Endoscopic sleeve gastroplasty (ESG) differs from Laparoscopic sleeve gastrectomy (LSG).
ESG (Endoscopic Sleeve Gastroplasty) is promoted and advocated as a low-risk, equal alternative to the Laparoscopic Sleeve Gastrectomy, but it is not.
Anatomically speaking:
Endoscopic Sleeve Gastroplasty is an endoscopic procedure performed under general anesthesia. During this procedure, a specialized endoscope is inserted through the mouth into the stomach. Multiple plastic “H”-type anchors are used to create a fold in the stomach, thereby reducing its size. No part of the stomach is removed. Initial limited weight loss occurs as the patient feels full after consuming small volumes of food. This effect resembles what happens with the lap band and gastric balloon, and we know how the story ends with those.
LSG is performed laparoscopically with incisions on the abdomen under general anesthesia. Seventy-five to eighty-five percent of the stomach, along its greater curvature, is removed, eliminating the part of the stomach that produces the Ghrelin hormone, which controls and modulates hunger. This is why patients feel fuller with a smaller volume of food and experience significantly reduced hunger.
Results:
Please read the fine print
The summary results indicate
“Our results suggest that ESG is safe and effective for the treatment of obesity, with durable
long-term results for at least up to 5 years after the procedure. “
When you look at the details of the results, however, it states:
“At 5 years, mean TBWL was 15.9% (95% CI, 11.7-20.5, p < .001) and 90 and 61% of
patients maintained 5 and 10% TBWL, respectively.”
This means that five years after ESG, 90% of the patients have only lost 10% of their TBWL (total body weight loss), and 61% would have lost 10% of their TBW (Total Body Weight).
This serves as an illustration of how actual outcomes are obscured within the fine print, resulting in a lack of attention from individuals seeking the optimal outcome devoid of perceived risk. The same principle applies to the ongoing discourse regarding GLP-1 medications. The genuine risk associated with ESG and PLG-1 is that patients have undergone alterations to their anatomy and physiology without demonstrable results. Several years into contemplating a treatment promising sustained outcomes, we find that the alterations have increased the overall risk.
As a surgeon, I encourage people to always ask questions and demand that scientific proof be provided. I am not opposed to progress; considering the nature of our practice, we have witnessed and have unrgone significant evolution over the past 30 years, transitioning from performing open cases necessitating a hospitalization period of 4 to 6 days to performing the same cases laparoscopically and robotically in some cases outpatient procedures.
We, as humans, can consume three energy sources: carbohydrates (glucose), fat (fatty acids), and protein (amino acids). They are all needed for optimal body function. Protein (amino acids) and protein metabolism are critical to the human body’s structure (muscles) and function (immune system). However, there is a possibility of “too much protein“. All forms of nutrients are eventually converted to fat for storage. So when patients focus on a protein-rich diet and consume protein supplement drinks without accounting for the calories, they may slow or stop the weight loss and, in some cases, even gain weight after weight loss surgery. Before everyone gets alarmed and stops eating protein, I am only trying to raise awareness to keep an inventory of the protein intake, not only a measure of the protein but also the caloric intake.
The images below depict different states of metabolism and protein metabolism. Please note that in the image below (in a feasting state), all consumed protein leads to fat storage if not used as a building block of protein (amino acids). This is why too much protein can cause weight gain if not used to build muscle.
The key is to manage the delicate balance of taking adequate protein against what is needed to maintain healthy muscle mass and immune function. The image below shows what happens when patients do not consume sufficient protein over long periods. The body starts breaking down the muscles and converts this all to energy. In this diagram, body proteins are the muscle mass broken down into amino acids to supply the body with needed glucose and ketones to give the body energy for its functions.
Hello
Weight loss surgical results are dependent on several variables. These include patient-specific conditions as well as the type of surgery. The primary objective of this study is to evaluate if there is any value in the specific pre-operative workup mandated by health insurance plans and the long-term outcome of the weight loss surgical procedures. The secondary result of the study is to compare the surgical outcomes of the different weight loss procedures.
