Category: Two Staged Duodenal Switch
Vitamin D Metabolism and Deficiency file
March 28, 2020 8:17 am
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
In some cases, patients may need injectable Vitamin A or D to improve vitamin levels.
Click the links to view the information below and within the comments of this file:
Vitamin D3 50 by Biotech: Amazon
directly from BioTech:
Many DS surgeon’s do not recommend Children’s vitamins or chewable vitamins unless there is a specific reason or need for them.
DS Surgeon Blog on Vitamin D:
Webinar on Vitamin D metabolism:
Medications that effect Bone health:
This does not constitute medical advice, diagnosis or prescribing. It is simply a compiled list of gathered information. If you are in doubt or have questions please contact your medical healthcare professional.
Stapled Anastomosis
December 30, 2019 11:23 am
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
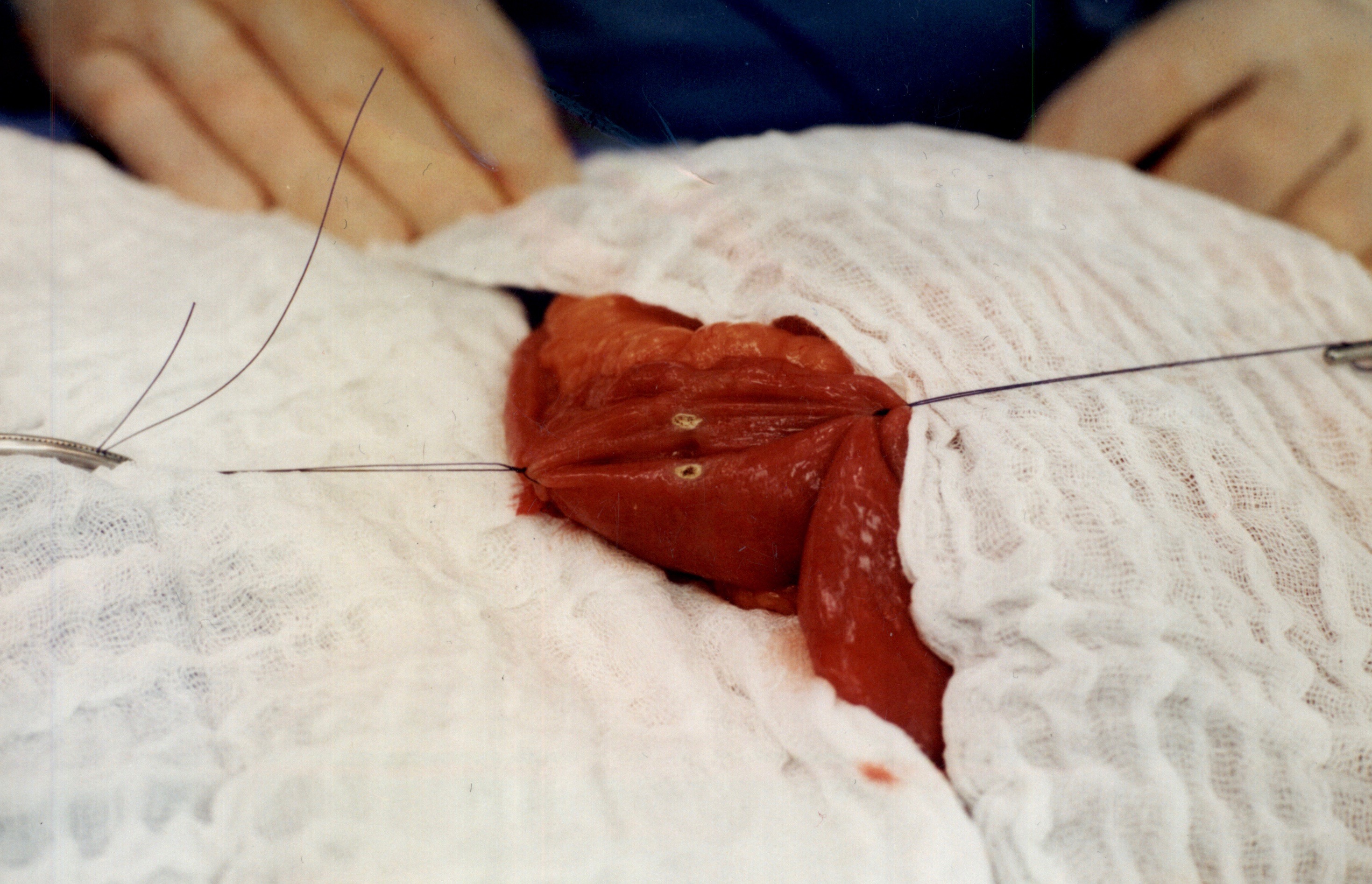
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
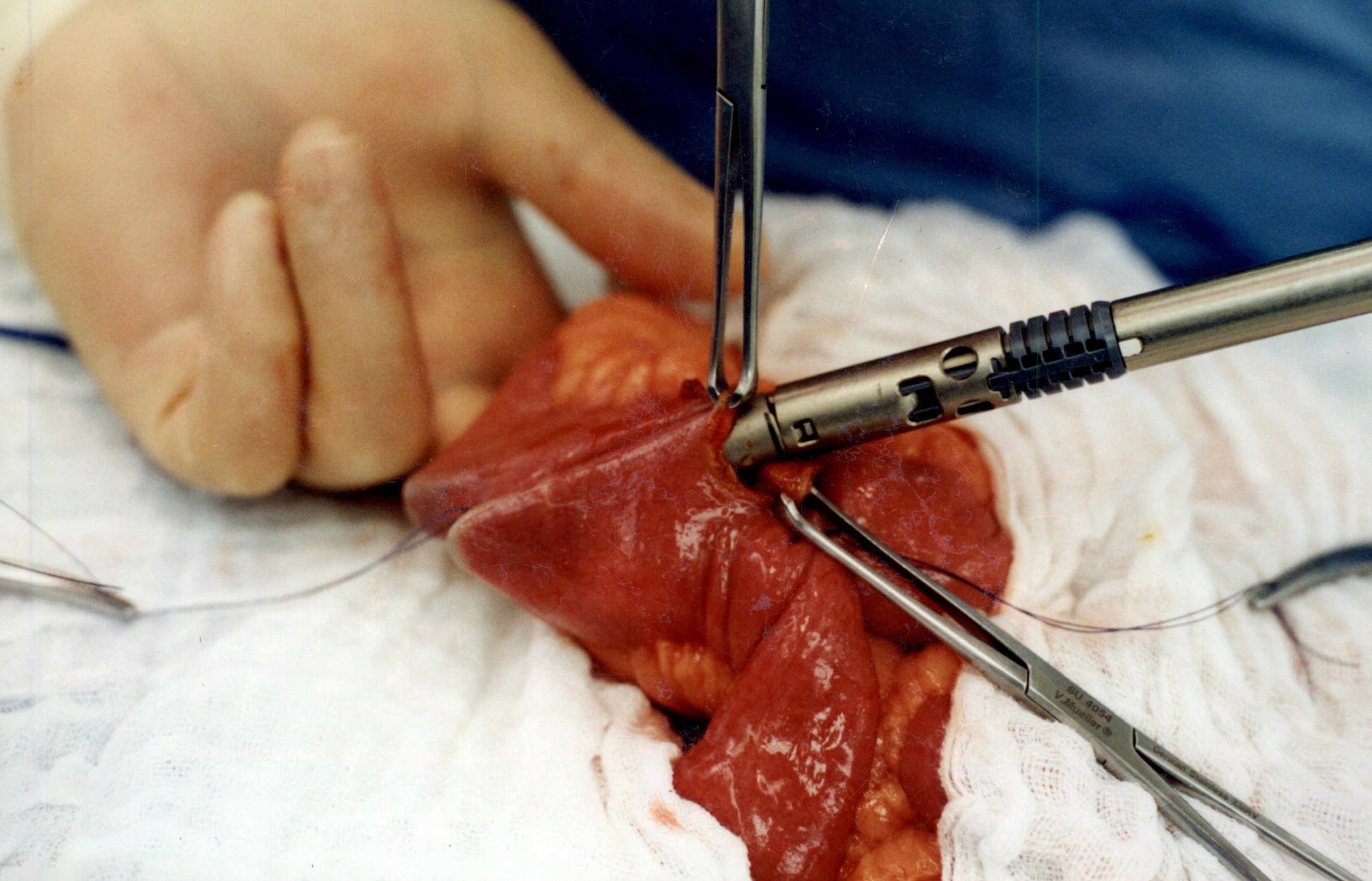
When the stapler is fired in opposite direction, a very wide anastomosis is created.
