There are 4 parathyroid glands which are located behind the thyroid gland, among other functions, are the main regulators of calcium, phosphorous, and magnesium in the blood. Elevations of parathyroid hormone (hyperparathyroidism) can be: 1-Primary, 2-Secondary, 3-Tertiary
Primary hyperparathyroidism means the parathyroid glands themselves are hyperactive. This may involve only one of the four glands: a) an adenoma, a benign tumor that needs surgical removal, or b) hyperplasia, when all 4 glands are hyperactive and/or enlarged, and in some cases, most of the 4 glands need to be removed.
Secondary hyperparathyroidism means that the elevated PTH level is caused by an external regulatory stimulus, such as low calcium, which itself may be due to low vitamin D, low calcium intake, or other causes.
Tertiary hyperparathyroidism is seen only in specific renal failure and transplant patients.
Regardless of the type of hyperparathyroidism, the end result is the same. Because the parathyroid gland aims to maintain normal calcium levels, it will do everything to achieve them. This includes increasing calcium absorption from the GI tract, breaking down bone to increase the blood calcium supply, and increasing calcium reabsorption from the urine.
Distinguishing between primary and secondary is critical, as primary is more likely than not a surgical problem that needs to be addressed. Secondly, it may be responding to metabolic deficiencies (low CA, low Vitamin D) that need to be corrected and take some time.
Not all cases require surgical intervention, as labs (vitamin D, calcium, and alkaline phosphatase) and imaging studies, such as neck ultrasound, CT scan, and Sestamibi scan, provide the information needed to dictate the treatment plan. Please stay up to date with your yearly lab results to catch changes sooner rather than later.
Iron is critical for the production and action of red blood cells. Deficiency of iron may have many causes. These include bleeding from the GI track, inadequate absorption, inadequate intake, and menstrual losses in females.
It’s important to have at least yearly laboratory studies to surveil for abnormalities. Normal results of iron testing may be different for men, women, and children. Iron and TIBC are measured in micrograms per deciliter (mcg/dL). Normal results for iron are:
65 to 175 mcg/dL for men
50 to 170 mcg/dL for women
50 to 120 mcg/dL for children
Normal results for TIBC are 250 to 450 mcg/dL for men and women.
To correct or prevent IDA, iron supplementation is recommend in some patients. Iron absorption is very inefficient. It take a long time to develop IDA and as long if not longer to correct it with oral supplementation. This is why we recommend some patient condor getting iron infusion.
For most, oral supplements are adequate. There are different formulary of iron supplement with varying degree of absorption.
Heme iron and iron bisglycinate have been shown to have much better absorption than ferrous sulfate formulary.
Endoscopic sleeve gastroplasty (ESG) differs from Laparoscopic sleeve gastrectomy (LSG).
ESG (Endoscopic Sleeve Gastroplasty) is promoted and advocated as a low-risk, equal alternative to the Laparoscopic Sleeve Gastrectomy, but it is not.
Anatomically speaking:
Endoscopic Sleeve Gastroplasty is an endoscopic procedure performed under general anesthesia. During this procedure, a specialized endoscope is inserted through the mouth into the stomach. Multiple plastic “H”-type anchors are used to create a fold in the stomach, thereby reducing its size. No part of the stomach is removed. Initial limited weight loss occurs as the patient feels full after consuming small volumes of food. This effect resembles what happens with the lap band and gastric balloon, and we know how the story ends with those.
LSG is performed laparoscopically with incisions on the abdomen under general anesthesia. Seventy-five to eighty-five percent of the stomach, along its greater curvature, is removed, eliminating the part of the stomach that produces the Ghrelin hormone, which controls and modulates hunger. This is why patients feel fuller with a smaller volume of food and experience significantly reduced hunger.
Results:
Please read the fine print
The summary results indicate
“Our results suggest that ESG is safe and effective for the treatment of obesity, with durable
long-term results for at least up to 5 years after the procedure. “
When you look at the details of the results, however, it states:
“At 5 years, mean TBWL was 15.9% (95% CI, 11.7-20.5, p < .001) and 90 and 61% of
patients maintained 5 and 10% TBWL, respectively.”
This means that five years after ESG, 90% of the patients have only lost 10% of their TBWL (total body weight loss), and 61% would have lost 10% of their TBW (Total Body Weight).