We hope you can spare a few minutes to complete the survey if you have received it. If you have not seen the study, please check your spam junk folder for an email that contains the link from our office.
We wish you a happy and healthy holiday season.
Date-entry instruction Video
Obesity is related to as many as 400,000 deaths each year in the US and it has increasingly been recognized as a risk factor for several nutrient deficiencies. This may seem surprising given the likelihood of over consumption of calories, however these additional calories are not from nutritious sources. One of the main reason for these nutritional deficits is the greater availability of inexpensive foods that are rich in calories and are nutrient deficient. This has led some medical professional to conclude that there is a certain group of people who are overfed but undernourished. Even with the epidemic of the obesity, there is significant nutritional deficiencies noted.
Obese subjects have increased blood volume, cardiac output, adiposity, lean mass and organ size all of which can influence volume of distribution, in addition, treatment for severe obesity involving surgical procedures can worsen these nutrient deficiencies and in some cases may cause new ones to develop.
This table shows the percentage of population below the estimated average requirement (EAR) by body weight status in adults more tan 19 years old, showing that almost 90 to 100 percent of people including normal weight (NW) are below the EAR of vitamin D and Vitamin E.
Nutritional deficiencies in obese patients may promote the development of chronic diseases including increased insulin resistance, pancreatic B-cell disfunction and diabetes, this is because specific micronutrients are involved in glucose metabolic pathways; There are other chronic diseases related to obesity that are being investigated such as decrease in focal grey matter volume and cognitive impairment or inadequate sleep due to low intake of antioxidant vitamins.
We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
Sleeve gastrectomy has become the most frequently performed operation in the US. Sleeve as a part of the Duodenal Switch or as a stand alone operation has been offered in our practice for nearly 20 years. As a precondition to this, patients’ choosing to have the sleeve, especially with high BMI (>45) and those with metabolic conditions (diabetes, high cholesterol or triglycerides, PCOS, and others) we have always recommended Duodenal Switch as the procedure of choice instead of the Sleeve Gastrectomy due to improved and lasting co-morbid resolution and weight loss maintenance with Duodenal Switch. It has been know for years that a sizable number of patients having the sleeve will experience weight regain requiring conversion to the duodenal switch or the RNY Gastric Bypass. Majority of the patients having gained weight after sleeve, or experiencing the return of co-morbidities after a transient resolution during the their weight loss phase, should only be revised to the Duodenal switch operation in my opinion. The alternative procedures of SIPS and SADI or similar single anastomosis operation with confusing nomenclature should be avoided, since as of the publication of this blog they are still considered investigational by the American Society for Metabolic and Bariatric Surgery (ASMBS) with no long term data.
The only plausible reason for revision of the Sleeve to the gastric bypass (RNY) would be those patients who are experiencing reflux.