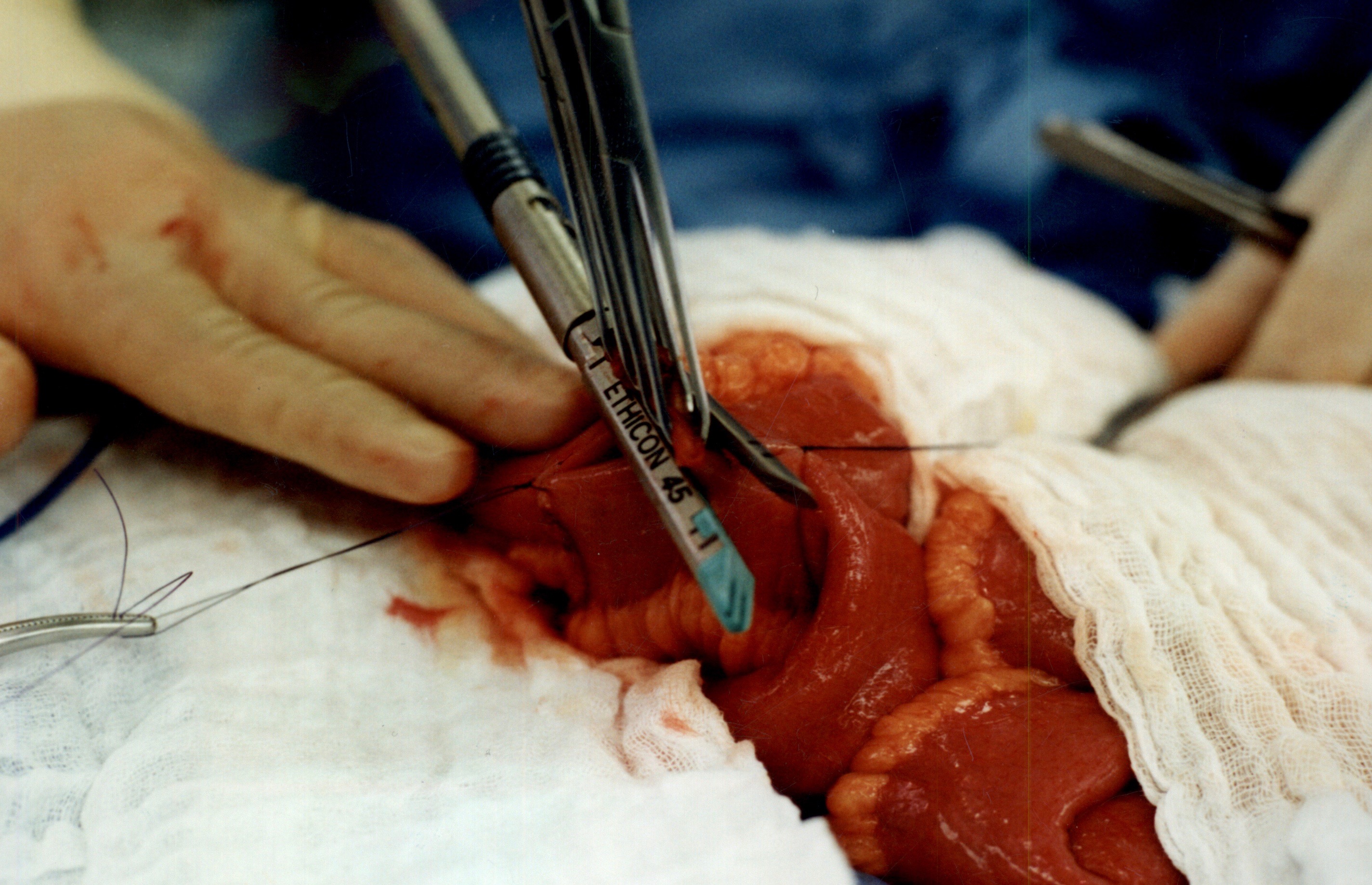
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Copper Deficiency Intravenous SupplementationExclusive Member Content
