Category: Esophagogastroduodenoscopy
Three Different Problems: Gastritis, Gastroesophageal Reflux, and Bile reflux Gastritis
June 05, 2025 4:52 am
Gastritis is a general term used for the description of symptoms associated with several very different physical conditions and require different treatments based on their ideology . Gastritis, gastroesophageal reflux, and bile reflux gastritis
Gastritis may be caused by excess acid or bile in the stomach. Some patients may have gastroesophageal reflux due to a hiatal hernia, which needs to be treated surgically with Nissen fundoplication, regardless of the size of the hernia, contrary to what gastroenterologists recommend by prescribing antacids for an extended period. I have seen patients who have had one cm hiatal hernia and have been very symptomatic, and others who have had larger hiatal hernias and have been asymptomatic. Size should not be a determinant of whether the patient has had or will have a hernia repair or not.
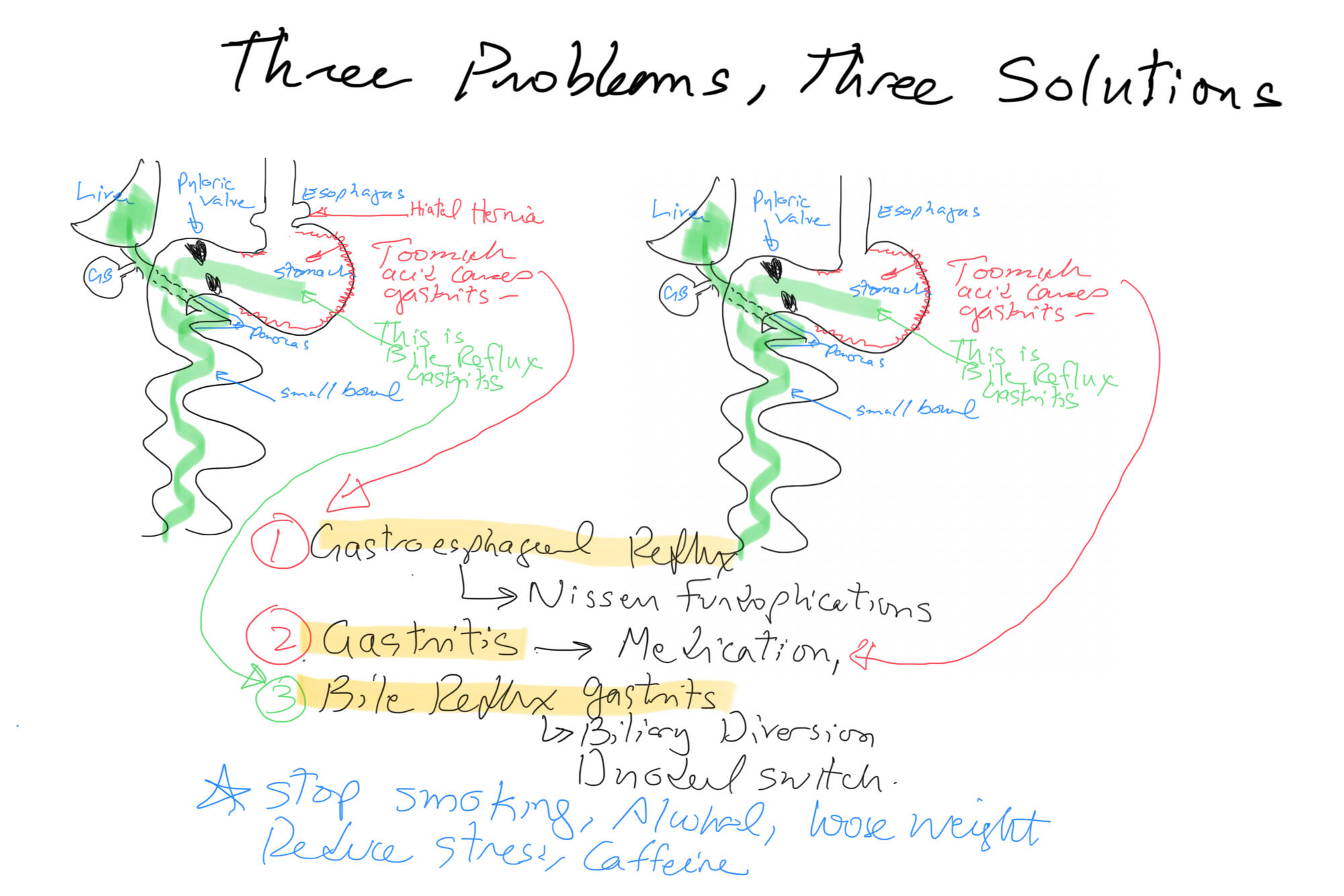
Billiary Diversion is the definitive surgical procedure for Bile Reflux Gastritis.
Gastroesophageal Reflux: Bile Vs. Acid
May 14, 2019 12:52 pm
Gastroesophageal (GE) reflux is the condition when the stomach contents are able to “reflux” back through an incompetent lower esophageal sphincter (LES) into the esophagus.
Gastroesophageal reflux Disease (GERD) is a clinical condition caused by long-standing reflux that results in microscopic and visible changes to the inner lining of the esophagus and esophageal mucosa.
GERD is nondescript as to the cause of the condition. It only states that the stomach contents have been irritating the lining of the esophagus on a chronic basis. This can be caused by an anatomical abnormality of the GE junction (hiatal hernia) or may be related to dysfunction of the LES. Other possible causes of GERD may be infection (H. Pylori), environmental (stress), and dietary (nicotine, alcohol, caffeine, spicy food) in origin.
So far, we have not clarified the chemical nature of the refluxed content.
In Acid Reflux, the relative acid overproduction of acidic secretion and the exposure of the esophageal mucosa need to be addressed. This is accomplished by acid suppression medications, anti-histamine (H2 blockers), and Proton pump inhibitors (PPIs). The physiology and the mechanism involving this condition are well understood. As a surgeon, however, I do see patients who should have had surgical intervention. The initial mode of therapy for a patient with documented acid reflux and or symptomatic hiatal hernia is placing them on medication. These patients are then recommended to have a related upper endoscopy. Patients who do not improve or where deterioration of the esophageal mucosa and the presence of precancerous cells are referred for surgical intervention.
Bile Reflux, contrary to acid reflux, may have tiny, if anything, to do with the LES. The symptoms experienced by the patient may be as after related to the excessive bile in the stomach, which is seen frequently
after cholecystectomy, or in those patients with a dysfunctional gallbladder (low EF on HIDA scan).
The treatment of Bile reflux is Duodenal Switch without the associated sleeve gastrectomy component in addition to repair of hiatal hernia if present. Ann Surg. 2007 Feb; 245(2): 247–253.
Hiatal Hernia Treatment
February 13, 2016 4:45 pm
Hiatal Hernia may be one reason for developing symptoms of GERD (Gastroesophageal reflux disease). As we have discussed previously, the treatment for reflux should not be long-term use of the “purple pill”, or all PPI’s, as advertised on TV. There is a large population who are delaying definitive care and probably increasing their chance of esophageal cancer by taming the symptoms of the reflux with over the counter or prescription medication. However, it is important to note that taming the symptoms isn’t necessarily stopping the effects. Be proactive and request to be sent to a surgeon to fix any issues if you are being recommended to “….take the medication and come back again for another endoscopy again ….”
Types of Hiatal Hernia:

This is an example of a patient who had been told to take the medication and just keep and eye on it with repetitive endoscopies. He had to have hiatal hernia repair with Nissen fundoplication for progressively worsening symptoms even on maximum treatment.

This is another example of a hiatal hernia repair procedure of a patient with a previous history of sleeve gastrectomy. In this patient, mesh had to be placed in order to fix the hiatal hernia.
GERD, Nausea and Vomiting- Don’t ignore it!
April 28, 2015 11:30 am
Gastroesophageal Reflux Disease is a serious matter and should not be left untreated. It is know as heartburn or reflux and if you are experiencing more than twice a week you should be evaluated by a physician to investigate the cause. Listed below are some of the causes and end results of not treating GERD.
Esophagitis – An irritant that can be acid, bile, food and digestive enzymes coming back up the esophagus can cause irritation and swelling in the esophagus. If left untreated, it can damage the lining of the esophagus to the point of erosion and scarring. Bile Reflux may also be a cause of esophagitis and Duodenogastroesphogeal reflux (DGER). Bile Reflux information here.
Esophageal Stricture – Scar tissue can cause the lumen of the esophagus to become smaller and narrow. This stricture makes it difficult or painful to swallow foods. If a stricture is narrow enough food may become stuck and require intervention for removal and treatment. This can also put a person at risk for choking. The treatment includes ballon dilation with an endoscope and in cases where it recurs surgery may be required.
Esophageal Ulceration– If GERD is left untreated it can progress to actual ulcerations in the esophagus. Patients may cough up or vomit blood or see it in their stool as dark tarry or coffee ground type stool.
Gastric Stricture– After weight loss surgery such as sleeve gastrectomy, RNY Gastric Bypass, Duodenal Switch, SADI/Loop, Adjustable Gastric Banding, or other gastric surgeries a narrowing of the inner opening of the stomach can result from scar tissue forming. This will require a surgical procedure to rectify. The symptoms can be food intolerance, full feeling, nausea and/or vomiting. (See pictures below)
Hiatal Hernia– An anatomical weakening or enlargement of the opening of the diaphragm muscle where the esophagus meets the stomach. This defect can allow a portion of the stomach to slide or roll into the chest cavity. This then causes reflux of gastric juice and content. Hiatal Hernia’s can also form on weight loss surgical patients. There are several examples within this blog here.
Breathing Difficulties– The acid aspiration while sleeping can make asthma and other breathing difficulties worst and can cause coughing and other issues.
Dental Issues – The acid, food, digestive enzymes backing up into the esophagus and mouth can cause dental issues such as erosion and tooth decay. In regards to dental issues after weight loss surgery there are also other vitamin and mineral deficiencies that can cause oral health issues. Dental Issues after WLS here.
Lower Quality of Life– GERD can affect a person’s quality of life. If you are in discomfort from acid reflux or having food intolerance it can make life difficult. It can also alter food choices and impact nutrition.
Barrets Esophagus– Pre-cancerous changes in the bottom portion of the esophagus due to long term acid exposure from gastric reflux. Diagnosis requires and endoscopic procedure (EGD) and biopsy.
Esophageal Cancer– There is a significant rise in the western world in esophageal adenocarcinoma. The main risk factors are alcohol use, smoking, untreated GERD, and poor diet.
Reflux and difficulty with swallowing caused by stricture is not normal. These problems are quite frequently encountered as complication of Adjustable gastric banding, with slipped band or a band that is too tight and scarred in placed resulting is belt effect. This results in the esophagus not being able to empty and propel the food down. The end result is significant reflux, with difficulty swallowing, nausea, vomiting etc. Similar problems are seen with Gastric bypass where the anastomosis between the stomach pouch and the small bowel RNY limb is too narrow. In Gastric Sleeve and Duodenal Switch operations, is the sleeve is made too narrow, or misshaped (hour glass, funnel, cork screw) it will result in the patient having reflux and symptoms of stricture. One specific problem with the new operation of SADI is the concern for risk of bile reflux, similar to the BillRoth I procedure.
Gastric bypass patient with stricture at the gastro-jejunostomy before and after balloon dilation. Fig A

After balloon dilation. Fig B

Fig. C : Lap band Patient with stricture where the band as removed at another facility and the scar tissue formed around the GE junction was not taken down. The patient had to be taken back to the operation room after his symptoms persisted even though the band had been removed 3 months prior.

A corkscrew stomach of a Duodenal Switch done at another facility, with the patient presented with persistent reflux, nausea and vomiting for years after surgery. Fig. D

This is not an inclusive discussion of GERD and the treatment. Please see your healthcare providers if you are experiencing any symptoms pertaining to GERD or any other health care issue.
Endoscopy Procedures and Duodenal Switch
February 27, 2014 6:58 pm
Upper Endoscopy (Esophagogastroduodenoscopy- EGD)
Gastrointestinal endoscopic procedures can be done in patients after the duodenal switch operation.
An upper endoscopy in an intact anatomy, involves examination of the esophagus, stomach, pyloric valve, and the duodenum including the ampulla of vater. This is where the biliopancreatic secretions are added into the GI track for absorption of the nutrients.
The upper endoscopy examination is limited after the duodenal switch operation to the first part of the three parts of the Duodenum. So the ampulla of vater can not be examined. This is also why an ERCP cannot be performed in patients after the duodenal switch operation.
Lower Endoscopy (Colonoscopy)
Duodenal switch operation does not change the anatomy of the large intestine. The colonoscopy examination can be done as with a patient who has not had the duodenal switch operation. The only consideration should be the bowel preparation. It has been noted that the patients after the duodenal switch operation require a longer than usual time for the bower prep. We recommend patients going on a liquid diet for 4-5 days before the planned procedure. I know it sounds unexpected that we recommend patients after the duodenal switch to be on liquid diet. You may also want the physician doing the colonoscopy be aware that you may need more aggressive and longer bowel prep.
Please see examples of the upper endoscopy here.
Does Size Matter
September 28, 2009 12:14 pm
The scientific basis for weight loss surgery, for the majority of the part relies on the premise that overeating and lack of exercise are the principal mechanisms contributing to the increase in the incidence of obesity over that last decade. Much has been said about our unhealthy life style that involves sedentary activity and immobility. Fast foods, high fat content meals, calorie dense food, are some of the examples of possible contributing factors to this health crisis.
The contrary position would be that there are other factors that contribute to obesity. These may include environmental factors, food preservatives, genetics, and exposures to toxins.
If one assumes that the over eating is the core problem, then you can also assume that the most successful operation will have the smallest stomach, since it will reduce the ability to over eat most drastically. This is where the scientific evidence does not support the theory and we all have to reassess the principal that the treatments are directed toward.
Recently there have been a number of studies that have been published in scientific journals that suggest size of the stomach or the pouch does not matter. So if obesity is the result of over eating then the operation that provides the smallest stomach must work the best. This argument should be true for the pouch size after gastric bypass, and the opening of the gastro-jejunostomy (connection between the stomach pouch and the small bowel connected to it after the gastric bypass, RNY operation). The same theory applies to the sleeve gastrectomy of the duodenal switch operation.
This argument that over eating and lack of exercise is the major contributing factor seems to be loosing ground.
The studies below are outline to demonstrate the disparity between the theory and the lack of scientific support for it.
1- Sanchez-Pernaute et.al. (Obesity Surgery, 17, 2007) reported that “After DS, gastric tube volume is not directly related to weight changes.” He proposed that there are other factors that may contribute to the weight loss than the size of the gastric tube.

This graph taken from the referenced study above shows that the size of the stomach sleeve does not correlate with the %EBWL in DS patients. The smaller stomach sleeve does not result in the more weight loss.
2- O’Connor et.al. (SOARD 4(2008)399-403) reported that “With construction of divided, vertical, lesser curve-based small-volume (=<20cm3) gastric pouches, the actual size of the gastric pouch did not correlate wit the %EBWL at 1 year after Laparoscopic, GB [gastric bypass]”.
3- Nishie et.al. (Obesity surgery, 17, 2007) concluded that “pouch size area, measured by routine UGI [upper GI series] on the first post operative day, does no influence short-term postoperative weight loss”.

This a sample of a number of graph that Nishie published in her study. The similar graphs were for 3, 12, and 24 months. They all had a flat line distributions. What they are showed was regardless of the time lapsed from surgery, the %EBWL was independent of the size of the pouch measured immediately post operatively.
4- Cottam et.al. (Obesity Surgery, 2009, 19:13-17) reported “The level of restriction or the presence of stenosis achieved by different circular stapler sizes does not have a significant role in weight loss”.

This study was focused on the size of the opening that is made between the stomach pouch and the small bowel in the gastric bypass (RNY) operation. The weight loss did not differ in the two groups of the patients. One group had a 21mm stapler and the other one 25mm stapler used. The weight loss, as measured by %EBWL was nearly identical in both cases.
In summary, the size does not seem to matter. The size of the stomach pouch, when it gets to a certain size in not important. The smaller stomach pouch or the narrower connection of the stomach and the small bowel will not make a patient loose more weight. Doesn’t this prove, to at least some degree, that there is much more to obesity than the simple notion of eating small portion and exercising?