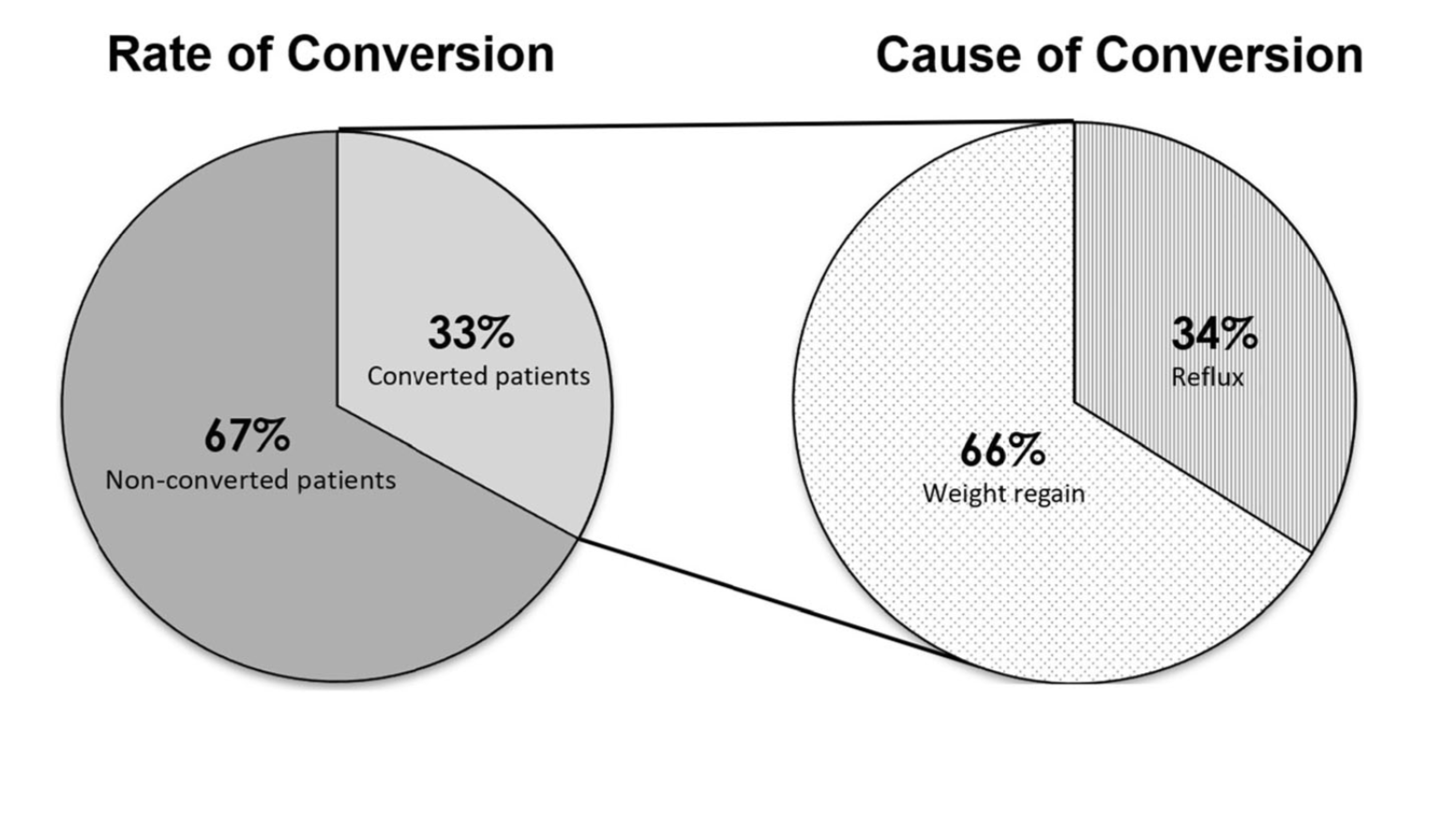
Felsernreich et.al. demonstrated that 10 years after sleeve gastrectomy33% were requiring revisions of their sleeve due to weight regain or reflux. 66% needed revision for weight loss and only 34% for reflux. Those patients who have revision to gastric bypass (in their practice all being revised with two exception) had resolution of their reflux however had no sustained weight loss after the revisions. This supports our position that we have had for years that the those patient who had the sleeve and are experiencing weight regain, recurrence of comorbidities inadequate weight loss ahould all be revised to the duodenal switch operation.
Gastroesophageal (GE) reflux is the condition when the stomach contents are able to “reflux” back through an incompetent lower esophageal sphincter (LES) into the esophagus.
Gastroesophageal reflux Disease (GERD) is a clinical condition caused by long-standing reflux that results in microscopic and visible changes to the inner lining of the esophagus and esophageal mucosa.
GERD is nondescript as to the cause of the condition. It only states that the stomach contents have been irritating the lining of the esophagus on a chronic basis. This can be caused by an anatomical abnormality of the GE junction (hiatal hernia) or may be related to dysfunction of the LES. Other possible causes of GERD may be infection (H. Pylori), environmental (stress), and dietary (nicotine, alcohol, caffeine, spicy food) in origin.
