Category: BPD
Vitamin D level and Liver Function Test (LFT) elevation
February 08, 2026 11:21 am
After weight-loss surgery, some patients may experience a transient elevation in liver function tests that resolves over time. We have previously reported on this. IT is essential to distinguish between the Duodenal switch and the SIPS/SADI procedure, where some patients are led to believe they are identical. These procedures differ physiologically, and their weight loss and metabolic behaviours vary significantly.
Other than the stress of the weight loss, obesity, and comorbidities of obesity, there may be other anatomical post-surgical causes for elevated liver function test. This has also been discussed extensively.
A recent literature review supports the protective effects of vitamin D supplementation.
Elevated liver enzymes may be caused by many factors, including nutritional deficiencies, excessive supplementation (turmeric), medications, alcohol, adhesions causing partial bowel obstruction, and increased enterohepatic bile reabsorption . I would be very cautious about associating vitamin D supplementation with elevated liver function test results, even if the vitamin D level is in the very high normal range, regardless of the daily dose (much less frequent with injectable).
Vitamin D, as a fat-soluble vitamin, however, protects the liver and improves liver function test even in very high serum level . In rare cases, prolonged, elevated vitamin D levels may strain the liver. In Fact, the association of the vitamin D level and liver disease, including cirrhosis, leads to hepatocellular carcinoma (HCC) and dea h. Vitamin D protects the liver from HCC but cannot reduce the risk of cirrhosis.
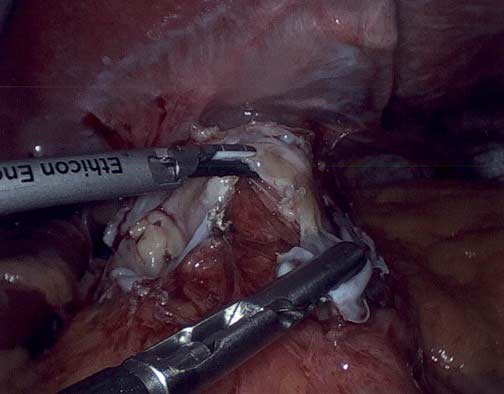
How does a stapler staple and cut at the same time
February 11, 2025 12:27 pm
The gastrointestinal staplers simultaneously pass six rows of staples and cut in between them to create two secure lines of staples, three rows on each side. The staples come in different thicknesses and lengths for various applications. Staple cartridges that are used for colon surgery are usually thicker tissue staples than those that are used for small bowel stapling.
Different manufacturers have different color coding.

Another question I frequently get asked is, How does a stapler staple and cut at the same time? The stapler needs to be thick enough to not tear through the tissue and provide uniform pressure for control of bleeding and prevent leaks. It can not be too large either.
When stapling on the stomach for sleeve gastrectomy, the stomach wall thickness is different. We use different-sized staples to accommodate the thicker part of the lower stomach toward the thinner part of the stomach where it meets the esophagus.


Video of stapler demonstration
Feeding Tube with Duodenal Switch
February 03, 2025 9:53 am
The surgical changes following the revision of the failed gastric bypass to the duodenal switch or a primary duodenal switch require an evident appreciation and understanding of the anatomy and physiology of placing a feeding tube and managing the nutritional status. There are different places where a feeding tube can be placed.
1-A feeding gastrostomy tube endoscopically cannot be placed because of the transected post-pyloric duodenum (The image viewed on a desktop or a laptop allows the scroller on the image to move)
2-An orogastric or nasogastric tube should only use an elemental feeding formula. This is because the food in the stomach is prevented from mixing with the biliopancreatic juices, which will not be adequately absorbed.
3-A feeding Jejunostomy can only be insured surgical post ligament of traits. This cannot be done endoscopically because duodenal switch transaction post pyloric small bowel to prevent mixing of the biliopancreatic secretion.
Additional informationShould Adjustable Gastric Banding (Lap Band) be done?
October 06, 2024 9:17 pm
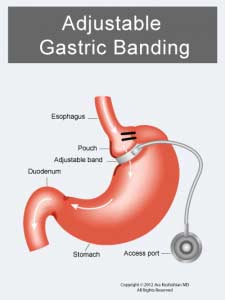

- The Lap Band does not result in long-term sustained weight loss.
- Lap band has significant complications, some of which may not be reversible.
