Category: Vitamin D 25-OH
Vitamin D level and Liver Function Test (LFT) elevation
February 08, 2026 11:21 am
After weight-loss surgery, some patients may experience a transient elevation in liver function tests that resolves over time. We have previously reported on this. IT is essential to distinguish between the Duodenal switch and the SIPS/SADI procedure, where some patients are led to believe they are identical. These procedures differ physiologically, and their weight loss and metabolic behaviours vary significantly.
Other than the stress of the weight loss, obesity, and comorbidities of obesity, there may be other anatomical post-surgical causes for elevated liver function test. This has also been discussed extensively.
A recent literature review supports the protective effects of vitamin D supplementation.
Elevated liver enzymes may be caused by many factors, including nutritional deficiencies, excessive supplementation (turmeric), medications, alcohol, adhesions causing partial bowel obstruction, and increased enterohepatic bile reabsorption . I would be very cautious about associating vitamin D supplementation with elevated liver function test results, even if the vitamin D level is in the very high normal range, regardless of the daily dose (much less frequent with injectable).
Vitamin D, as a fat-soluble vitamin, however, protects the liver and improves liver function test even in very high serum level . In rare cases, prolonged, elevated vitamin D levels may strain the liver. In Fact, the association of the vitamin D level and liver disease, including cirrhosis, leads to hepatocellular carcinoma (HCC) and dea h. Vitamin D protects the liver from HCC but cannot reduce the risk of cirrhosis.
Vitamin Toxicity
December 17, 2024 1:36 pm
Patients are frequently asked to explain why they take high fat- or water-soluble vitamin doses. They are have often been scared by their well meaning healthcare providers that their higher levels of vitamin supplements will end up with vitamin toxicity.