So far, we have not clarified the chemical nature of the refluxed content.
In Acid Reflux, the relative acid overproduction of acidic secretion and the exposure of the esophageal mucosa need to be addressed. This is accomplished by acid suppression medications, anti-histamine (H2 blockers), and Proton pump inhibitors (PPIs). The physiology and the mechanism involving this condition are well understood. As a surgeon, however, I do see patients who should have had surgical intervention. The initial mode of therapy for a patient with documented acid reflux and or symptomatic hiatal hernia is placing them on medication. These patients are then recommended to have a related upper endoscopy. Patients who do not improve or where deterioration of the esophageal mucosa and the presence of precancerous cells are referred for surgical intervention.
Bile Reflux, contrary to acid reflux, may have tiny, if anything, to do with the LES. The symptoms experienced by the patient may be as after related to the excessive bile in the stomach, which is seen frequently
The treatment of Bile reflux is Duodenal Switch without the associated sleeve gastrectomy component in addition to repair of hiatal hernia if present. Ann Surg. 2007 Feb; 245(2): 247–253.
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
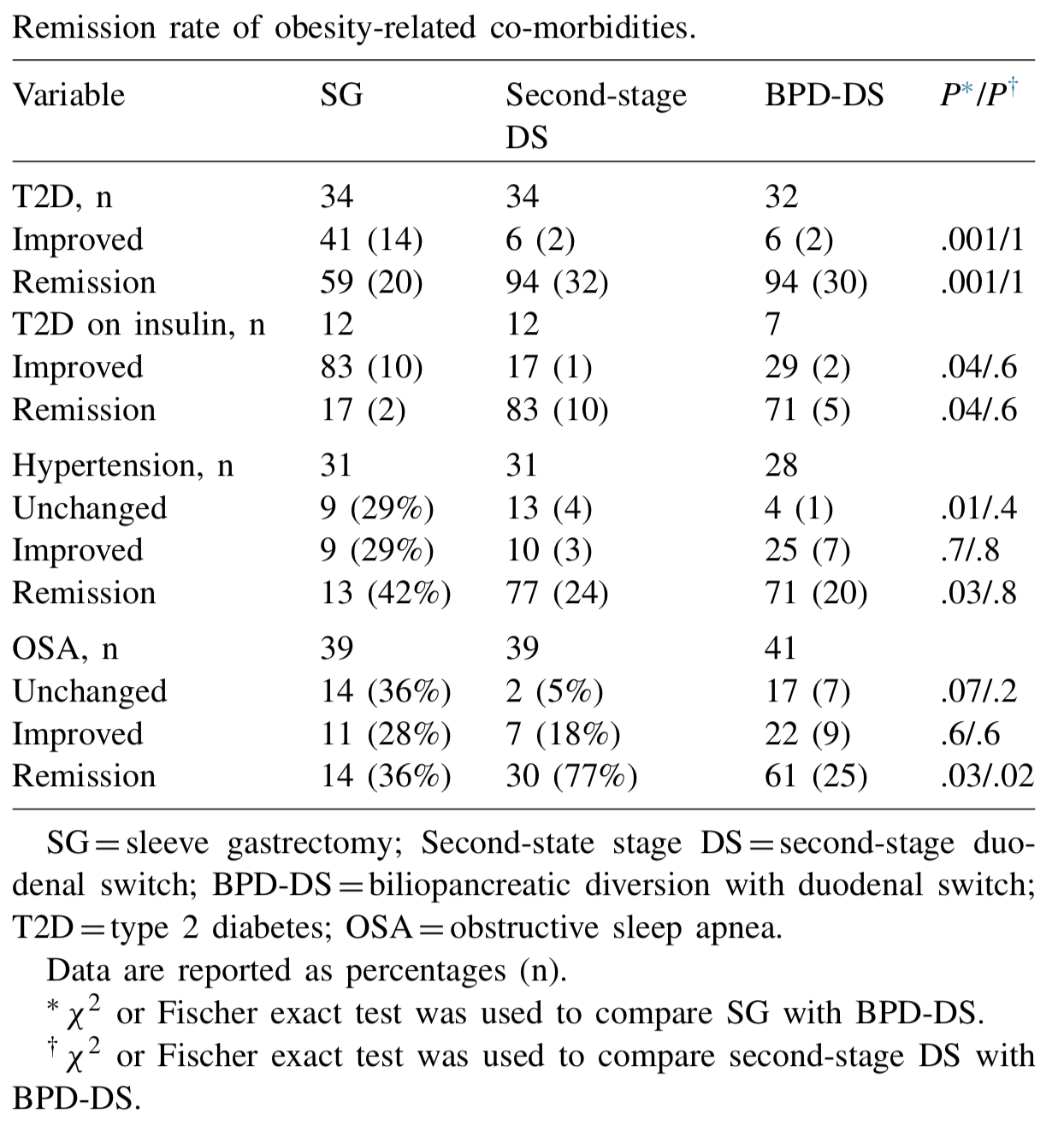
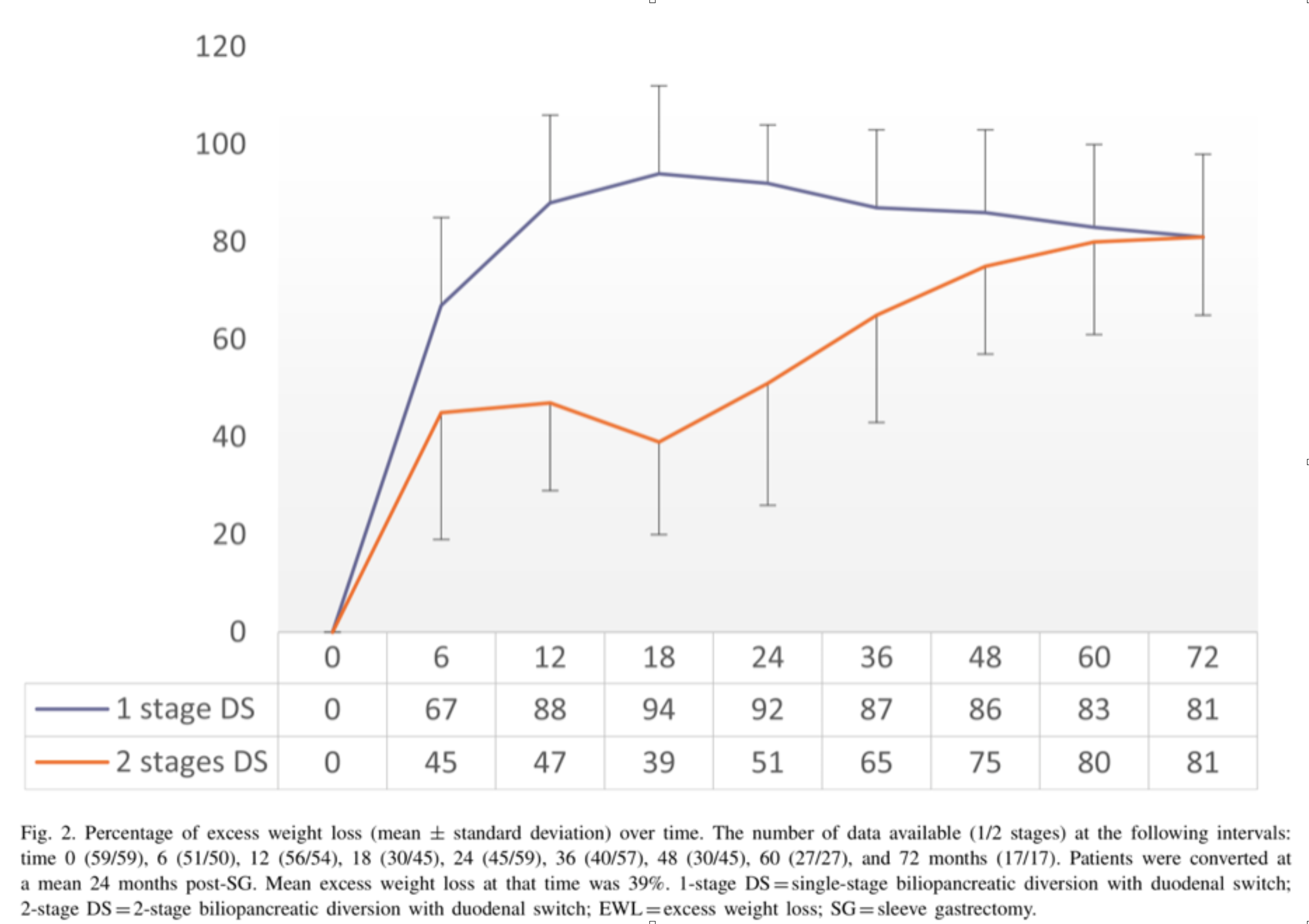
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss.
