Description:
Sphincter of Oddi Dysfunction (SOD) is a clinical syndrome characterized by biliary/ pancreatic pain from abnormal function or obstruction of the.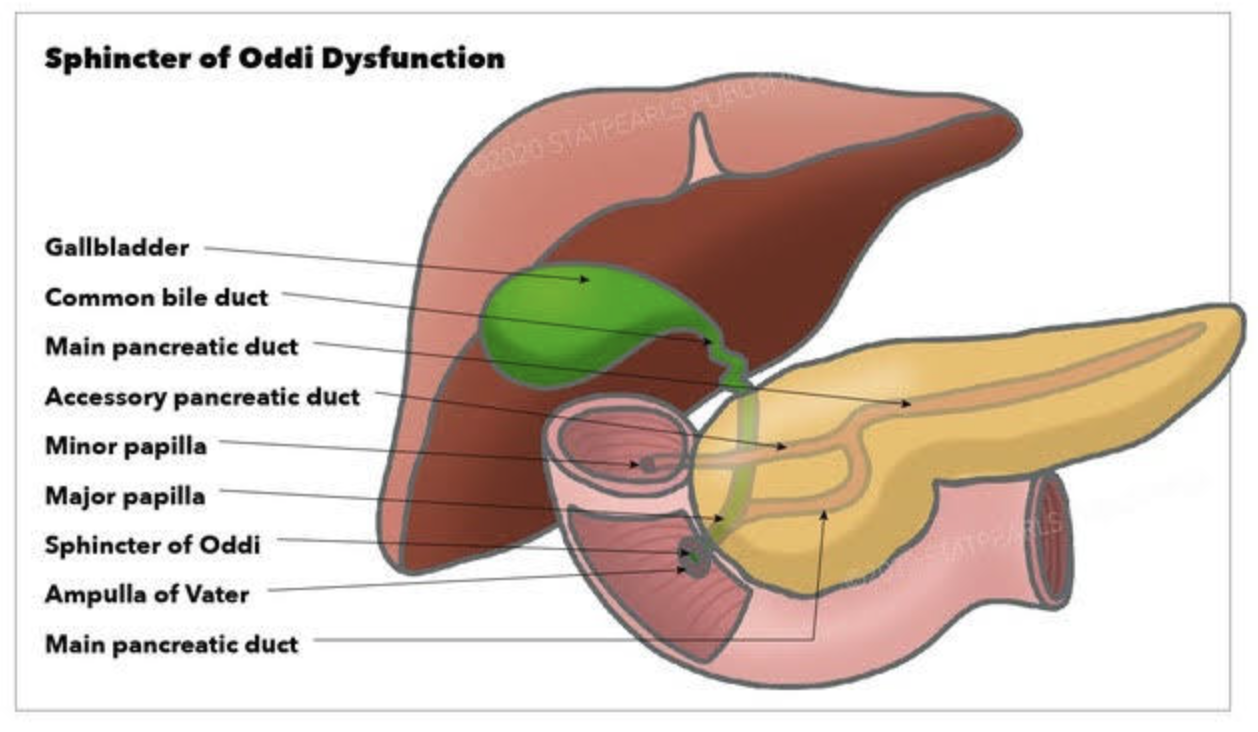
Diagnostic and classification
- The SOD spectrum includes biliary, pancreatic, or combined sphincter dysfunction, with symptoms driven by dyskinesia or mechanical obstruction. The term SOD encompasses both functional motility disorders (biliary or pancreatic sphincter dysfunction) and mechanical obstructions such as papillary stenosis.
- SOM has been considered the gold standard for diagnosing elevated basal sphincter pressure. It is invasive and carries complications, including pancreatitis. SOM can also not be done in those who have had gastric bypass or duodenal switch operations. Sphincterotomy outcome is not uniform. Consequently, many centers have moved toward empiric endoscopic therapy for appropriately selected patients and toward noninvasive or less invasive diagnostic approaches for others.
Treatment approaches
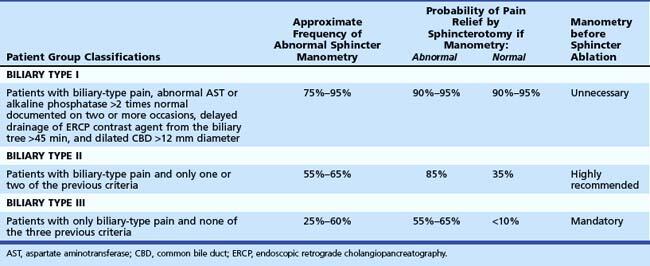
- Endoscopic biliary sphincterotomy (EST) is the most established nonpharmacologic treatment for biliary SOD, particularly in type I and many type II patients with objective ductal dilation and/or enzyme elevation.
- In type II SOD, outcomes after EST correlate with objective evidence of obstruction or sphincter hypertension on SOM. Empiric sphincterotomy without manometry is controversial.
- Type III SOD has emerged as predominantly functional pain rather than a mechanical obstacle. Alternative management emphasizes risk stratification, noninvasive strategies, and multidisciplinary approaches.
- Medical and non-sphincterotomy options (calcium-channel blockers, nitrates, antidepressants, and lifestyle modifications) have been discussed as potential adjuncts or alternatives.
Summary
- SOD is a multifactorial biliary and pancreatic sphincter disorder with a spectrum from mechanical obstruction to pure dyskinesia. Type I and II retain treatment relevance, particularly EST for biliary obstruction. Type II management requires clear identification of the cause.
- SOM is a diagnostic tool with significant limitations.
- Endoscopic sphincterotomy offers meaningful symptom relief in type I and select type II with objective obstruction. It carries a risk of complications, including pancreatitis; risk mitigation strategies are integral to practice. In type III SOD, sphincterotomy generally has limited benefit, necessitating a move toward noninvasive management and careful patient counseling. Patients post- gastric bypass, or duodenal switch, can not have ERCP or SOM done.
Leave a Reply