Category: esophageal ulceration
Sphincter of Oddi Dysfunction
April 26, 2026 8:43 am
Description:
Sphincter of Oddi Dysfunction (SOD) is a clinical syndrome characterized by biliary/ pancreatic pain from abnormal function or obstruction of the.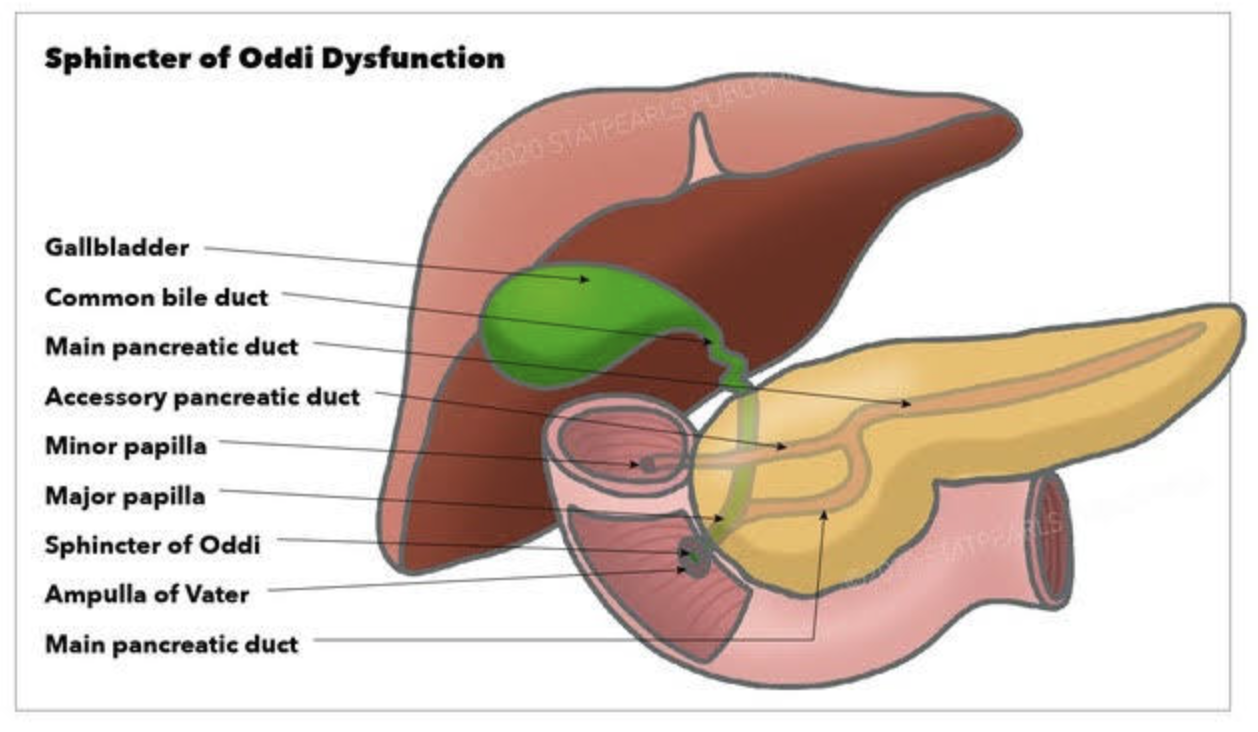
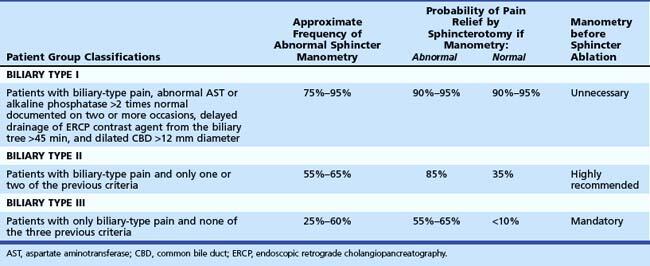
Diagnostic and classification
- The SOD spectrum includes biliary, pancreatic, or combined sphincter dysfunction, with symptoms driven by dyskinesia or mechanical obstruction. The term SOD encompasses both functional motility disorders (biliary or pancreatic sphincter dysfunction) and mechanical obstructions such as papillary stenosis.
- SOM has been considered the gold standard for diagnosing elevated basal sphincter pressure. It is invasive and carries complications, including pancreatitis. SOM can also not be done in those who have had gastric bypass or duodenal switch operations. Sphincterotomy outcome is not uniform. Consequently, many centers have moved toward empiric endoscopic therapy for appropriately selected patients and toward noninvasive or less invasive diagnostic approaches for others.
Treatment approaches
- Endoscopic biliary sphincterotomy (EST) is the most established nonpharmacologic treatment for biliary SOD, particularly in type I and many type II patients with objective ductal dilation and/or enzyme elevation.
- In type II SOD, outcomes after EST correlate with objective evidence of obstruction or sphincter hypertension on SOM. Empiric sphincterotomy without manometry is controversial.
- Type III SOD has emerged as predominantly functional pain rather than a mechanical obstacle. Alternative management emphasizes risk stratification, noninvasive strategies, and multidisciplinary approaches.
- Medical and non-sphincterotomy options (calcium-channel blockers, nitrates, antidepressants, and lifestyle modifications) have been discussed as potential adjuncts or alternatives.
Summary
- SOD is a multifactorial biliary and pancreatic sphincter disorder with a spectrum from mechanical obstruction to pure dyskinesia. Type I and II retain treatment relevance, particularly EST for biliary obstruction. Type II management requires clear identification of the cause.
- SOM is a diagnostic tool with significant limitations.
- Endoscopic sphincterotomy offers meaningful symptom relief in type I and select type II with objective obstruction. It carries a risk of complications, including pancreatitis; risk mitigation strategies are integral to practice. In type III SOD, sphincterotomy generally has limited benefit, necessitating a move toward noninvasive management and careful patient counseling. Patients post- gastric bypass, or duodenal switch, can not have ERCP or SOM done.
Bile Reflux Gastritis and Cholecystectomy
May 21, 2025 2:41 pm
Bile reflux gastritis is not a the result of the cholecystectomy but may be seen in a subset of patient with other confounding conditions. Bile is produced in the liver and stored in the gallbladder. In response to high fat and protein in the stomach, the gallbladder contracts to ” squeeze” the bile stored in the gallbladder into the small bowel to help absorb the fat and protein.