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.
Here we go again…. There is a new cure for obesity, Gastric Balloon, with minimal to no risk, is an outpatient procedure and/or can be done in the surgeons office with no anesthesia. Have we not similar claimed like this before (Adjustable gastric band) ?
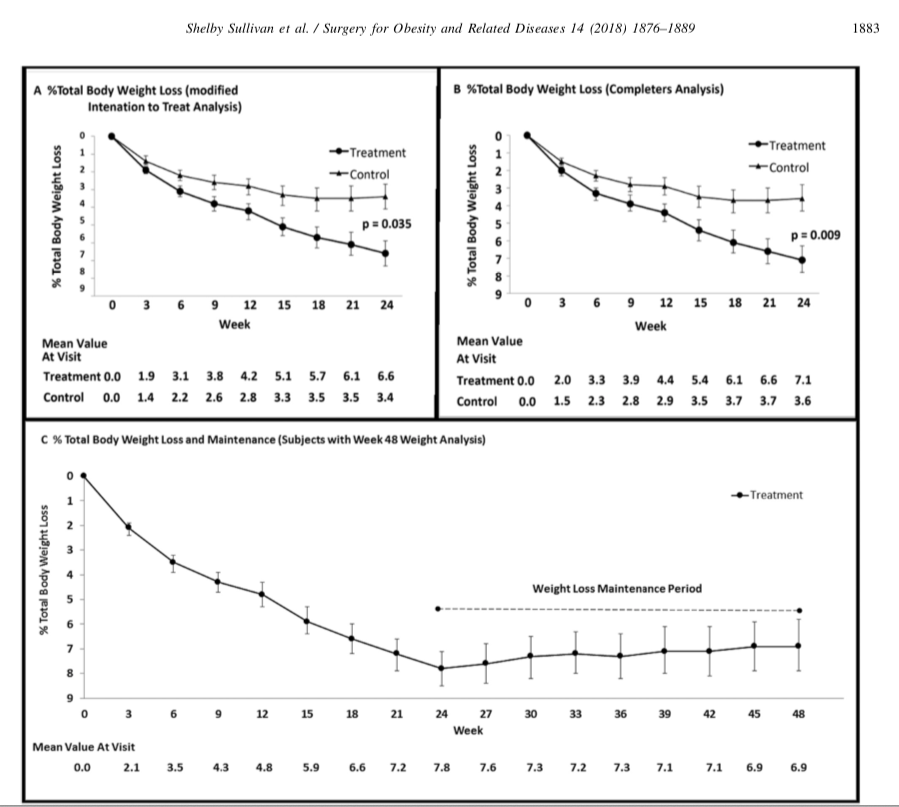
Randomized sham-controlled trial of the 6-month swallowable gas-filled intragastric balloon system for weight loss published in Surgery for Obesity and Related Diseases 14 (2018) 1876–1889, by Sullivan et. al reports
“Conclusions: Treatment with lifestyle therapy and the 6-month swallowable gas-filled intragastric balloon system was safe and resulted in twice as much weight loss compared with a sham control, with high weight loss maintenance at 48 weeks.”
