After weight-loss surgery, some patients may experience a transient elevation in liver function tests that resolves over time. We have previously reported on this. IT is essential to distinguish between the Duodenal switch and the SIPS/SADI procedure, where some patients are led to believe they are identical. These procedures differ physiologically, and their weight loss and metabolic behaviours vary significantly.
Other than the stress of the weight loss, obesity, and comorbidities of obesity, there may be other anatomical post-surgical causes for elevated liver function test. This has also been discussed extensively.
A recent literature review supports the protective effects of vitamin D supplementation.
Elevated liver enzymes may be caused by many factors, including nutritional deficiencies, excessive supplementation (turmeric), medications, alcohol, adhesions causing partial bowel obstruction, and increased enterohepatic bile reabsorption . I would be very cautious about associating vitamin D supplementation with elevated liver function test results, even if the vitamin D level is in the very high normal range, regardless of the daily dose (much less frequent with injectable).
Endoscopic sleeve gastroplasty (ESG) differs from Laparoscopic sleeve gastrectomy (LSG).
ESG (Endoscopic Sleeve Gastroplasty) is promoted and advocated as a low-risk, equal alternative to the Laparoscopic Sleeve Gastrectomy, but it is not.
Anatomically speaking:
Endoscopic Sleeve Gastroplasty is an endoscopic procedure performed under general anesthesia. During this procedure, a specialized endoscope is inserted through the mouth into the stomach. Multiple plastic “H”-type anchors are used to create a fold in the stomach, thereby reducing its size. No part of the stomach is removed. Initial limited weight loss occurs as the patient feels full after consuming small volumes of food. This effect resembles what happens with the lap band and gastric balloon, and we know how the story ends with those.
LSG is performed laparoscopically with incisions on the abdomen under general anesthesia. Seventy-five to eighty-five percent of the stomach, along its greater curvature, is removed, eliminating the part of the stomach that produces the Ghrelin hormone, which controls and modulates hunger. This is why patients feel fuller with a smaller volume of food and experience significantly reduced hunger.
Results:
Please read the fine print
The summary results indicate
“Our results suggest that ESG is safe and effective for the treatment of obesity, with durable
long-term results for at least up to 5 years after the procedure. “
When you look at the details of the results, however, it states:
“At 5 years, mean TBWL was 15.9% (95% CI, 11.7-20.5, p < .001) and 90 and 61% of
patients maintained 5 and 10% TBWL, respectively.”
This means that five years after ESG, 90% of the patients have only lost 10% of their TBWL (total body weight loss), and 61% would have lost 10% of their TBW (Total Body Weight).
This serves as an illustration of how actual outcomes are obscured within the fine print, resulting in a lack of attention from individuals seeking the optimal outcome devoid of perceived risk. The same principle applies to the ongoing discourse regarding GLP-1 medications. The genuine risk associated with ESG and PLG-1 is that patients have undergone alterations to their anatomy and physiology without demonstrable results. Several years into contemplating a treatment promising sustained outcomes, we find that the alterations have increased the overall risk.
As a surgeon, I encourage people to always ask questions and demand that scientific proof be provided. I am not opposed to progress; considering the nature of our practice, we have witnessed and have unrgone significant evolution over the past 30 years, transitioning from performing open cases necessitating a hospitalization period of 4 to 6 days to performing the same cases laparoscopically and robotically in some cases outpatient procedures.
I was asked if my opinion of SIPS-SADI has changed since ASMBS endorsed it.
Let me remind everyone that ASMBS also endorses Adjustable Gastric Banding. We know what happened to the story. Is anyone considering Lap Band, even though ASMBS endorses it?
I am a member of ASMBS. The endorsement of the ASMBS does not unequivocally validate the outcome of a procedure; it only states that is an available alternative.
As stated previously, patients should be clear that SIPS-SADI procedures are not Duodenal Switch operations. Any suggestion is misleading. The physiology of SIPS-SADI is very different than that of the duodenal switch operation. Complications are associated with them, as reflected by the revisions we do to convert them to a Duodenal switch with percentage-based measurement of the small bowel.
In our practice, we have had to revise SIPS-SADI to duodenal switch operation due to compilation such as bile reflux gastritis and inadequate weight loss.
Semaglutide (Ozempic, Rybelsus, Wegovy, Saxenda) and tripeptide (Mounjaro) treat type II diabetes. They work thru several complex pathways. An observed side effect that has been noted in diabetic patients has been weight loss.
Some have been advocating using the class of medications for weight loss. However, Wegovy is the only medication approved for weight loss in non-diabetic patients.
There is a lot to be discussed here:
1-the use of the medications for weight loss is an off-label use (except Wegovy)- meaning that the FDA did not approve the medication as a weight loss drug.
The practical implication is that the medication’s safety and complication profile in non-diabetic patients looking to lose weight may be unknown and has not been studied.
2-The medication has become available thru compounding pharmacies. It is crucial to appreciate that compounding medications do not meet the same rigor and standards and may, in fact, not be the same formula as the FDA has stated.. This also means that a compounding pharmacy does not approve the medications in several states.
3-The most critical issue for me is the lack of a “long-term plan.” It is not clear what would happen when the patient stopped the medication. Will the patient experience weight regain? Will the patient require higher doses of the medication to maintain the weight loss, or will the medication stop working altogether? Unfortunately, we do not have these answers. For those skeptical about my questions, let me remind you that phentermine has significant side effects, and almost all patients experience weight gain when they have to stop the medication because of the cardiovascular complication of medication.
We should be aware that being physically active is part of being healthy. Health is a combination of being physically active, having a healthy diet are all parts of the variables that contribute to our physical and mental well-being long-term.
The restrictions and the stressors caused by COVID-19 have resulted in our inability to maintain a healthy diet and be physically active. However, we must be vigilant with maintain our activity levels to combat health issues.
It is timely that the British Medical Journal has just published an entire issue regarding the significance of activity and our health as individuals and public health worldwide.
There are a few articles that are outlined here.
Ekelund et al. Reviewed published articles and correlated the activity level and mortality. They Concluded, “Higher sedentary time is associated with higher mortality in less active individuals when measured by accelerometry. About 30–40 min of MVPA per day attenuate the association between sedentary time and risk of death, which is lower than previous estimates from self-reported data.”
The benefits of weight loss surgical procedures are undisputed. Over the last decades, as the incidence of obesity has increased, so has the need for effective long-term treatment options. It is no secret that diet and exercise plans are only short-term remedies since none of them provide realistic long-term alternatives. Let’s be clear that a healthy diet and activity level are critical to a healthy body and mind and to the long-term success of weight loss surgery.
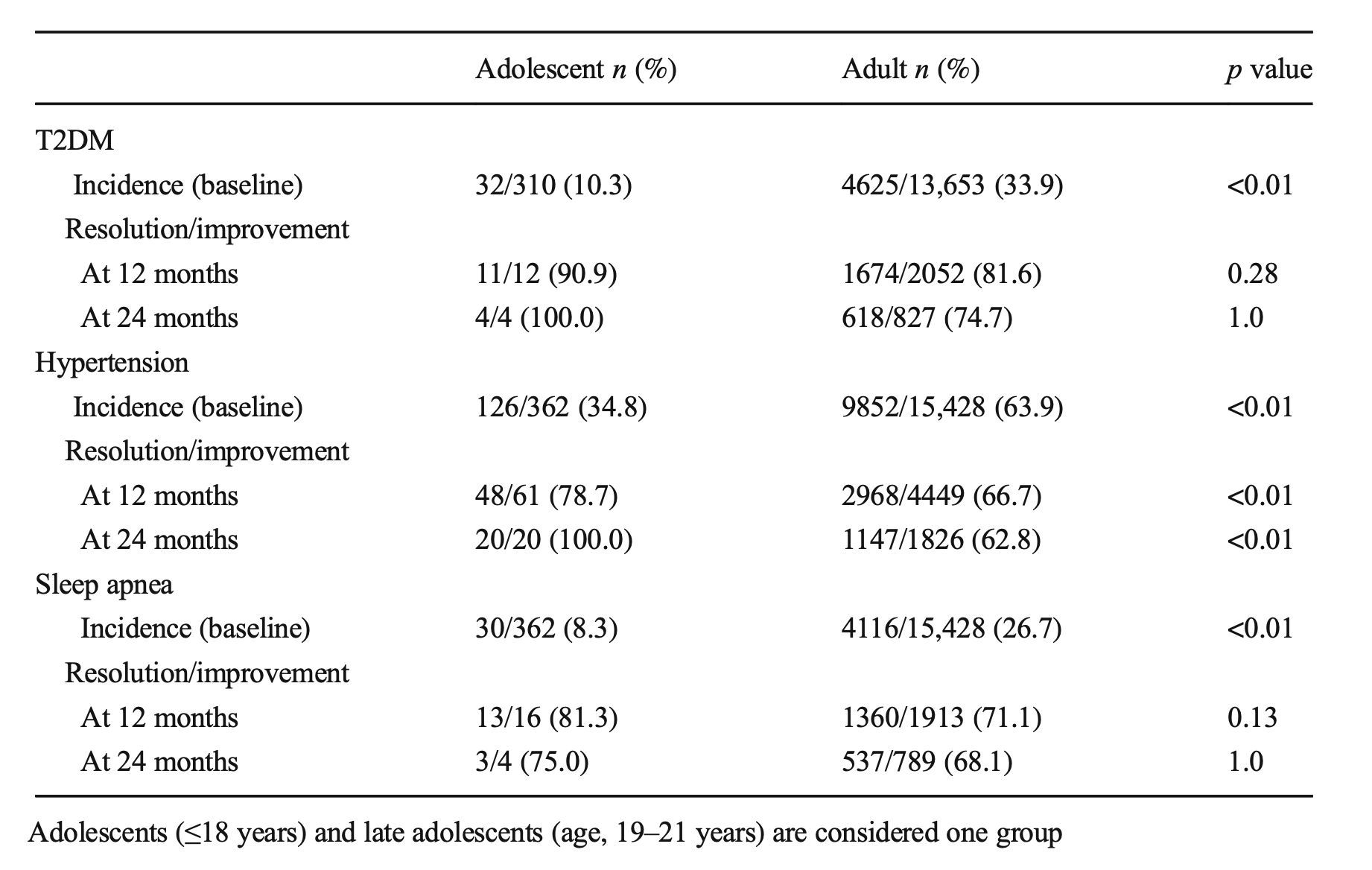
A frequent question: How young is too soon for weight loss surgery? We work with our patients to ensure that weight loss surgery will not affect the growth of an adolescent patient with regard to height, bone formation, and hormonal status. Specifically, there are concerns about a female patient’s ability to get pregnant and have children. All the scientific evidence points to the benefits of weight loss surgery and the improved ability to get pregnant and bear the pregnancy to completion. Weight loss positively impacts the ability to get and have a healthy pregnancy leading to a non obese child.
An article recently published demonstrated the benefits of early intervention. Specifically, it showed the improved odds of resolution of diabetes in the younger patients (100% in adolescents, Vs. 75% in adults ) at 24 months post-op.
Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
Here we go again…. There is a new cure for obesity, Gastric Balloon, with minimal to no risk, is an outpatient procedure and/or can be done in the surgeons office with no anesthesia. Have we not similar claimed like this before (Adjustable gastric band) ?
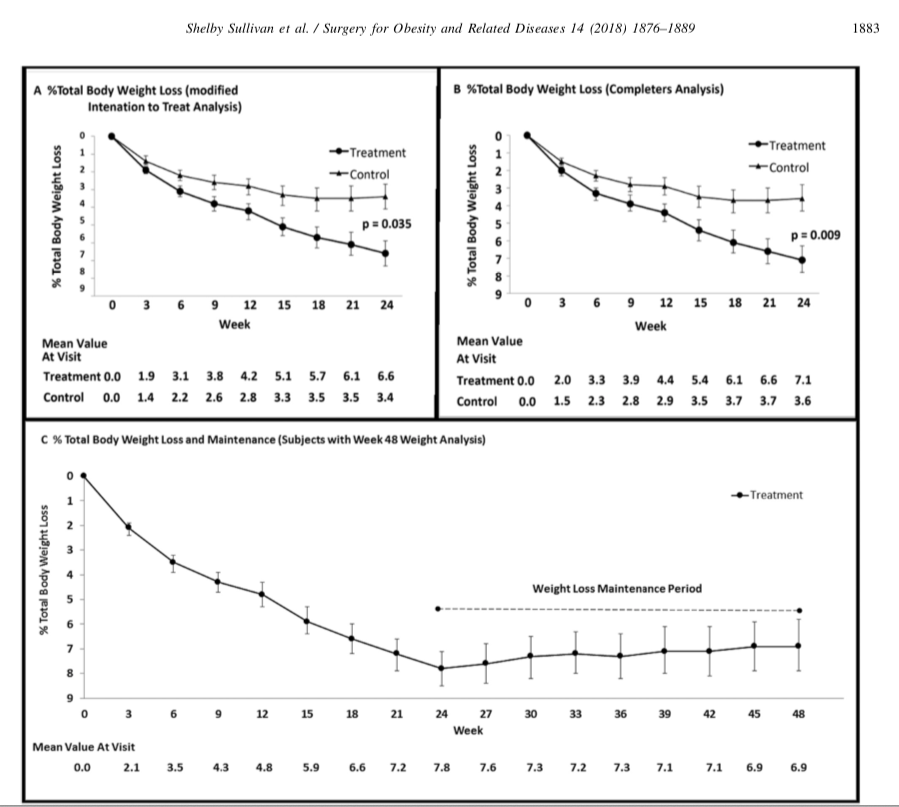
Randomized sham-controlled trial of the 6-month swallowable gas-filled intragastric balloon system for weight loss published in Surgery for Obesity and Related Diseases 14 (2018) 1876–1889, by Sullivan et. al reports
“Conclusions: Treatment with lifestyle therapy and the 6-month swallowable gas-filled intragastric balloon system was safe and resulted in twice as much weight loss compared with a sham control, with high weight loss maintenance at 48 weeks.”
This sound very promising, however is very vague and leaves out significant, critical, and pertinent information.
The outcome of weight loss at 24 weeks was reported in Total Body weight loss % (TBWL%), Excess weight % (EWL), weight loss, and BMI change. Of those, the last three were statistically significant changes.
The outcome the weight loss was reported to be at 7% TBWL% at 24 weeks with some weight regain, with the patient employing post REMOVAL life style changes.
It is stated that the Gastric Balloon is temporary device that needs to be removed in 6 months and should be considered in low BMI patients (<35kg/m2). It is is important for those patients who are considering this temporary expensive measure for minimal weight loss to entertain the alternative of the same temporary results that may be obtained by lifestyle changes. These results may be maintained by a healthy lifestyle, exercise, and eating without the need for a device.
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.
Gallbladder, Duct and Duodenum
When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.
Common_Cystic-Duct
Clipped_Cystic_DuctandArtery
In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.
Poly Cystic Ovarian Syndrome
Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.