Let’s clarify one point: there is such a thing as too much vitamin.
However, the point that is often overlooked in teaching within professional schools (medical, nursing, pharmacy, etc.) and drug manufacturers is that recommendations are based on “how much to take” and not how much is needed to keep a patient’s blood level in the normal range.

This table highlights how toxicity is described and what requirements are recommended. Vitamin toxicity is seen rarely in post-weight loss surgical patients who take them proactively in as many doses as needed to get their blood levels in the normal range. I see more patients in the office who suffer from low vitamin levels, such as vitamin D and A levels (duodenal switch and sleeve), than any patient with high or toxic levels of any vitamins.
Here is an example of critical vitamin A deficiency and night blindness and how, with aggressive large-dose supplementation, her condition was corrected.
Oral Vitmain D
September 24, 2021 3:42 pm
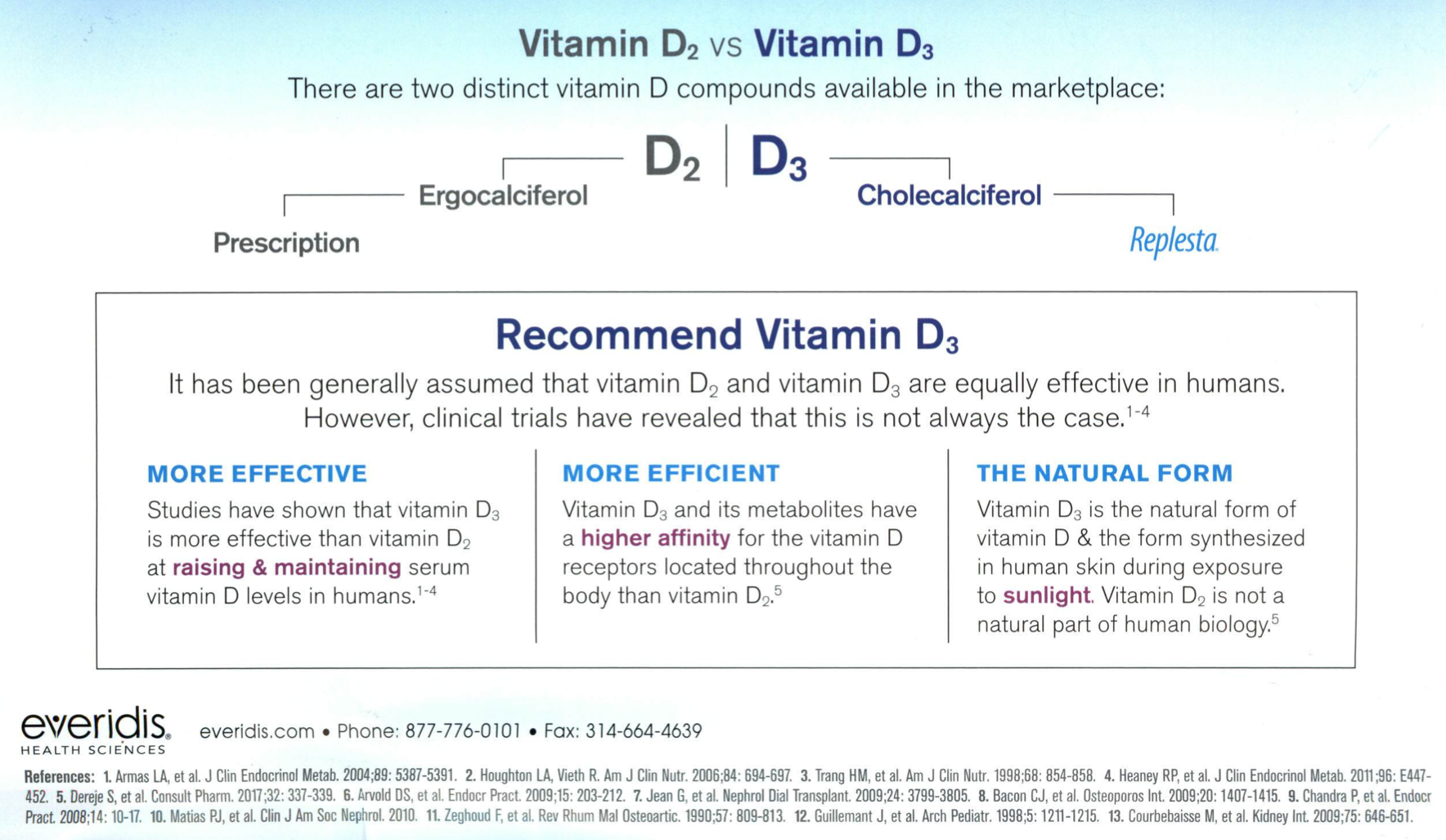
Over the Counter Vitmain D3 better than the Prescription Vitamin D2
August 30, 2021 10:41 am
COVID Vaccines
March 05, 2021 3:50 pm
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
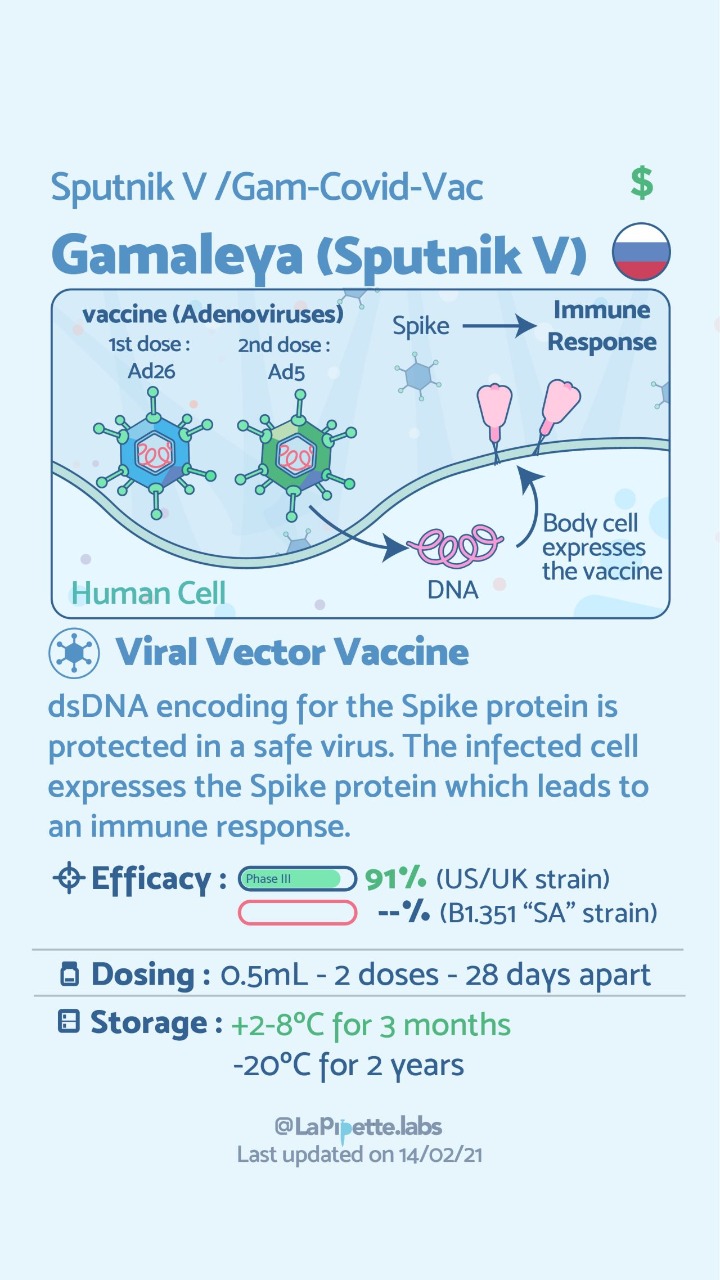
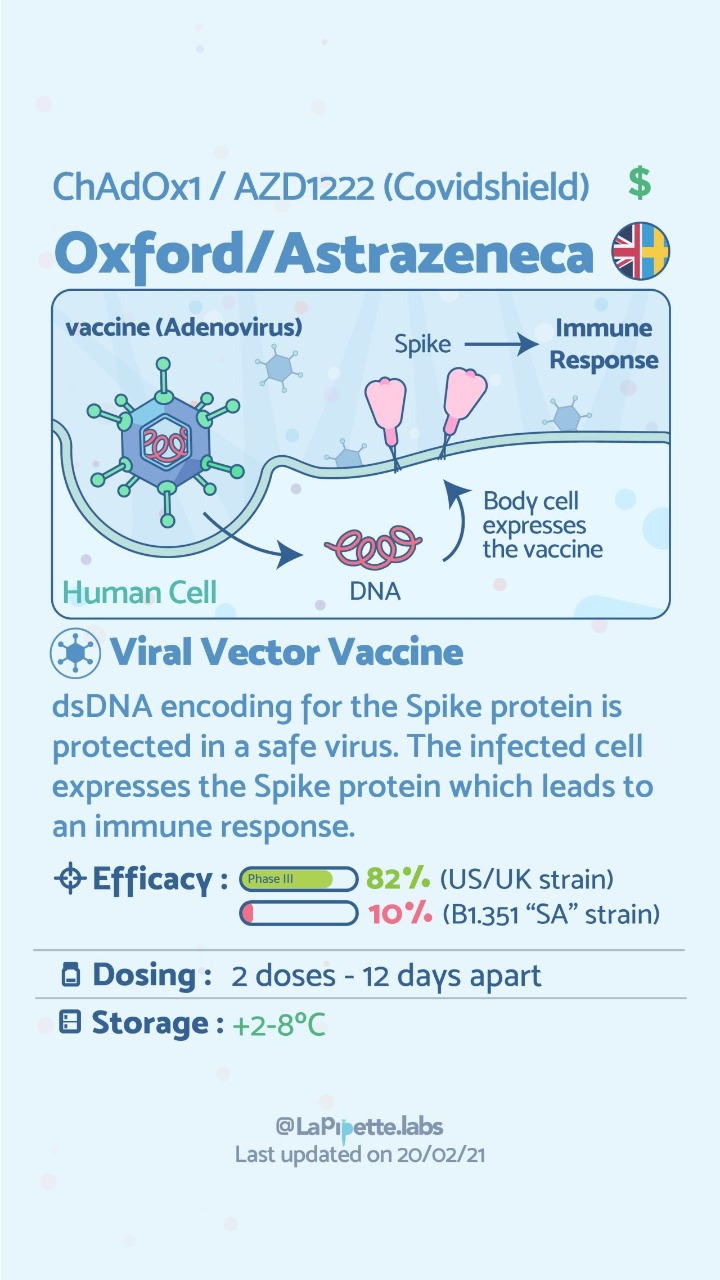
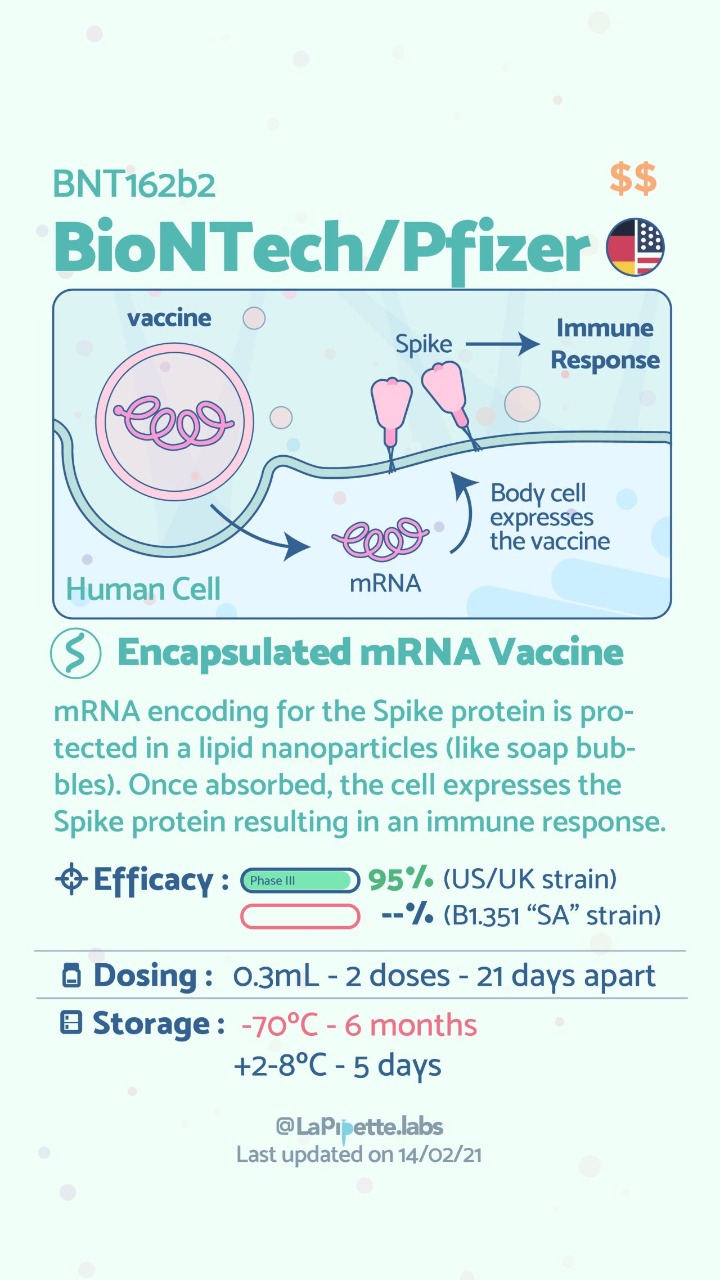
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Vitamin D, Immune Responce and COVID-19
January 26, 2021 6:45 pm
Vitamin D and Covid -19
May 07, 2020 9:24 am
We are all aware of the many roles that Vitamin D plays in our bodies. This includes immune function in addition to all the regulatory roles that Vitamin D plays in several physiologic reactions. There may be a correlation of low Vitamin D and COVID-19 infection increasing death risk as looked at in research articles.