This serves as an illustration of how actual outcomes are obscured within the fine print, resulting in a lack of attention from individuals seeking the optimal outcome devoid of perceived risk. The same principle applies to the ongoing discourse regarding GLP-1 medications. The genuine risk associated with ESG and PLG-1 is that patients have undergone alterations to their anatomy and physiology without demonstrable results. Several years into contemplating a treatment promising sustained outcomes, we find that the alterations have increased the overall risk.
As a surgeon, I encourage people to always ask questions and demand that scientific proof be provided. I am not opposed to progress; considering the nature of our practice, we have witnessed and have unrgone significant evolution over the past 30 years, transitioning from performing open cases necessitating a hospitalization period of 4 to 6 days to performing the same cases laparoscopically and robotically in some cases outpatient procedures.
Semaglutide (Ozempic, Rybelsus, Wegovy, Saxenda) and tripeptide (Mounjaro) treat type II diabetes. They work thru several complex pathways. An observed side effect that has been noted in diabetic patients has been weight loss.
Some have been advocating using the class of medications for weight loss. However, Wegovy is the only medication approved for weight loss in non-diabetic patients.
There is a lot to be discussed here:
1-the use of the medications for weight loss is an off-label use (except Wegovy)- meaning that the FDA did not approve the medication as a weight loss drug.
The practical implication is that the medication’s safety and complication profile in non-diabetic patients looking to lose weight may be unknown and has not been studied.
2-The medication has become available thru compounding pharmacies. It is crucial to appreciate that compounding medications do not meet the same rigor and standards and may, in fact, not be the same formula as the FDA has stated.. This also means that a compounding pharmacy does not approve the medications in several states.
3-The most critical issue for me is the lack of a “long-term plan.” It is not clear what would happen when the patient stopped the medication. Will the patient experience weight regain? Will the patient require higher doses of the medication to maintain the weight loss, or will the medication stop working altogether? Unfortunately, we do not have these answers. For those skeptical about my questions, let me remind you that phentermine has significant side effects, and almost all patients experience weight gain when they have to stop the medication because of the cardiovascular complication of medication.
One consideration for anesthesia in weight loss surgery is “airway management.” A sleep and paralyzed patient loses the ability to breathe because of the medication given for general anesthesia. For this, a temporary breathing tube is placed. The breathing tube is then connected to the machine, where the oxygen is pumped in, and the carbon dioxide is removed.
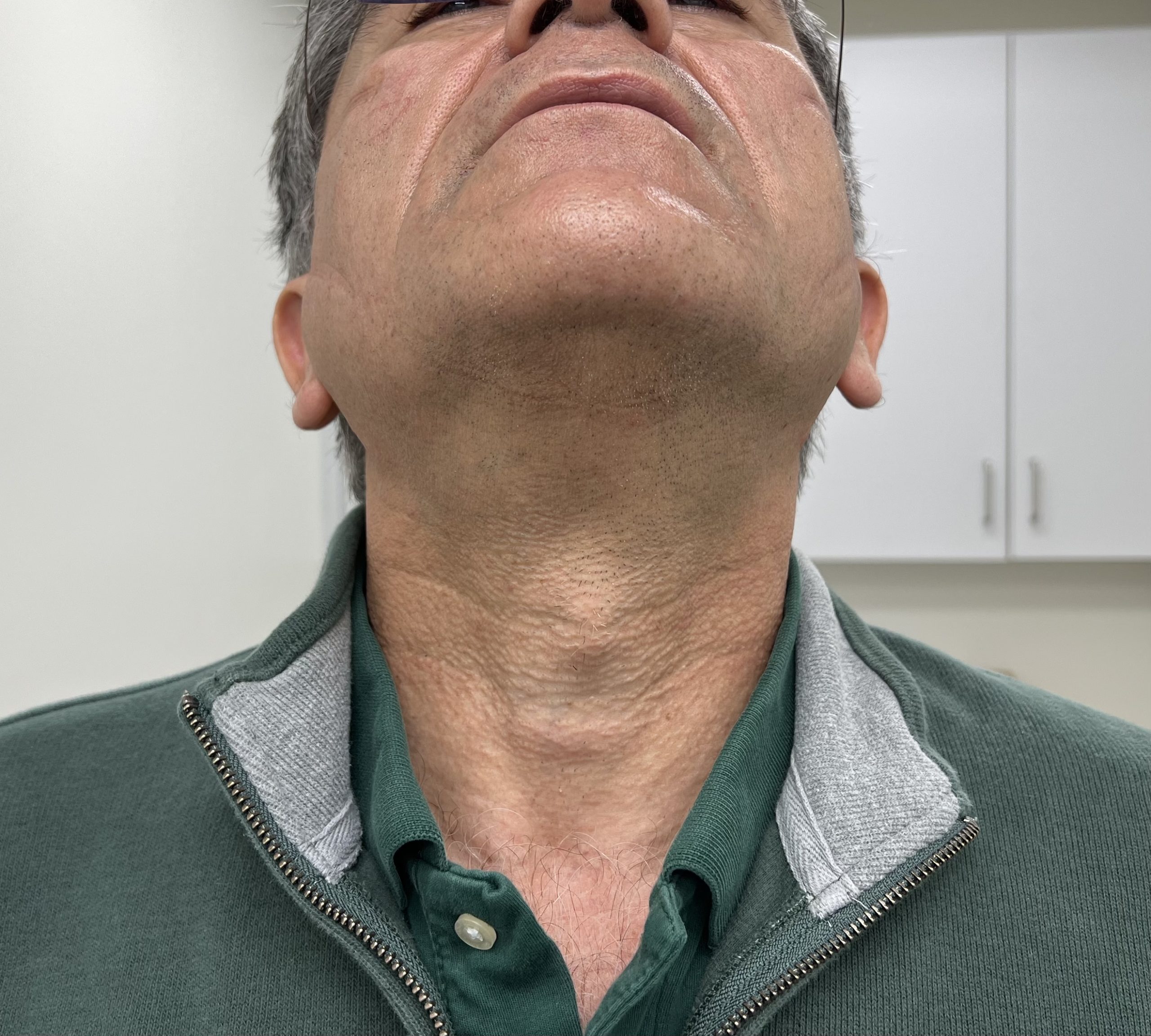
An anesthesiologist assesses the mouth and neck before the operation to evaluate the pertinent anatomy’s length, size, and position. This will dictate the instruments needed to insert the appropriately sized tube
The anesthesia staff may sometimes want pictures of your neck reviewed before surgery. If asked for photos of the neck, please take images similar to the one below and email them to [email protected].
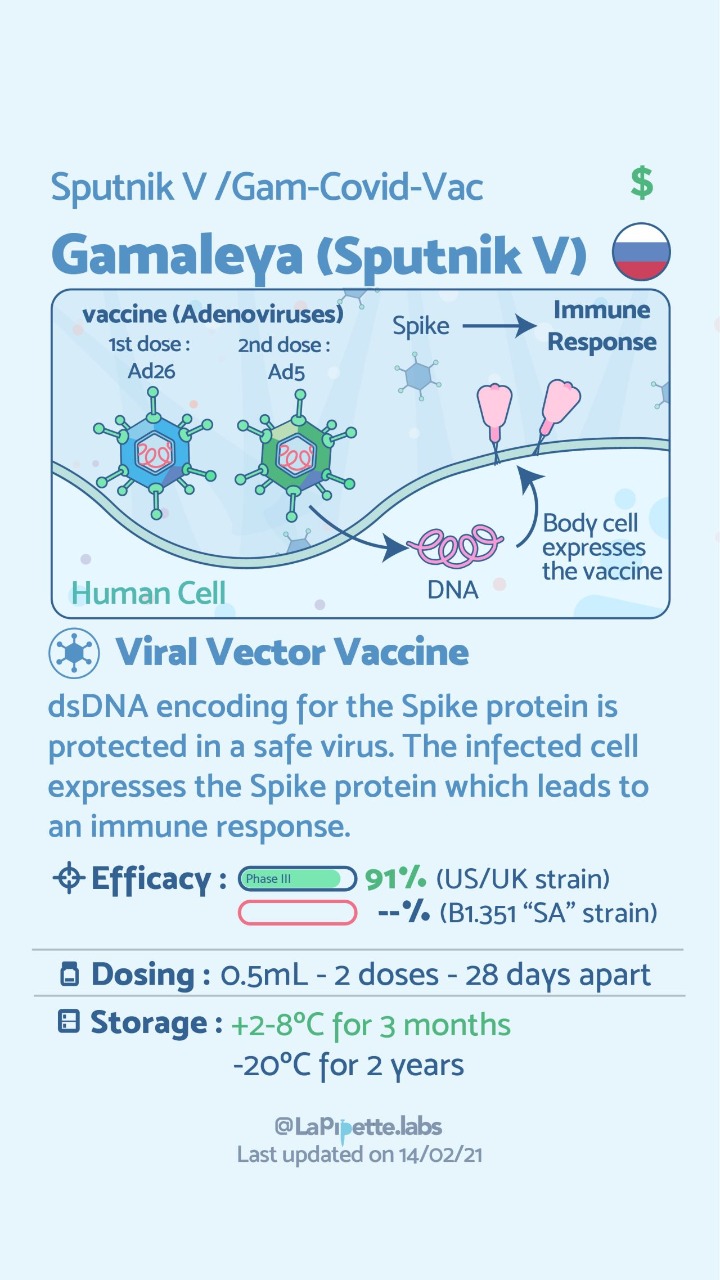
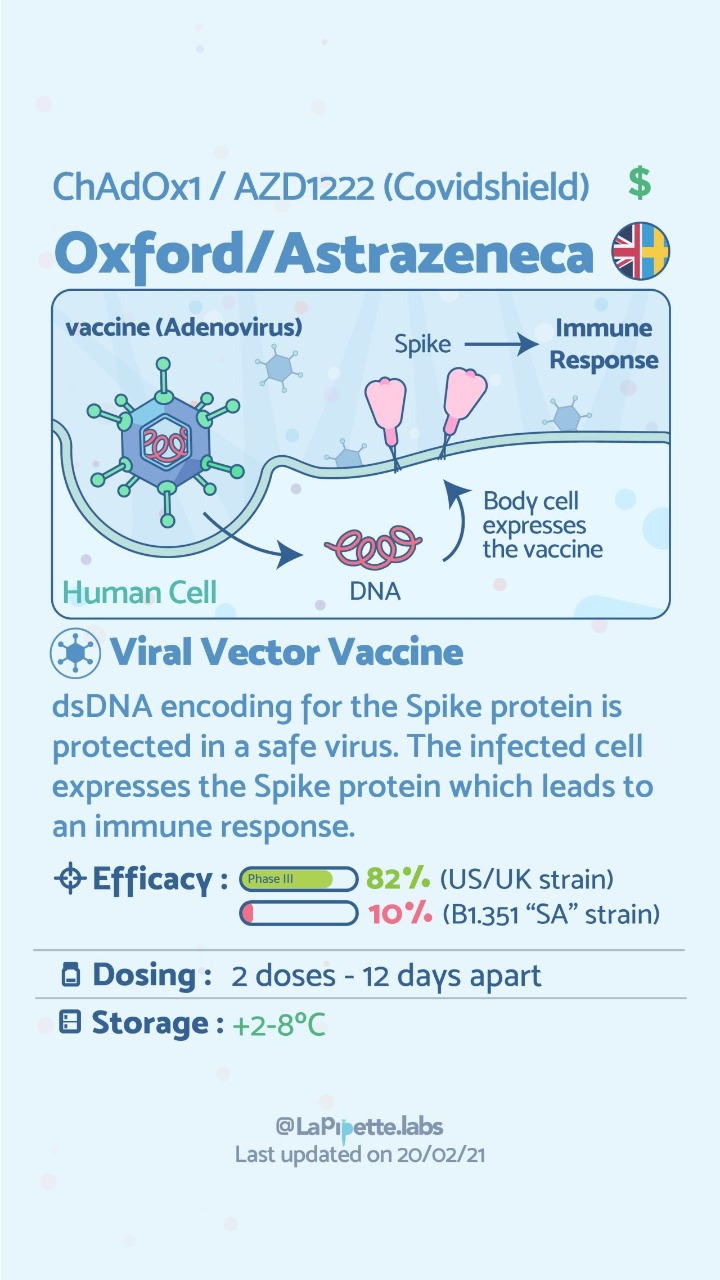
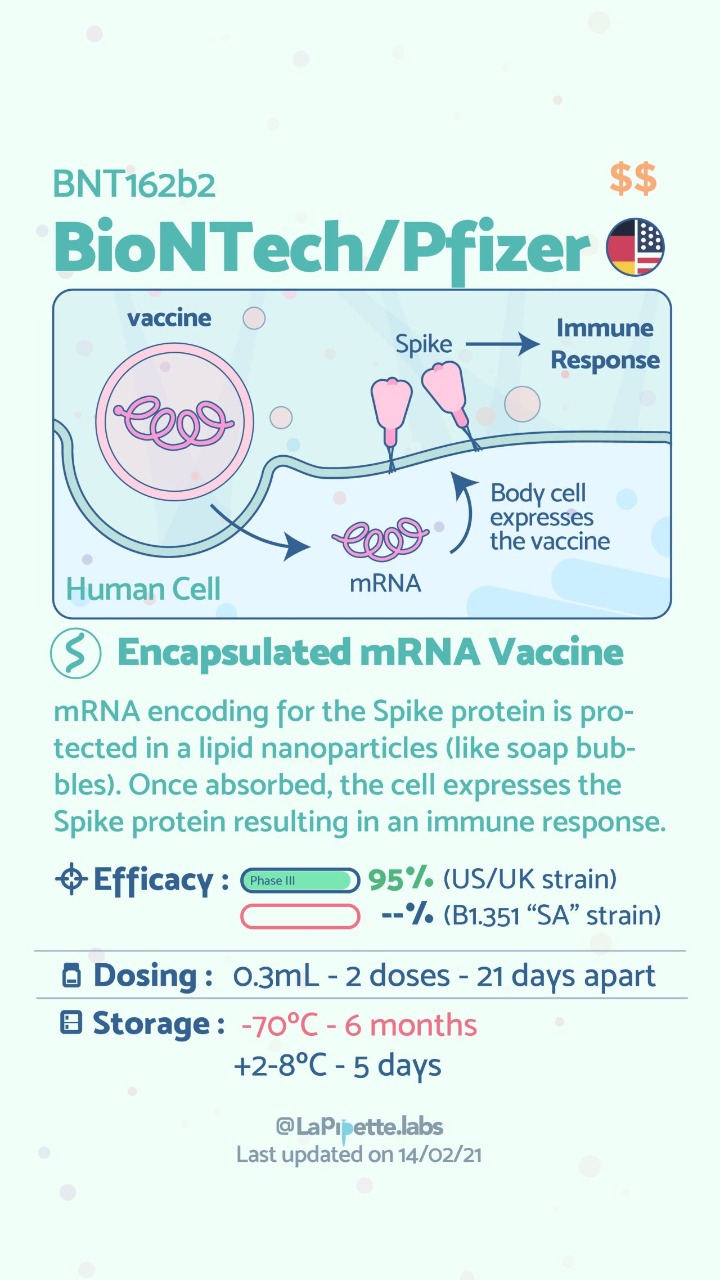
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.
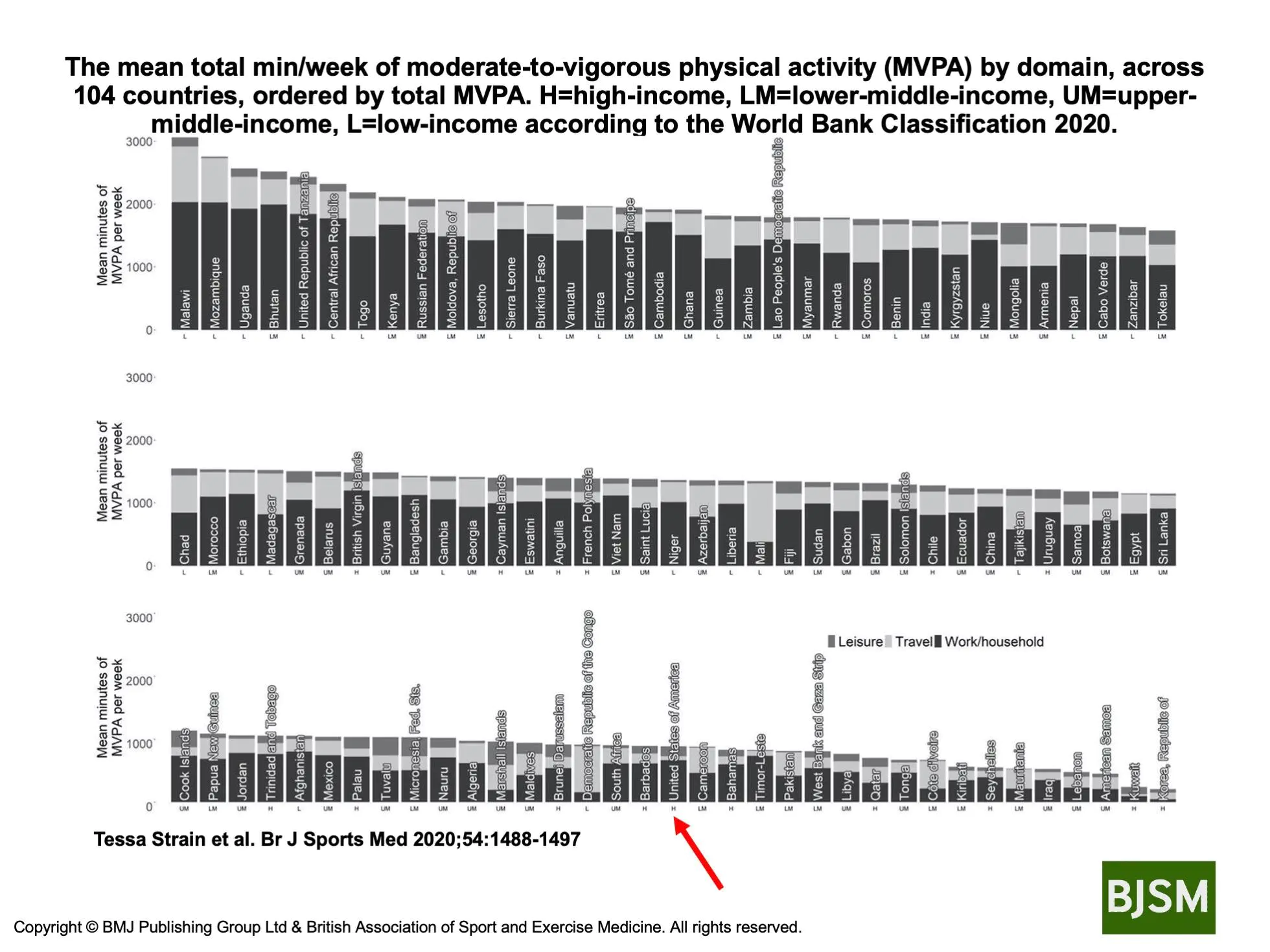
Physical activity in the U.S. varies based on geographic location, socioeconomic status and in comparison to other countries. It is important to know that physical activity is an important component of our well-being. However, this does not mean that going to the gym is the only way to be physically active.
Strain et al. Shows that different populations in different countries get their activity from different sources.
His research showed that the United States population ranked as a high-income country, ranks in the lower 1/3 of the number of countries surveyed with regards to the meeting minutes of moderate-to-vigorous physical activity (MVPA) per week. This may be a contributing factor to the significant rise in obesity in the United States. Individually we should all aim to increase our moderate to vigorous activity significantly.
The benefits of weight loss surgical procedures are undisputed. Over the last decades, as the incidence of obesity has increased, so has the need for effective long-term treatment options. It is no secret that diet and exercise plans are only short-term remedies since none of them provide realistic long-term alternatives. Let’s be clear that a healthy diet and activity level are critical to a healthy body and mind and to the long-term success of weight loss surgery.
A frequent question: How young is too soon for weight loss surgery? We work with our patients to ensure that weight loss surgery will not affect the growth of an adolescent patient with regard to height, bone formation, and hormonal status. Specifically, there are concerns about a female patient’s ability to get pregnant and have children. All the scientific evidence points to the benefits of weight loss surgery and the improved ability to get pregnant and bear the pregnancy to completion. Weight loss positively impacts the ability to get and have a healthy pregnancy leading to a non obese child.
