Category: WLS
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
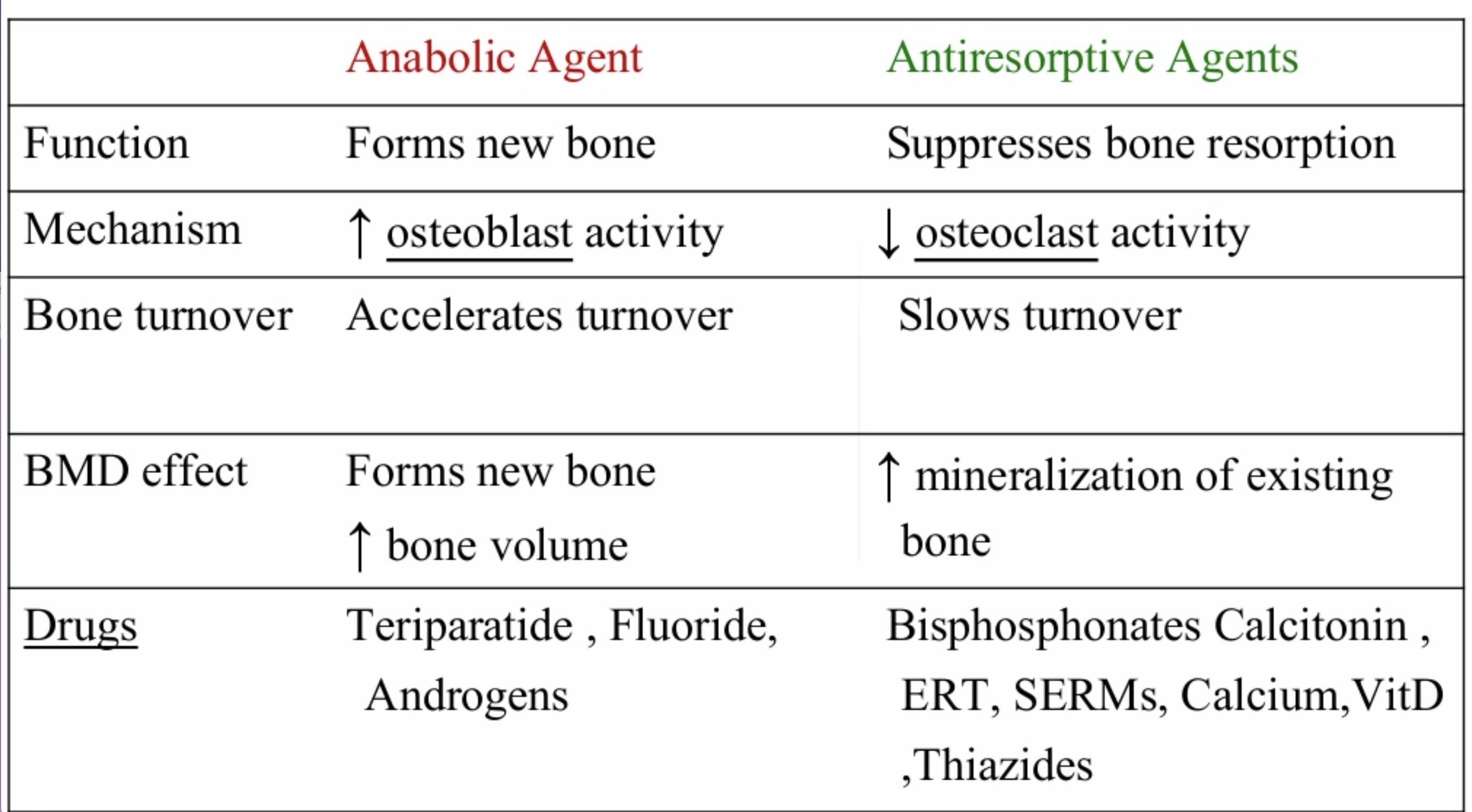
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
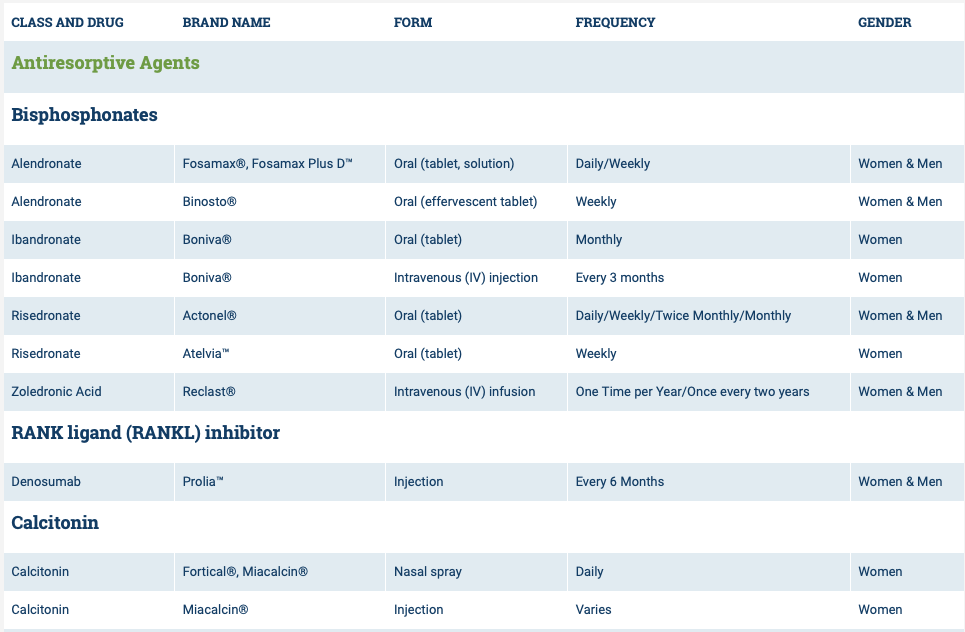
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

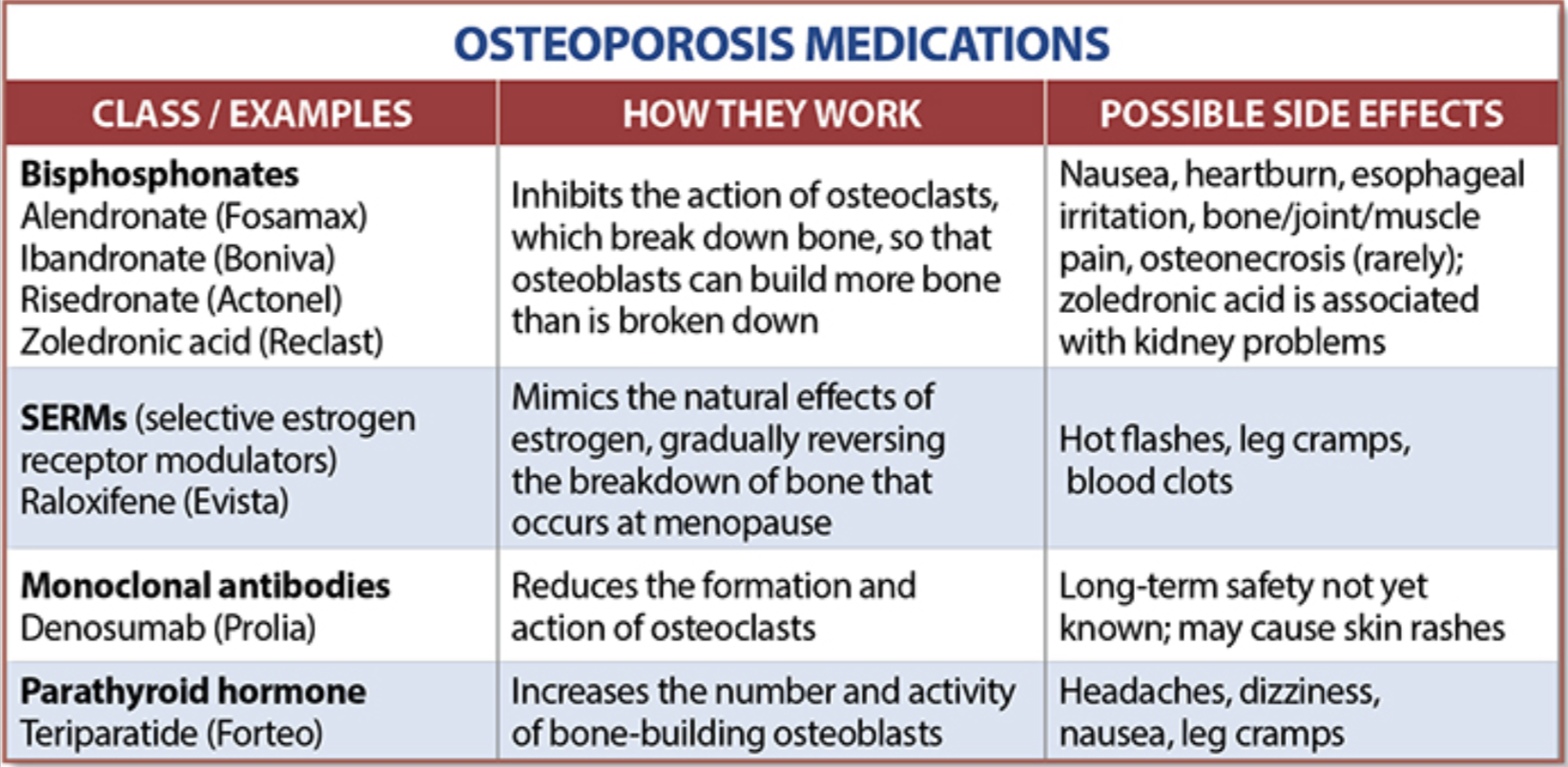
The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 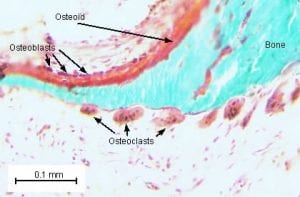
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
SIPS, SADI-S, Loop DS
May 01, 2019 9:03 am

The American Society for Metabolic and Bariatric Surgery (ASMBS) and MBSAQUIP-A on March of 2019, published and updated list of “Endorsed Procedures and Devices”
Endorsed Procedures and Devices | American Society for Metabolic and Bariatric Surgery
Note that any surgical procedures that does not employ two anastomosis, are not endorsed and are only recommended to be performed with an IRB (Institutional Review Board) or an IRB exemption. Duodenal Switch, Sleeve Gastrectomy, Roux en Y Gastric Bypass, Gastric Balloon, Adjustable Gastric Banding, and Nerve Blocking which are endorsed procedures.
SIPS, SADI-S, SIPS, Loop DS are all in the category of the “Non-Endorsed Procedures and Devices”. To see an anatomical comparison of these procedures to the Duodenal Switch procedure.
