Category: C.diff
Medication Accumulation in Gut Bacteria May Curb Drug Effectiveness, Alter Gut Microbiome
October 05, 2021 2:06 pm
Biofilm
April 26, 2020 9:44 am
Written By: Eric Baghdasaryan, Maria Vardapetyan, Osheen Abnous
Biofilm are tiny microorganism-filled communities found throughout the human gastrointestinal tract and oral cavity. These communities adhere to both biological and non-biological surfaces within the human body. They provide their inhabitants with many competitive advantages that help these bacterial communities withstand biological, chemical, and physical stresses1. Within these communities, microorganisms collaborate with one another to increase the likelihood of growth and multiplication despite the harsh conditions of the human gut. Not all bacteria within these biofilms are harmful, but those that are go on to cause infections and other severe health problems for the host.
Biofilm formation
Studies have shown that approximately 60-80% of bacterial infections in the human body are associated with biofilm formation. Such findings have compelled researchers to investigate the complex factors responsible for biofilm formation.

Figure 1: Biofilm adhesion, formation, and maturation. whiteley.com.au/biofilms
It was shown that bacteria anchor themselves to the mocosa surface. They collectively form a protective layer made of polysaccharides, proteins, and extracellular DNA. This forms the biofilm matrix. This biofilm matrix acts as a shield against antimicrobials, toxins, and antibodies. From here, biofilm associated bacteria go on to cause chronic infections characterized by persistent inflammation and tissue damage, initiating in the gut and adjacent regions of the gastrointestinal tract. Furthermore, some biofilm associated bacteria have shown the ability to disperse from this mature biofilm to colonize new niches, underscoring the association between local infections and systemic diseases such as atherosclerosis and rheumatoid arthritis2 caused by the buildup of biofilm dispersed bacteria and subsequent inflammation in the coronary vasculature and joint capsules, respectively. In fact, BADAS syndrome (bowel associated dermatosis-arthritis syndrome) is a condition where patients present themselves with small bumps on their inner skin (mainly along the vasculature) caused by the buildup of circulating microtoxins (very small clusters of bacteria). This may lead to chronic bacteremia in the bloodstream. Also, the over circulation of host immune complexes presents many problems for the patients, such as the development of arthritis and the accompanying joint pain, caused by the build up of white blood cells in host joint capsules. Patients often link the lumps to a dermatological condition, when in reality the condition is caused by a bacterial overgrowth originating in the gut and bowel. Clinicians now believe it is very likely these bacteria are biofilm-associated and a proper early diagnosis of the biofilm origin is critical to the prevention of BADAS and similar pathologies3.
The formation of biofilms has been studied on foreign substances such as intravenous catheters, orthopedic implants, and other biomaterials that have shown device-associated infections. However, it is commonly accepted that the majority of chronic bacterial infections involve biofilm formation on natural surfaces. The pathogenic bacterial overgrowth, forming the biofilms, have been linked to major diseases of the gastrointestinal tract including Inflammatory bowel disease and colo-rectal cancer4.
In addition to the gastrointestinal tract, biofilms can also be formed in the oral cavity. Over 700 bacterial species reside in the oral cavity. These contribute to the outgrowth of oral biofilms (otherwise known as dental plaque, see figure 2). These oral biofilms are responsible for major oral diseases such as tooth decay, gingivitis, and periodontitis. Moreover, those with periodontal infections have significantly increased risk of cardiovascular diseases, including atherosclerosis, myocardial infarction, and stroke2. The inflammation caused by oral biofilm may also be a contributing cause of conditions such as diabetes and rheumatoid arthritis1. Therefore, the control of oral biofilm growth before the development of oral infections is critical for the prevention of these system conditions.

Figure 2: Oral Biofilm Formation.
https://phys.org/news/2018-10-scientists-infection-causing-biofilms.html
This symbiotic (mutually beneficial) relationship between gut microbiota (bacteria living in our gut) and the host begins at birth and is crucial to our overall fitness and health. However, certain external and internal factors modify the gut microbiota. This causes the formation of a pathogenic biofilm, which leads to detrimental health conditions. The same bacteria that was once helping us by maintaining a healthy gastrointestinal tract, is now triggering disease conditions4.
Due to bacteria’s ability to translocate, migrate, and colonize new surfaces or niches, biofilm associated infections in the gut have been linked to systemic infections in other organs, including the joints, the skin, the eyes, the vasculature, the lungs, and even the central nervous system. It is assumed that the formation of a thick mucosal biofilm might be used as a diagnostic biomarker for the onset of systemic diseases. The outgrowth of a biofilm is widely viewed as the tipping point between two alternative states: a healthy and diseased gut1.
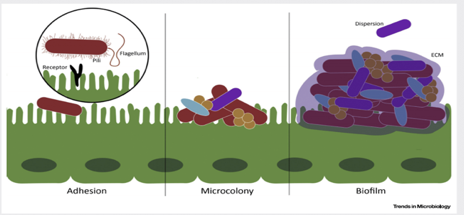
Figure 3. Biofilm matrix – a protective layer. Trends in Microbiology.
The biggest clinical challenge with biofilm-associated infections is their high resistance to antibiotic therapy. The effective therapeutic concentration of certain antibiotics to fight off bacteria within a biofilm (amount of the antibiotics needed in order to have positive therapeutic effects) is about 100-1000-fold higher than if the same bacteria were not associated with a biofilm2. The extracellular matrix, scaffold that keeps the bacteria anchored in place, prevents the penetration of host immune cells into the biofilm, thus contributing to the increased survival of the bacterial species living within the biofilm. Bacteria living within a biofilm also undergo an increased number of mutations, leading to the generation of more antibiotic-resistant phenotypes of bacteria. Finally, studies have shown that minimal concentrations of antibiotics may actually facilitate and stimulate biofilm formation, which can be extremely problematic in clinical treatment2. Therefore, to decrease the risk of biofilm induction, physicians should begin with very high doses of chemotherapeutics (antibiotics) from the very beginning of diagnosed infection. Looking ahead, there is clearly a need for novel biofilm-targeted therapies that are specifically made to prevent biofilm formation as well as eliminate the biofilm completely once it has already matured. Researchers have identified several drug candidates – DNase, lactoferrin, chlorhexidine, and taurolidine2 – that they believe have the potential to effectively penetrate and destroy components of the biofilm matrix. Further research is needed to determine their efficacy.
References
- Tytgat HLP, Nobrega FL, van der Oost J, de Vos WM. Bowel Biofilms: Tipping Points between a Healthy and Compromised Gut? Trends in Microbiology. January 2019;27(1): 17-25. doi:10.1016/j.tim.2018.08.009.
- Marcinkiewicz J, Strus M, Pasich E. Antibiotic Resistance: a “dark side” of biofilm-associated chronic infections. Polskie Archiwum Medycyny Wewnetrznej (Polish Archive of Internal Medicine). 2013;123(6):309-312.
- Buret AG, Motta JP, Allain T, Ferraz J, Wallace JL. Pathobiont release from dysbiotic gut microbiota biofilms in intestinal inflammatory diseases: a role for iron? Journal of Biomedical Science. January 2019;26(1) doi:10.1186/s12929-018-0495-4
Flagyl
September 25, 2019 9:07 am
Flagyl is sometimes prescribed for excessive gas and diarrhea. It is an antibiotics that works well on certain bacteria that accumulates in the GI tract and contributes to the gas and the bloating.
These bad bacteria flourish when patients consume significant and excessive fiber and carbohydrates (sugars, salad, pasta etc.) The FIRST line of defense against flatulence, bloating, and diarrhea should be eleminating the culprits in the diet. This point can not be stressed enough. Adding a daily dose of yogurt may improve symptoms due to yogurts probiotic benefits. To be beneficial, Yogurt should contain live bacteria cultures, not contain artificial sweeteners or have a high sugar content.
Artificial sweetness also area source of the excessive gas and should be avoided.
The Flagyl eliminates and reduces the bad bacteria. Along with a Probiotic and healthy dietary choices Flagyl can help to significantly improved or eliminate those symptoms of gas and diarrhea.
Before Flagyl is prescribed, it is important that the diet is critically examined to make sure that the carbohydrates and the fiber as source of gas and bloating is minimized or eliminated. Excessive use of medications that may be needed for other infections should be avoided.
Chronic diarrhea should be evaluated to rule out GI infection with C. diff bacteria or other bacteria or parasite.
Additional Information on C. Diff (Clostridium Difficile) and probiotics.
Probiotics, C. diff & Enteric Hyperoxaluria
July 26, 2014 3:21 pm
Calcium Oxalate Kidney Stones:
One DS specific advantage to adding a probiotic regime is the possible decrease in enteric hyperoxaluria, calcium oxalate kidney stones. Enteric hyperoxaluria is the mechanism of malabsorbed fatty acids in the colon binding with calcium thereby allowing oxalate to be absorbed into the blood stream. Also there is the theory that the unapposed bile salts may change the epithelial cells allowing oxalate absorption. “This increases the chance for oxalate kidney stone formation. Enteric hyperoxaluria is caused by jejunoileal bypass, as well as the modern bariatric procedure Roux en Y bypass. Patients with inflammatory bowel disease, pancreatic insufficiency, and intestinal resection for any reason are also at risk.” John Leske, M.D., Mayo Clinic. The fat blocking drug Zetia has also been linked to enteric hyperoxaluria. These research articles suggests that the use of Oxadrop ® probiotics, along with a low fat, low oxalate diet and increased hydration and increase calcium intake with meals, deceased the amount of oxalate absorption. Oxadrop® contains the bacteria Lactobacillus acidophilus, Lactobacillus brevis, Streptococcus thermophilus, and Bifidobacteria infantis. They suggest that the probiotic should be taken with meals and hypothesize that the probiotic bacteria possibly bind with oxalate, therefore deceasing oxalate absorption in the colon and also improve colon cells health. This is an area that needs additional study.
Another research study suggests that Oxalobacter formigenes may reduce the risk of Calcium Oxalate Kidney Stones. The study was a relatively small sample size but reports a 70% decrease in stone reoccurrence.
3. Align contains Bifidobacteria infantis
In conclusion, adding probiotics to the pre and post DS supplement regime can have benefits of improved weight loss, immune function, decreasing loose stools and possibly decreasing oxalate kidney stone formation. There are many types of probiotics on the market. In the U.S., probiotics are sold as a dietary supplement and are not held to the same standard that the medication are. There is no guarantee that the types of bacteria listed on a label are effective for the condition you’re taking them for. Health benefits are strain-specific, and not all strains are necessarily useful. It is beneficial to work with your physician to decide which probiotic may be the best choice for you.
A special thank you to Dr. David Caya, D.C. for his input into this post.