With the gallbladder removed, the bile produced by the liver cannot be stored and goes directly to the small bowel via the biliary tree.

It is possible and likely that some of the bile will find its way back to the stomach. In some patients, due to compounding circumstances, the bile may collect and cause gastritis. We need to dissect this a little for it to make sense.
- Not every patient after cholecystectomy will have bile in their stomach.
- Not every patient with bile in the stomach has gastritis.
To appreciate this, let’s remember that for bile to get from the small bowel to the stomach, it needs to:
- Go upstream, against the peristalsis of the small bowel, and do not be washed down by the flow of the gastric
- juices coming out of the stomach.
- Go through the pyloric valve.
- If it reaches the stomach, the acid in the stomach does not neutralize it, causing gastritis.

As I’m sure we all appreciate, other contributing factors besides cholecystectomy may cause bile reflux and bile reflux gastritis. This is why it’s also emphasized that bile in the stomach alone does not confirm biliary reflux gastritis. It is also why we always state that bile reflux gastritis is a disease of exclusion, where other conditions such as gastroparesis, acid reflux, and hiatal hernia (regardless of size, as some patients are unfortunately told that since the hernia is small it does not need to be fixed, which is incorrect) must be considered. Further information on Bile Reflux.
Billary Diversion is the only definitive surgical procedure for Bile Reflux Gastritis.
Bile Reflux Gastritis
August 02, 2024 10:53 am
Bile Reflux
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary tract flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or a tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis is reserved for cases with no alternatives.