November 17, 2019 9:23 pm
Sleeve Gastrectomy Failure
May 07, 2019 12:53 pm
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
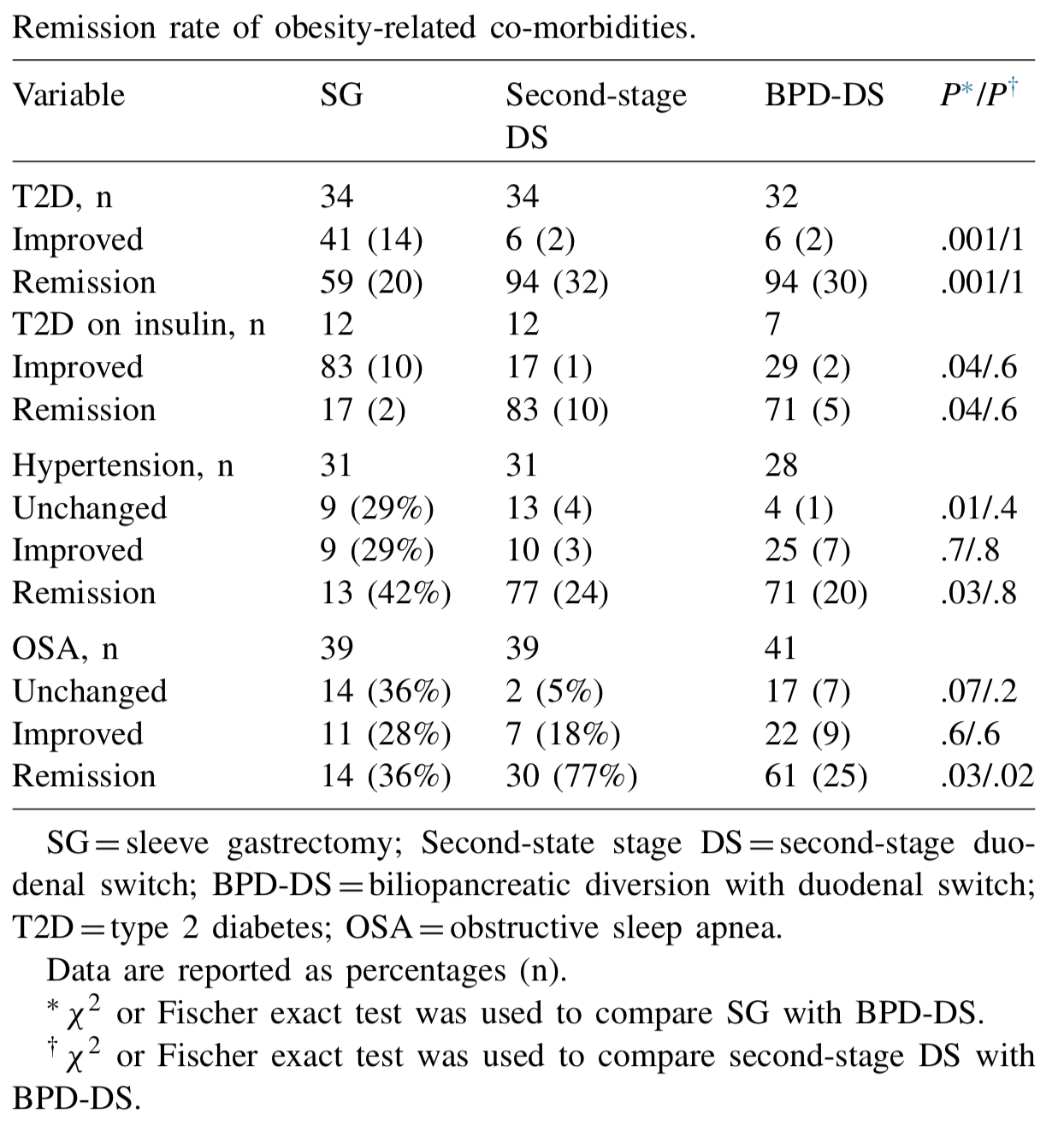
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss. 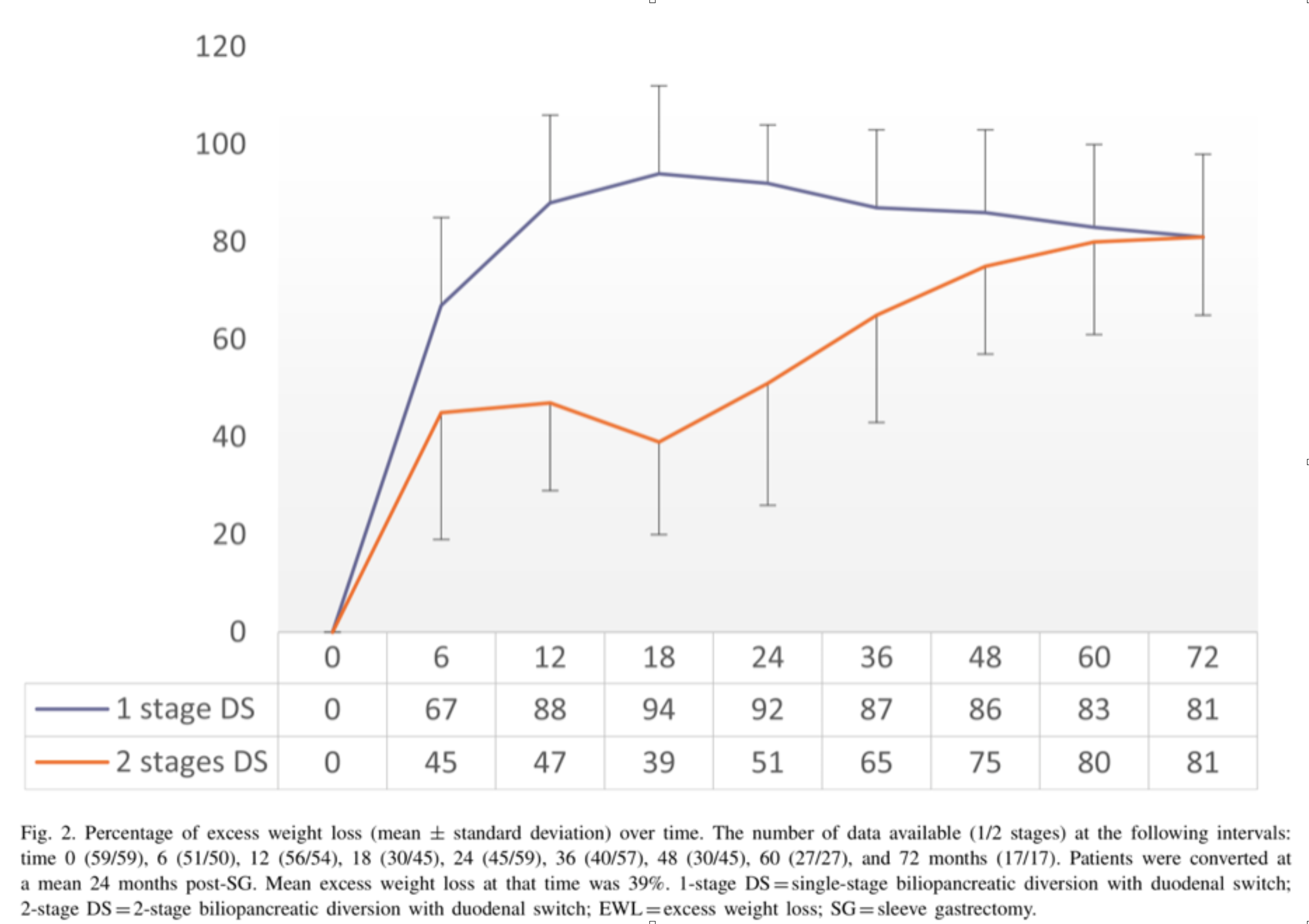
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.
Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP
Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium
New Pasadena Office Map and Parking
August 12, 2017 8:35 am
We’ve created a helpful map and parking diagram for our new Pasadena, CA office location. It also has a general layout of the Huntington Memorial Hospital Campus and Pre-operative intake and testing area. We hope that you find it helpful on your next visit to see Dr. Ara Keshishian, General and Bariatric Surgeon.

Dr. Ara Keshishian has performed more than 2,000 Duodenal Switch procedures, thousands of Sleeve Gastrectomies and more than 500 revisions from other Weight Loss Surgeries such as RNY Gastric Bypass, Adjustable Gastric Band, and Sleeve Gastrectomy to Duodenal Switch as well as General Surgical cases over the last 18 years of private practice.
Shared Success- Samantha had a Sleeve to Duodenal Switch Revision
July 14, 2017 9:30 am
After struggling with obesity for most of my life I was finally fed up. I had heard about weight loss surgeries before but was always under the common misconception that it was for people who wanted the “easy” way out of a hard situation. I had been working out and reducing calories and tried every popular diet and trainer you could think of. I was still huge and each time I would stop one of these extreme programs I would only end up larger than I was before.
My husband’s cousin had the sleeve surgery and she raved about it. Watching her success is what started to open my mind to surgery, but I was only considering the sleeve gastrectomy. I went to a center in another state that offers Duodenal switch, lapband, RNY and the sleeve. The surgeon I met with strongly suggested RNY to me, but I was stuck on the sleeve. I didn’t want my intestines touched period. I had the sleeve surgery on October 9, 2013.
My high weight was 402 lbs and I weighed 343 on the day of my sleeve surgery. I actually did well with the sleeve and was able to get down to 218 as my lowest. However it was still much like dieting. It was so stressful. After a while my body wouldn’t drop the weight regardless of how little I ate and exercised. I was eating 800-1200 calories a day and low fat meals and working out and kept slowly gaining weight. I was frustrated and honestly I gave up. My reflux wouldn’t go away so I visited a bariatric surgeon in my area who suggested that we essentially re-do the sleeve surgery to make my sleeve small again so that I would eat less and lose weight again. I got a second opinion and that surgeon suggested I revise to RNY. I went to obesity help’s website to explain my situation and a lot of people with much more experience than me HIGHLY urged me to see Dr Keshishian before making a decision. He was said to be an expert in revision weight loss surgery. I almost cancelled my appointment and didn’t have hope with this doctor either, but since I was in a dead end I went anyway. Dr Keshishian told me it wasn’t my fault. WHAT!? I had never heard that before. I usually get the shame from doctors who assume I must not be trying or that I am secretly eating something wrong. He ordered tests and told me it was “simply science” and I just LOVED him! I had a stricture in my Sleeve that needed to be repaired so since I needed surgery anyway I decided to go ahead and revise to a surgery that has the highest success rate, Duodenal Switch.