Covid -19 in a subset of patience causes significant lung injury. These patients require mechanical ventilation.
Previously reported publications have suggested a possible correlation between ace inhibitors and increased risk of pulmonary complications of Covid -19. Some researchers suspect that the Covid-19 may be able to enter lung cells by the ACE receptors.
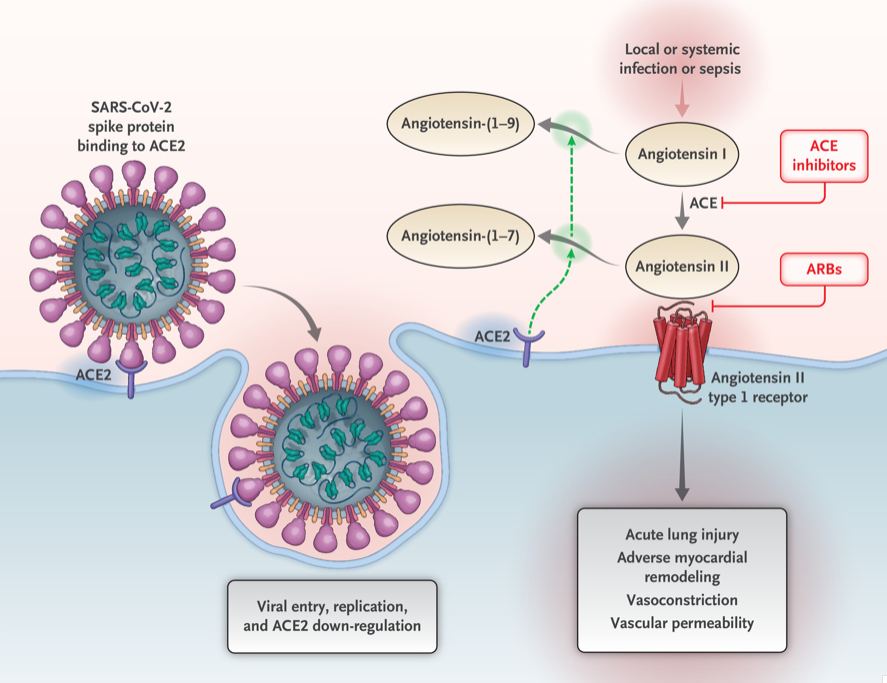
Vitamin D may positively implact the receptor ACE2. This study, report clear correlation between the high death rate with low vitamin D levels in Covid infected patients. There are limitation to this study that the attached abstract outlines.
Our take home message would be to please make sure you have updated labs and that you are all taking the recommended Vitamin D based on your surgical anatomy and laboratory values, not just an average non-bariatric person recommended dose.
https://www.dssurgery.com/wp-content/uploads/2020/05/manuscript.pdf
Vitamin D Metabolism and Deficiency file
March 28, 2020 8:17 am
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
In some cases, patients may need injectable Vitamin A or D to improve vitamin levels.
Click the links to view the information below and within the comments of this file:
Vitamin D3 50 by Biotech: Amazon
directly from BioTech:
Many DS surgeon’s do not recommend Children’s vitamins or chewable vitamins unless there is a specific reason or need for them.
DS Surgeon Blog on Vitamin D:
Webinar on Vitamin D metabolism:
Medications that effect Bone health:
This does not constitute medical advice, diagnosis or prescribing. It is simply a compiled list of gathered information. If you are in doubt or have questions please contact your medical healthcare professional.
Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium