
Category: Gastric Balloon
Gastric Balloon
March 12, 2019 9:10 am
Here we go again…. There is a new cure for obesity, Gastric Balloon, with minimal to no risk, is an outpatient procedure and/or can be done in the surgeons office with no anesthesia. Have we not similar claimed like this before (Adjustable gastric band) ?
Randomized sham-controlled trial of the 6-month swallowable gas-filled intragastric balloon system for weight loss published in Surgery for Obesity and Related Diseases 14 (2018) 1876–1889, by Sullivan et. al reports
“Conclusions: Treatment with lifestyle therapy and the 6-month swallowable gas-filled intragastric balloon system was safe and resulted in twice as much weight loss compared with a sham control, with high weight loss maintenance at 48 weeks.”
This sound very promising, however is very vague and leaves out significant, critical, and pertinent information.
The outcome of weight loss at 24 weeks was reported in Total Body weight loss % (TBWL%), Excess weight % (EWL), weight loss, and BMI change. Of those, the last three were statistically significant changes.
The outcome the weight loss was reported to be at 7% TBWL% at 24 weeks with some weight regain, with the patient employing post REMOVAL life style changes. 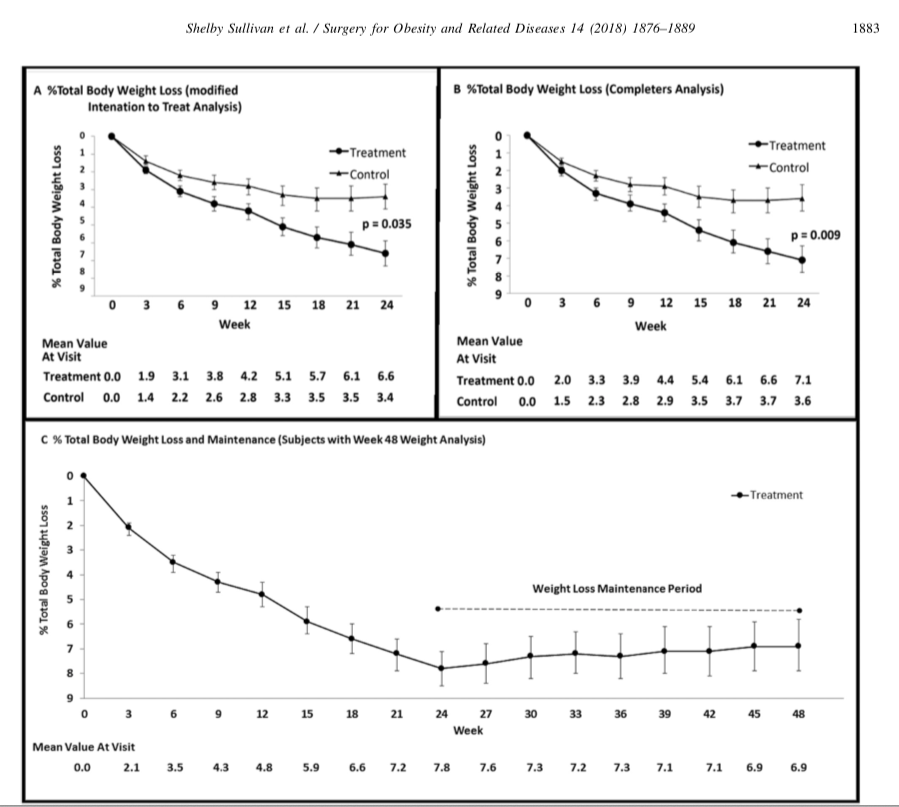
It is stated that the Gastric Balloon is temporary device that needs to be removed in 6 months and should be considered in low BMI patients (<35kg/m2). It is is important for those patients who are considering this temporary expensive measure for minimal weight loss to entertain the alternative of the same temporary results that may be obtained by lifestyle changes. These results may be maintained by a healthy lifestyle, exercise, and eating without the need for a device.
Does Size Matter
September 28, 2009 12:14 pm
The scientific basis for weight loss surgery, for the majority of the part relies on the premise that overeating and lack of exercise are the principal mechanisms contributing to the increase in the incidence of obesity over that last decade. Much has been said about our unhealthy life style that involves sedentary activity and immobility. Fast foods, high fat content meals, calorie dense food, are some of the examples of possible contributing factors to this health crisis.
The contrary position would be that there are other factors that contribute to obesity. These may include environmental factors, food preservatives, genetics, and exposures to toxins.
If one assumes that the over eating is the core problem, then you can also assume that the most successful operation will have the smallest stomach, since it will reduce the ability to over eat most drastically. This is where the scientific evidence does not support the theory and we all have to reassess the principal that the treatments are directed toward.
Recently there have been a number of studies that have been published in scientific journals that suggest size of the stomach or the pouch does not matter. So if obesity is the result of over eating then the operation that provides the smallest stomach must work the best. This argument should be true for the pouch size after gastric bypass, and the opening of the gastro-jejunostomy (connection between the stomach pouch and the small bowel connected to it after the gastric bypass, RNY operation). The same theory applies to the sleeve gastrectomy of the duodenal switch operation.
This argument that over eating and lack of exercise is the major contributing factor seems to be loosing ground.
The studies below are outline to demonstrate the disparity between the theory and the lack of scientific support for it.
1- Sanchez-Pernaute et.al. (Obesity Surgery, 17, 2007) reported that “After DS, gastric tube volume is not directly related to weight changes.” He proposed that there are other factors that may contribute to the weight loss than the size of the gastric tube.

This graph taken from the referenced study above shows that the size of the stomach sleeve does not correlate with the %EBWL in DS patients. The smaller stomach sleeve does not result in the more weight loss.
2- O’Connor et.al. (SOARD 4(2008)399-403) reported that “With construction of divided, vertical, lesser curve-based small-volume (=<20cm3) gastric pouches, the actual size of the gastric pouch did not correlate wit the %EBWL at 1 year after Laparoscopic, GB [gastric bypass]”.
3- Nishie et.al. (Obesity surgery, 17, 2007) concluded that “pouch size area, measured by routine UGI [upper GI series] on the first post operative day, does no influence short-term postoperative weight loss”.

This a sample of a number of graph that Nishie published in her study. The similar graphs were for 3, 12, and 24 months. They all had a flat line distributions. What they are showed was regardless of the time lapsed from surgery, the %EBWL was independent of the size of the pouch measured immediately post operatively.
4- Cottam et.al. (Obesity Surgery, 2009, 19:13-17) reported “The level of restriction or the presence of stenosis achieved by different circular stapler sizes does not have a significant role in weight loss”.

This study was focused on the size of the opening that is made between the stomach pouch and the small bowel in the gastric bypass (RNY) operation. The weight loss did not differ in the two groups of the patients. One group had a 21mm stapler and the other one 25mm stapler used. The weight loss, as measured by %EBWL was nearly identical in both cases.
In summary, the size does not seem to matter. The size of the stomach pouch, when it gets to a certain size in not important. The smaller stomach pouch or the narrower connection of the stomach and the small bowel will not make a patient loose more weight. Doesn’t this prove, to at least some degree, that there is much more to obesity than the simple notion of eating small portion and exercising?
- Weight loss Medications compared to surgery February 20, 2024
- SIPS-SADI and ASMBS December 31, 2023
- Survey December 16, 2023
- Long Term Outcome Survey December 1, 2023
- Weight Loss Injection May 10, 2023