With much better and safer alternative surgical procedures available (Sleeve Gastrectomy) (Duodenal Switch), no one should get the LAp Band placed. For those of you who have it, take it out as soon as possible before it becomes an emergency while causing irreversible dilation of the esophagus