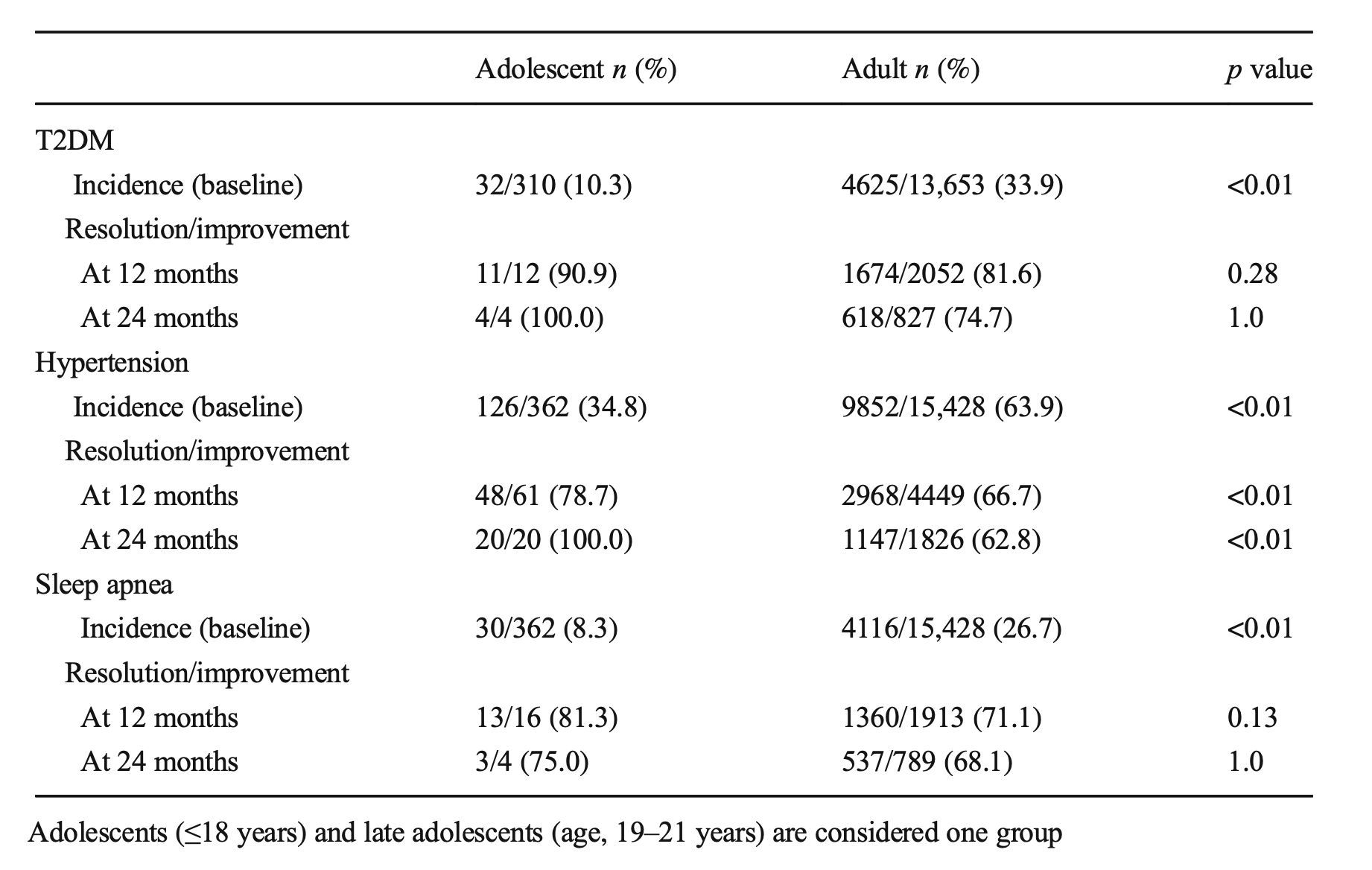
An article recently published demonstrated the benefits of early intervention. Specifically, it showed the improved odds of resolution of diabetes in the younger patients (100% in adolescents, Vs. 75% in adults ) at 24 months post-op.
Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
These meetings are for general topics and/or basic question and answers. If you need a more in-depth meeting we would suggest a video or in-person consultation with Dr. Keshishian. You can request a consultation via this link. Contact Us