I was so scared of my intestines being cut and Dr. Keshishian eased my fears. I wish I had went that route the first time but then I might not appreciate it like I do now. Duodenal switch is the ONLY surgery I would recommend to anyone. As Dr K says it’s simple numbers. It’s the surgery with the highest percent of excess weight lost and kept off. I was 252 before my revision from Sleeve to Duodenal Switch and I am just at a year out and today I weigh in the low 190’s and I am still losing. Dr K’s goal for me was about 180. My goal is about 175. I eat more fat now than I ever did even when I was 400 lbs. I enjoy what I eat and I enjoy exercising and most of all I get to enjoy seeing results from my hard work. Food no longer causes me stress and anxiety. I know with 100% certainty that I made the right decision. Thank you Dr. K for your great skill and I don’t mean just with the knife but with the way you are able to make a high anxiety situation seem like no big deal.


Controversies of Duodenal Switch -Staged or Single Stage
September 27, 2014 5:29 pm
There is almost no science supporting the two staged duodenal switch. The “theory” advocated was that one can try a less invasive procedure and then if it does not work, proceed with the more complex operation. This was also advocated as a risk reduction tool for patient to have the sleeve component done as a planned first stage to reduce the operative and the anesthesia risk of the full duodenal switch operation. The “DS” surgeons soon recognized that the weight loss after sleeve is limited and not long lasting.
Laparoscopic Sleeve Gastrectomy has received a great deal of attention in the last few years. Most of this attention is contributed to the almost universal failure and high complication rate of the adjustable gastric banding (AGB) procedures. Since some practices and surgeons promised a low risk, minimally invasive procedure with the AGB procedures, they had to find an alternative as the complications and the failure of the AGB procedures mounted. This is when the Sleeve Gastrectomy started gaining more acceptance by surgeons who previously had performed AGB. Sleeve Gastrectomy is becoming one of the most commonly performed weight loss surgical procedure in several areas in the country and world.
It is worth mentioning, that Sleeve Gastrectomy is nothing new to the surgeons who perform Duodenal Switch procedures. Duodenal Switch has been performed as a single stage procedure since it’s inception.In fact every classical Duodenal Switch procedure is a Sleeve Gastrectomy with two small bowel anastomosis, first described by Dr. Hess in 1988. Duodenal Switch surgeons were also first to offer Sleeve Gastrectomy as the first stage of a two staged procedure.
BiliopancreaticDiversion-Duodenal Swtich: Independent Contributions of Sleeve Resection andDuodenal Exclusion, Marceu P, Biron S, Marceau S, et al. Conclusion: SG and DS independently contribute to beneficial metabolic outcomes after BPD-DS. Long-term weight loss and correction of metabolic abnormalities were better after DS favoring its use as first stage in BPD-DS; one-stage BPD-DS outcomes were superior to two-staged.
Other than some extreme cases, there is no indication to offer the sleeve as a staging operation since in vast majority of the cases the patient will require to have an alternative procedure done when the weight loss stops, and in some cases weight gain is experienced.
The reasons one should avoid a staged procedure is the evidence in the research data does not support that staging a procedure benefits the patient. There is also consideration for two general anesthesia exposures. Anesthesia time is based on surgical experience, technique and past patient surgical history. The argument that a patient should have the Sleeve Gastrectomy, to improve the risk for Duodenal Switch has almost no support in the peer-reviewed literature. One should also consider that a patient having had a Sleeve Gastrectomy may not qualify for the second stage Duodenal Switch procedure due to lower BMI or the insurance benefits mandating only one weight loss procedure in a lifetime.
There may be patients who may benefit from the Sleeve Gastrectomy long term, but in my opinion to offer Sleeve Gastrectomy as a planned first phase of the the duodenal switch is not indicated in majority of the cases.