- The lap band can be removed, but eroding the banc to the stomach is not easy.

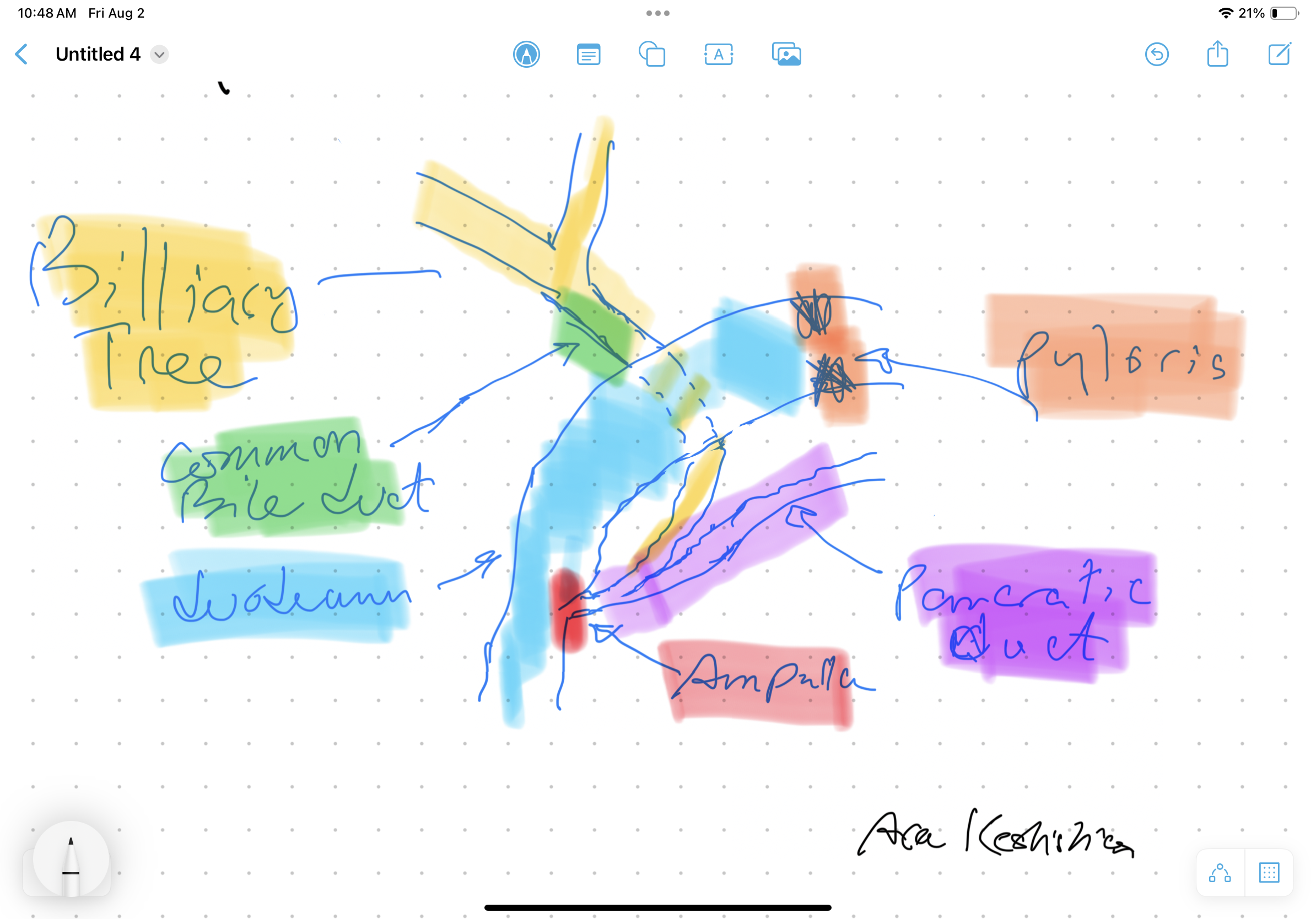
Bile Reflux Gastritis
August 02, 2024 10:53 am
Bile Reflux
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary tract flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or a tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis is reserved for cases with no alternatives.

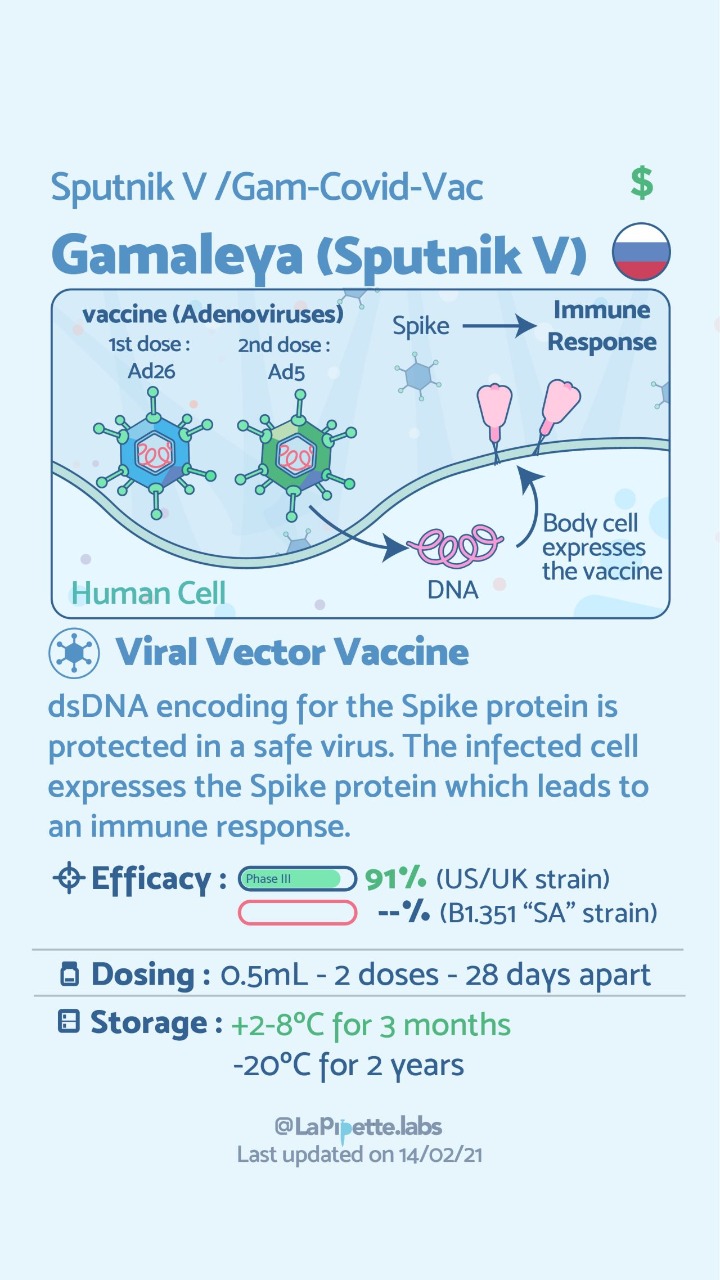
COVID Vaccines
March 05, 2021 3:50 pm
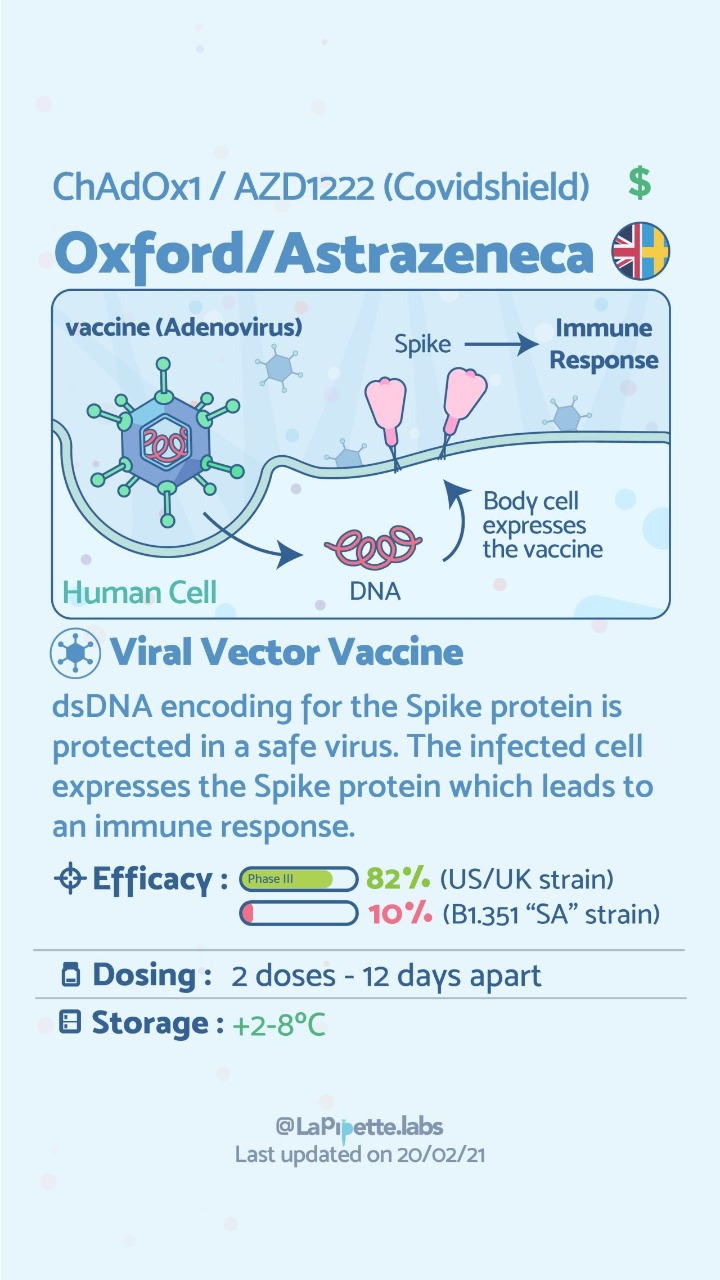
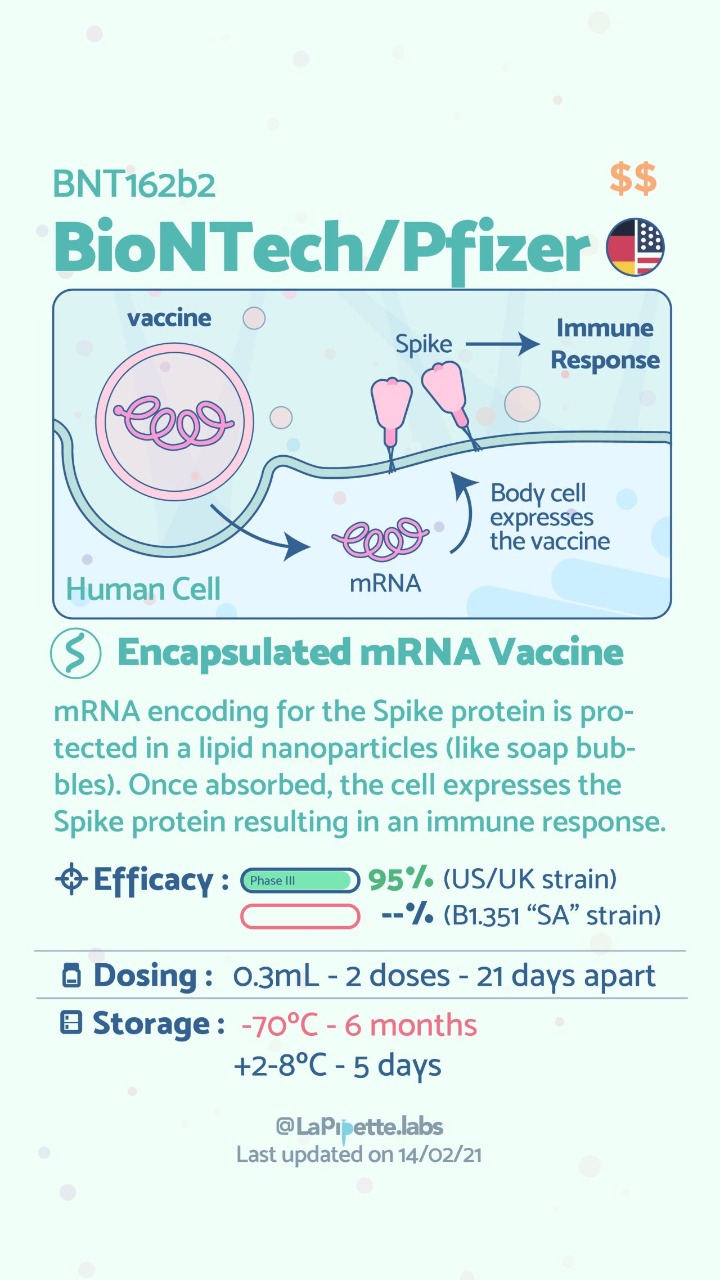
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
Vitamin D and Covid -19
May 07, 2020 9:24 am
We are all aware of the many roles that Vitamin D plays in our bodies. This includes immune function in addition to all the regulatory roles that Vitamin D plays in several physiologic reactions. There may be a correlation of low Vitamin D and COVID-19 infection increasing death risk as looked at in research articles.
Covid -19 in a subset of patience causes significant lung injury. These patients require mechanical ventilation.
Previously reported publications have suggested a possible correlation between ace inhibitors and increased risk of pulmonary complications of Covid -19. Some researchers suspect that the Covid-19 may be able to enter lung cells by the ACE receptors.
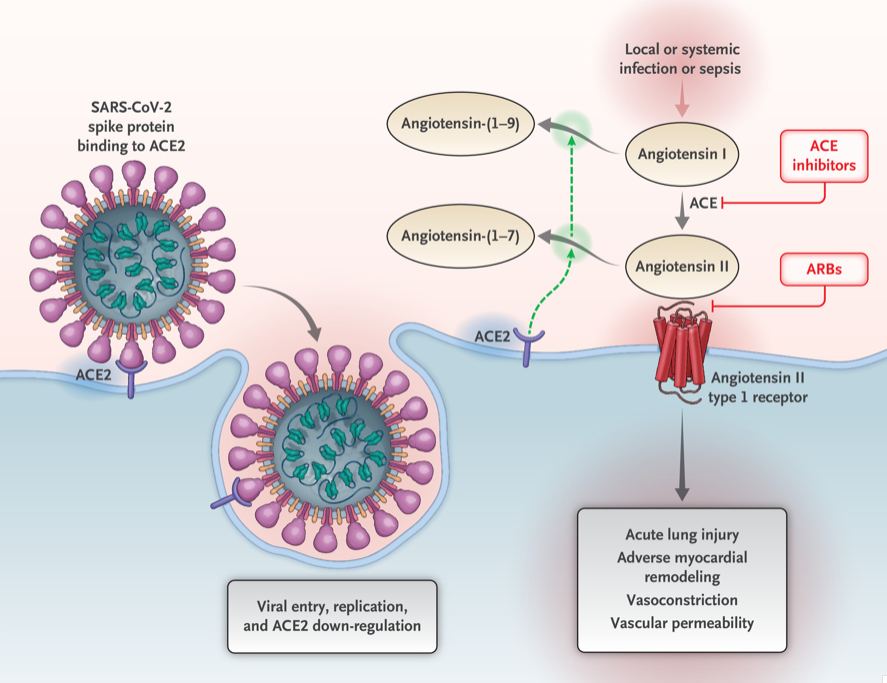
Vitamin D may positively implact the receptor ACE2. This study, report clear correlation between the high death rate with low vitamin D levels in Covid infected patients. There are limitation to this study that the attached abstract outlines.
Our take home message would be to please make sure you have updated labs and that you are all taking the recommended Vitamin D based on your surgical anatomy and laboratory values, not just an average non-bariatric person recommended dose.
https://www.dssurgery.com/wp-content/uploads/2020/05/manuscript.pdf
Diabetes and Weight Loss Surgery
April 06, 2020 5:51 am
The scientific literature is riddled with evidence pointing to the benefit of early metabolic surgery as a superior treatment, remission and possible cure option for diabetes. Unfortunately, the medical education, pharmaceutical companies, primary care healthcare delivery systems and third party payers (health insurance companies) have not caught up with the published data. The American Diabetes Association has changed their guidelines to reflected the benefit for combating diabetes with weight loss surgery.
There is ample evidence of the superior outcome of surgery as a treatment option for diabetes when compared to medical managment. Cummings et.al, in a published article in Diabetes Care, showed sustained stabilization of the Hemoglobin A1C six years after surgery. In contrast, there was no significant changes noted in the non-surgical group.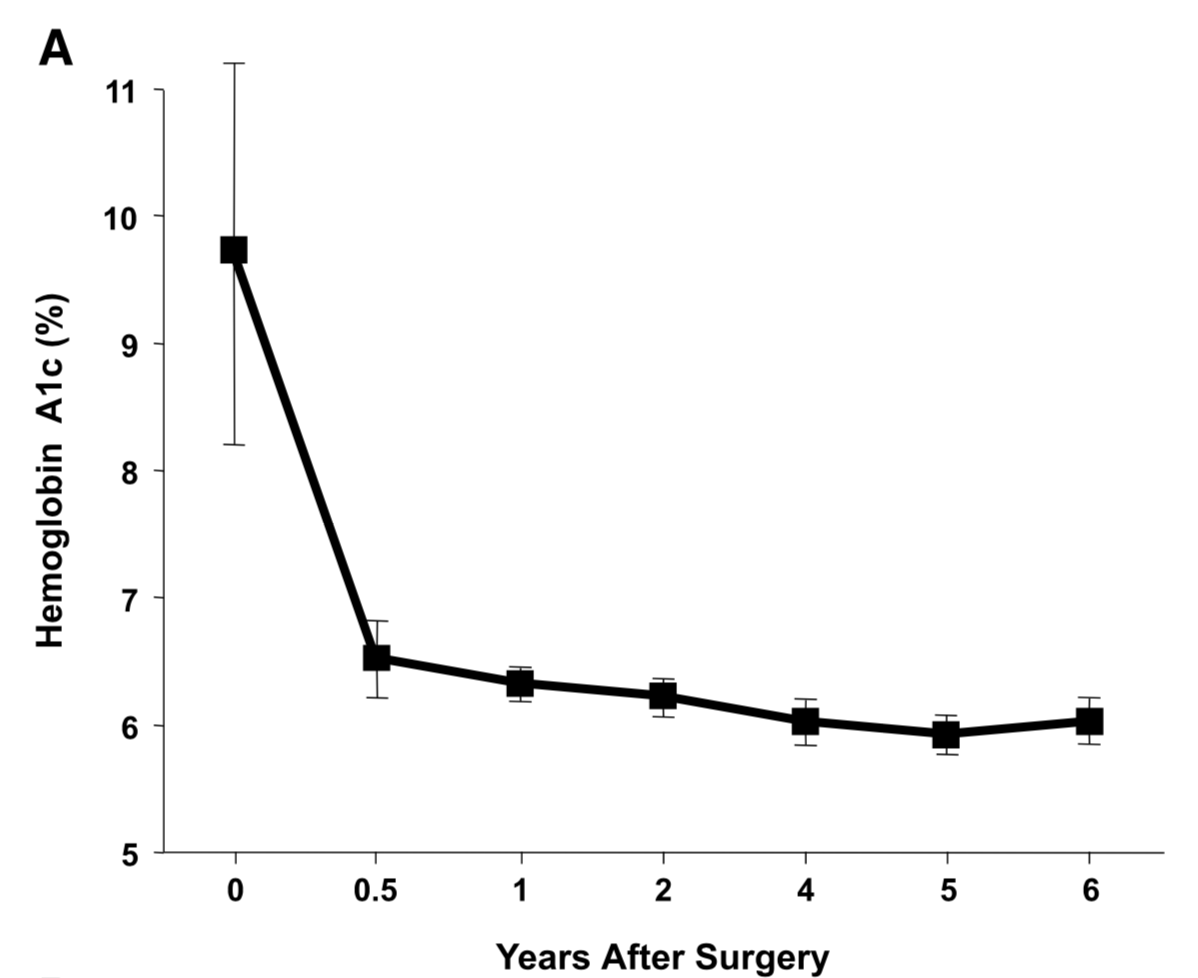
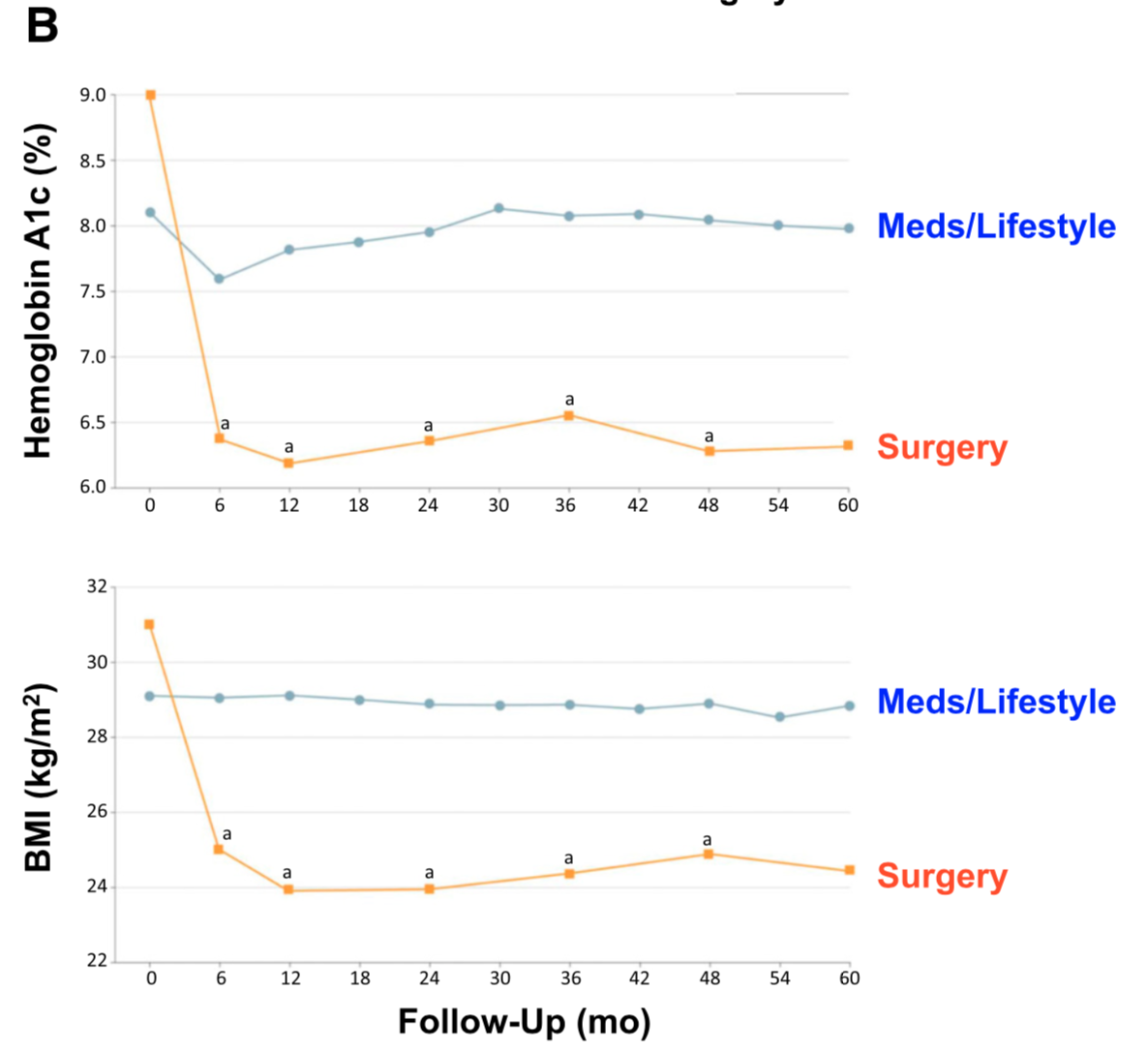
Jans et.al. , in November of 2019 showed that the patients who had NOT been on Insulin, and had metabolic surgery had the highest long term success for resolution and remission of the diabetes. This identifies that having a patient be proactive in their care by having metabolic surgery improves success rates.
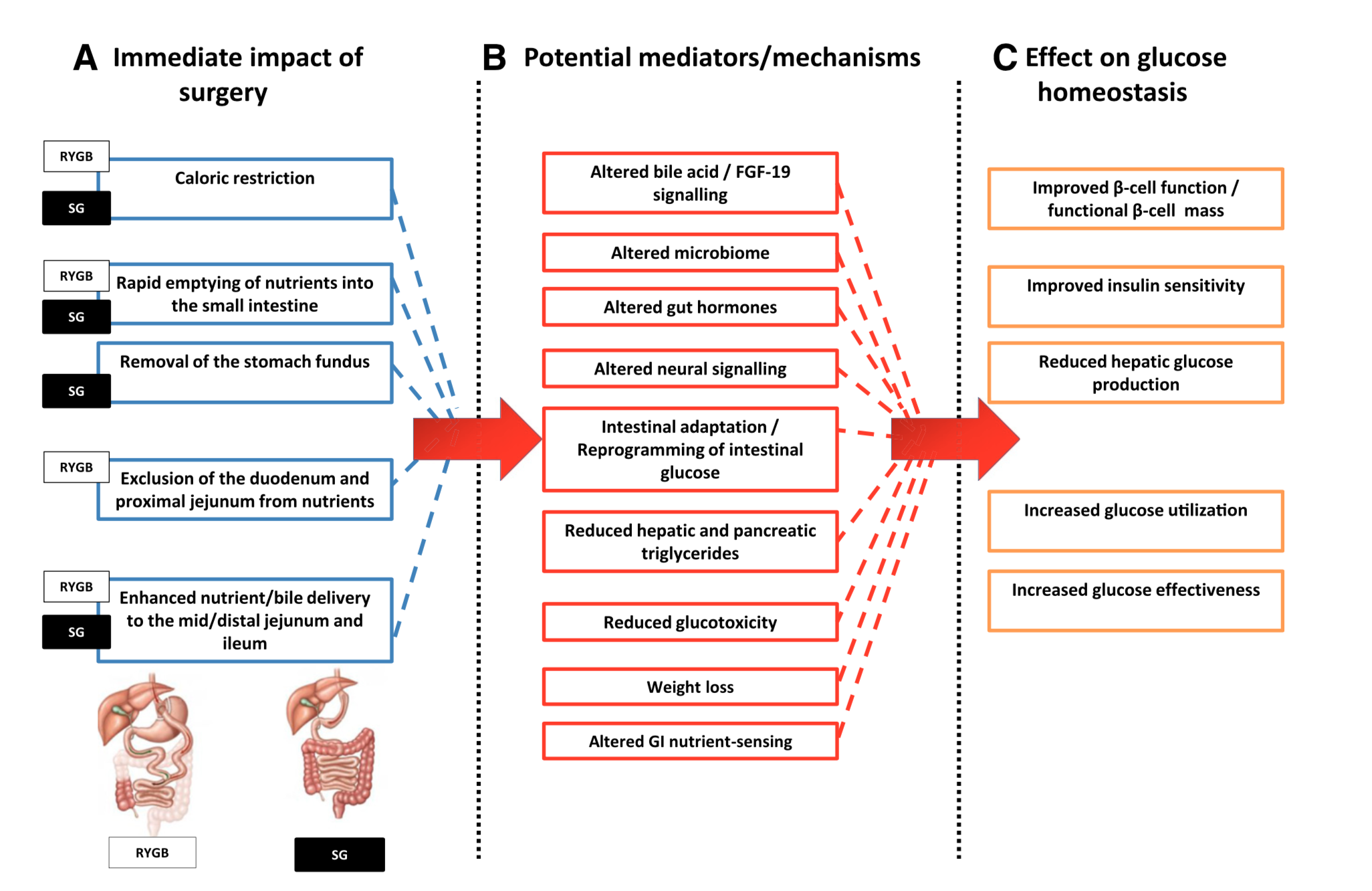
The exact mechanism by which the diabetes is resolved is unclear. The weight loss may play a role. There are numerous hormones and neuroendocrine modulators which control the complex metabolic pathways. Batterham et.al., in Diabetes Care (2016), published a summary overview of the possible mechanism involved in diabetes improvement following metabolic surgery.

There are a number of overlapping and sequential layers for possible reasons why diabetes resolves after weight loss/metabolic surgery. These may be directly related to surgery and the reduction of the calorie intake or absorption. It may also involve the neuroendocrine modulators.
What can be said definitively is that early surgical intervention is best and most likely the only permanent solution to type II diabetic resolution. There is no medical justification in not considering metabolic surgery in diabetic patients who may also have difficulty with meaning a BMI< 35.
Vitamin D Metabolism and Deficiency file
March 28, 2020 8:17 am
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
In some cases, patients may need injectable Vitamin A or D to improve vitamin levels.
Click the links to view the information below and within the comments of this file:
Vitamin D3 50 by Biotech: Amazon
directly from BioTech:
Many DS surgeon’s do not recommend Children’s vitamins or chewable vitamins unless there is a specific reason or need for them.
DS Surgeon Blog on Vitamin D:
Webinar on Vitamin D metabolism:
Medications that effect Bone health:
This does not constitute medical advice, diagnosis or prescribing. It is simply a compiled list of gathered information. If you are in doubt or have questions please contact your medical healthcare professional.