Gastroesophageal Reflux: Bile Vs. Acid
May 14, 2019 12:52 pm
Gastroesophageal (GE) reflux is the condition when the stomach contents are able to “reflux” back through an incompetent lower esophageal sphincter (LES) into the esophagus.
Gastroesophageal reflux Disease (GERD) is a clinical condition caused by long-standing reflux that results in microscopic and visible changes to the inner lining of the esophagus and esophageal mucosa.
GERD is nondescript as to the cause of the condition. It only states that the stomach contents have been irritating the lining of the esophagus on a chronic basis. This can be caused by an anatomical abnormality of the GE junction (hiatal hernia) or may be related to dysfunction of the LES. Other possible causes of GERD may be infection (H. Pylori), environmental (stress), and dietary (nicotine, alcohol, caffeine, spicy food) in origin.
So far, we have not clarified the chemical nature of the refluxed content.
In Acid Reflux, the relative acid overproduction of acidic secretion and the exposure of the esophageal mucosa need to be addressed. This is accomplished by acid suppression medications, anti-histamine (H2 blockers), and Proton pump inhibitors (PPIs). The physiology and the mechanism involving this condition are well understood. As a surgeon, however, I do see patients who should have had surgical intervention. The initial mode of therapy for a patient with documented acid reflux and or symptomatic hiatal hernia is placing them on medication. These patients are then recommended to have a related upper endoscopy. Patients who do not improve or where deterioration of the esophageal mucosa and the presence of precancerous cells are referred for surgical intervention.
Bile Reflux, contrary to acid reflux, may have tiny, if anything, to do with the LES. The symptoms experienced by the patient may be as after related to the excessive bile in the stomach, which is seen frequently
after cholecystectomy, or in those patients with a dysfunctional gallbladder (low EF on HIDA scan).
The treatment of Bile reflux is Duodenal Switch without the associated sleeve gastrectomy component in addition to repair of hiatal hernia if present. Ann Surg. 2007 Feb; 245(2): 247–253.
GERD, Nausea and Vomiting- Don’t ignore it!
April 28, 2015 11:30 am
Gastroesophageal Reflux Disease is a serious matter and should not be left untreated. It is know as heartburn or reflux and if you are experiencing more than twice a week you should be evaluated by a physician to investigate the cause. Listed below are some of the causes and end results of not treating GERD.
Esophagitis – An irritant that can be acid, bile, food and digestive enzymes coming back up the esophagus can cause irritation and swelling in the esophagus. If left untreated, it can damage the lining of the esophagus to the point of erosion and scarring. Bile Reflux may also be a cause of esophagitis and Duodenogastroesphogeal reflux (DGER). Bile Reflux information here.
Esophageal Stricture – Scar tissue can cause the lumen of the esophagus to become smaller and narrow. This stricture makes it difficult or painful to swallow foods. If a stricture is narrow enough food may become stuck and require intervention for removal and treatment. This can also put a person at risk for choking. The treatment includes ballon dilation with an endoscope and in cases where it recurs surgery may be required.
Esophageal Ulceration– If GERD is left untreated it can progress to actual ulcerations in the esophagus. Patients may cough up or vomit blood or see it in their stool as dark tarry or coffee ground type stool.
Gastric Stricture– After weight loss surgery such as sleeve gastrectomy, RNY Gastric Bypass, Duodenal Switch, SADI/Loop, Adjustable Gastric Banding, or other gastric surgeries a narrowing of the inner opening of the stomach can result from scar tissue forming. This will require a surgical procedure to rectify. The symptoms can be food intolerance, full feeling, nausea and/or vomiting. (See pictures below)
Hiatal Hernia– An anatomical weakening or enlargement of the opening of the diaphragm muscle where the esophagus meets the stomach. This defect can allow a portion of the stomach to slide or roll into the chest cavity. This then causes reflux of gastric juice and content. Hiatal Hernia’s can also form on weight loss surgical patients. There are several examples within this blog here.
Breathing Difficulties– The acid aspiration while sleeping can make asthma and other breathing difficulties worst and can cause coughing and other issues.
Dental Issues – The acid, food, digestive enzymes backing up into the esophagus and mouth can cause dental issues such as erosion and tooth decay. In regards to dental issues after weight loss surgery there are also other vitamin and mineral deficiencies that can cause oral health issues. Dental Issues after WLS here.
Lower Quality of Life– GERD can affect a person’s quality of life. If you are in discomfort from acid reflux or having food intolerance it can make life difficult. It can also alter food choices and impact nutrition.
Barrets Esophagus– Pre-cancerous changes in the bottom portion of the esophagus due to long term acid exposure from gastric reflux. Diagnosis requires and endoscopic procedure (EGD) and biopsy.
Esophageal Cancer– There is a significant rise in the western world in esophageal adenocarcinoma. The main risk factors are alcohol use, smoking, untreated GERD, and poor diet.
Reflux and difficulty with swallowing caused by stricture is not normal. These problems are quite frequently encountered as complication of Adjustable gastric banding, with slipped band or a band that is too tight and scarred in placed resulting is belt effect. This results in the esophagus not being able to empty and propel the food down. The end result is significant reflux, with difficulty swallowing, nausea, vomiting etc. Similar problems are seen with Gastric bypass where the anastomosis between the stomach pouch and the small bowel RNY limb is too narrow. In Gastric Sleeve and Duodenal Switch operations, is the sleeve is made too narrow, or misshaped (hour glass, funnel, cork screw) it will result in the patient having reflux and symptoms of stricture. One specific problem with the new operation of SADI is the concern for risk of bile reflux, similar to the BillRoth I procedure.
Gastric bypass patient with stricture at the gastro-jejunostomy before and after balloon dilation. Fig A

After balloon dilation. Fig B

Fig. C : Lap band Patient with stricture where the band as removed at another facility and the scar tissue formed around the GE junction was not taken down. The patient had to be taken back to the operation room after his symptoms persisted even though the band had been removed 3 months prior.

A corkscrew stomach of a Duodenal Switch done at another facility, with the patient presented with persistent reflux, nausea and vomiting for years after surgery. Fig. D

This is not an inclusive discussion of GERD and the treatment. Please see your healthcare providers if you are experiencing any symptoms pertaining to GERD or any other health care issue.