This sound very promising, however is very vague and leaves out significant, critical, and pertinent information.
The outcome of weight loss at 24 weeks was reported in Total Body weight loss % (TBWL%), Excess weight % (EWL), weight loss, and BMI change. Of those, the last three were statistically significant changes.
The outcome the weight loss was reported to be at 7% TBWL% at 24 weeks with some weight regain, with the patient employing post REMOVAL life style changes.
It is stated that the Gastric Balloon is temporary device that needs to be removed in 6 months and should be considered in low BMI patients (<35kg/m2). It is is important for those patients who are considering this temporary expensive measure for minimal weight loss to entertain the alternative of the same temporary results that may be obtained by lifestyle changes. These results may be maintained by a healthy lifestyle, exercise, and eating without the need for a device.
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.
Poly Cystic Ovarian Syndrome
Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
Whenever you are dealing with insurance issues it is important to have a general understanding of insurance ins and outs. The Obesity Action Coalition has a good general guide to the insurance process here. If you are having issues with out of network, out of area, or insurance appeals and denials for Duodenal Switch, there may be some additional assistance from two individuals who have had the Duodenal Switch procedure themselves. We are grateful that they have provided assistance throughout the years to the Duodenal Switch community. The following is their statement on insurance.
The majority of insurance companies are in the business of making money (for profit). They can deny requests for preauthorization with impunity. These denials are often complexly worded and difficult to comply with and overcome, and are definitely overwhelming to the patient, and the busy surgeon’s office. The vast majority of patients faced with demanding if not impossible to achieve prerequisites, or denial of the request for preauthorization simply give up, and the insurance companies pocket the savings.
If you find yourself facing impossible pre-op hurdles, or a denial, we urge you to appeal, and to seek assistance in preparing the appeal. You can hire an attorney, of course, but there is an informal and free resource we suggest that you investigate as well.
If you go to BariatricFacts.org (a non-profit, patient-run site), you will find individuals who are long-term DS postops, and patient advocates. They have been helping patients, pro bono (for free), for over 10 years. They will help you draft your appeal letters, provide supporting medical and legal documentation, and prepare draft letters of medical necessity to be reviewed and signed by your surgeon supporting your appeal. They will not represent you directly, but they will help you best represent yourself. in many cases it is necessary to exhaust all internal appeals (because the insurance companies are unlikely to overrule themselves), and then file for external review, where independent reviewers often overrule improper denials. If you join and then post on BariatricFacts.org asking for help, you will be connected with them and you can decide if you want their help.
Please note that this is just a suggestion. It is neither legal nor medical advice, nor a guaranty regarding their services, and you should always consider getting legal advice and assistance from an attorney who will represent you directly. The members at BariatricsFacts.org will help you draft your own letters, but will not be your legal or medical representatives; you will be required to do a fair amount of your own work on your appeals, and to sign them yourself.
It is suggested that before or at the same time as you contact the resources suggested at the site, you gather as much of the following information as you can:
A copy of your Evidence of Coverage, which is the usually 100+ page insurance contract between your employer and the insurance company, which you can obtain it from your HR department. If you are self-insured, it will be available directly from your insurance company. Note: it is NOT the Summary of Benefits – it needs to be the contract itself.
If your insurance is through an employer, you need to determine whether your plan is self-funded or fully-funded. Your rights are significantly different under the two types of plans.
If your insurance company has a separate bariatric surgery policy, provide a copy of that, too.
A copy of your surgeon’s request for preauthorization, which provides the ICD-10 and CPT codes submitted.
A copy of your denial letter, including the section regarding your appeal rights.
* It is strongly recommended that you obtain a copy of your surgeon’s LOMN (letter of medical necessity) before it is submitted to your insurer or for external review, so we can assist your busy surgeon in making the strongest possible case for you.
Don’t be deterred by a denial. It is unfortunately more common than it should be, but it can often be overcome if you meet the requirements for bariatric surgery, if you get help navigating the process.