Patients should request that their consent be clearly defined and should explicitly outline the procedure that is being proposed to them. This is to avoid a patient having a procedure that they assumed, or are led to believe to be a Duodenal Switch operation with two anastomosis. Do your due diligence and know the procedure you want. Investigate if the surgeon you are working with performs the procedure you are interested in. Have them draw a picture of the procedure or give you a diagram of the procedure.
Dr. Facebook
March 22, 2019 8:24 am
We have become reliant on the information that we obtain from the internet, specifically platforms such as Facebook. In our practice we have to continuously correct information that patients have obtained from other patients, unmonitored sites, blogs, and postings. Most of this information is based on individual experiences that has become gospel. “Fat is good for you” is one of them. To clarify, some health fat (olive oil, avocado, Omega 3) is healthy and needed for all patients. We do not recommend “fat bombs” as a part of ones daily dietary intake.
The following article was written on the accuracy of nutritional posts in support groups on Facebook.
Koalall et. all in SAORD, December 2018 Volume 14, Issue 12, Pages 1897–1902 published
“Content and accuracy of nutrition-related posts in bariatric surgery Facebook support groups”
The conclusion, as suspected, that “Over half of the posts contained inaccurate content or information that was too ambiguous to determine accuracy..:”

It is our recommendation before any dietary recommendations are taken from facebook and the like, the source of the information should be verified. As I have stated in the past, a frequent flier passenger is probably not qualified to fly a
commercial airplane, any more than a previous weight loss surgical patient providing medical and nutritional advice. We realize that there is significant value to the forum for exchange of information and sharing of experiences with other weight loss surgical patients as long as the information is well sourced and verified.
Gastric Balloon
March 12, 2019 9:10 am
Here we go again…. There is a new cure for obesity, Gastric Balloon, with minimal to no risk, is an outpatient procedure and/or can be done in the surgeons office with no anesthesia. Have we not similar claimed like this before (Adjustable gastric band) ?
Randomized sham-controlled trial of the 6-month swallowable gas-filled intragastric balloon system for weight loss published in Surgery for Obesity and Related Diseases 14 (2018) 1876–1889, by Sullivan et. al reports
“Conclusions: Treatment with lifestyle therapy and the 6-month swallowable gas-filled intragastric balloon system was safe and resulted in twice as much weight loss compared with a sham control, with high weight loss maintenance at 48 weeks.”
This sound very promising, however is very vague and leaves out significant, critical, and pertinent information.
The outcome of weight loss at 24 weeks was reported in Total Body weight loss % (TBWL%), Excess weight % (EWL), weight loss, and BMI change. Of those, the last three were statistically significant changes.
The outcome the weight loss was reported to be at 7% TBWL% at 24 weeks with some weight regain, with the patient employing post REMOVAL life style changes. 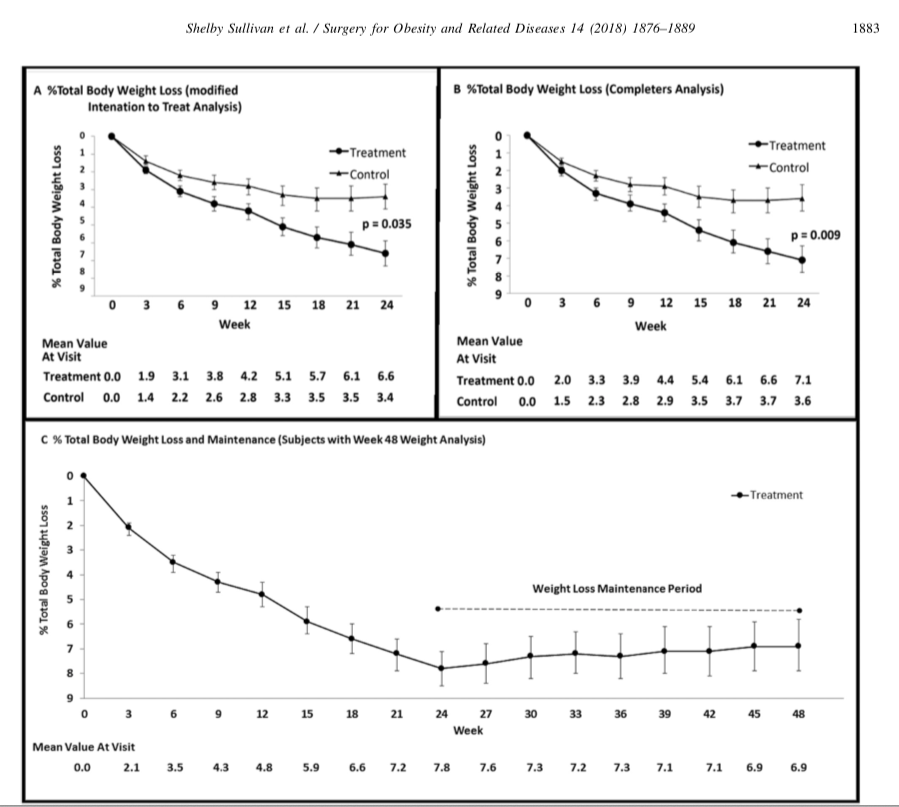
It is stated that the Gastric Balloon is temporary device that needs to be removed in 6 months and should be considered in low BMI patients (<35kg/m2). It is is important for those patients who are considering this temporary expensive measure for minimal weight loss to entertain the alternative of the same temporary results that may be obtained by lifestyle changes. These results may be maintained by a healthy lifestyle, exercise, and eating without the need for a device.
Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP
PolyCystic Ovarian Syndrome PCOS
September 04, 2018 9:58 am
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.

Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
Bariatric Surgery can improve PCOS in those individuals with Type 2 Diabetes Mellitus. Further information on weight loss surgery and its effect on PCOS here.
Health Insurances Working Against You
July 09, 2018 12:01 pm
Are Health Insurances working against you? Especially in people who have the disease of obesity? Insurance companies continue to lengthen the pre-operative period. The time that is required to lapse has now in some cases been extended between 6-12 months for some commercial health plans. There are yet again studies that have shown no benefit to the patient with this mandated waiting periods imposed on the patients. Unfortunately, the patients need to challenge the health care insurance companies by the means of all options that may be available to them. This may include internal appeal to external evaluation by some state agency. There are numerous studies that show pre-operative dieting does not equal better weight loss or compliance.


Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium