Tag: failed gastric bypass
Feeding Tube with Duodenal Switch
February 03, 2025 9:53 am
The surgical changes following the revision of the failed gastric bypass to the duodenal switch or a primary duodenal switch require an evident appreciation and understanding of the anatomy and physiology of placing a feeding tube and managing the nutritional status. There are different places where a feeding tube can be placed.
1-A feeding gastrostomy tube endoscopically cannot be placed because of the transected post-pyloric duodenum (The image viewed on a desktop or a laptop allows the scroller on the image to move)
2-An orogastric or nasogastric tube should only use an elemental feeding formula. This is because the food in the stomach is prevented from mixing with the biliopancreatic juices, which will not be adequately absorbed.
3-A feeding Jejunostomy can only be insured surgical post ligament of traits. This cannot be done endoscopically because duodenal switch transaction post pyloric small bowel to prevent mixing of the biliopancreatic secretion.
Additional informationLength of Bowel : Hess or No Hess
March 22, 2020 5:58 pm
“…What is the length of my common channel” is probably one of the frequently asked questions about the duodenal switch operation in the office. This usually comes up at the initial consult when patients repost credible sources such as Dr. Google and Dr. Facebook for patient with different bowel length have done well or not so after duodenal switch operation. Dr. Hess described the Duodenal Switch by using total bowel length measurements and creating the common channel as a percentage of the total small bowel length. However, it seems that this is being done less and less.
This leads to my explanation that is on the website
Hess calculator : Bowel Length Calculator
How the actual measurements matters: Bowel length video link
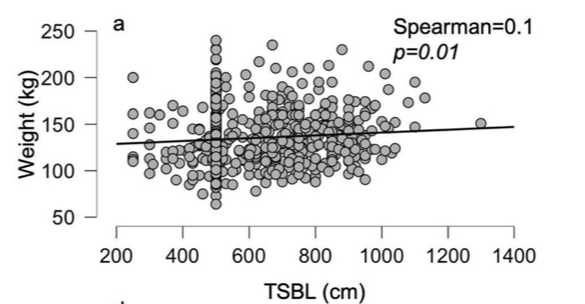
In 2019, Bekheit et.al published a very interesting study comparing total small bowel length (TSBL) to a number of variables such as height, weight, sex and BMI. They identified a few loose correlations. Male patient have longer TBSL than females. There was correlation between TSBL and height stronger in males than females but not statistically significant.
In Conclusion they reported ” Despite statistical significance of the correlation between the TSBL and the height and weight of the included participants, the correlation seems to have no clinical meaning since the effect size is negligible. ”
As I have previously discussed this Making the common and alimentary length standard for every duodenal switch patient will make some loose too much and other not enough weight.
Figure 1 shows TSBL on the horizontal axis, and height, weight, BMI and Age on the vertical axis. For the most part what they all show is that one can not predict how long a patients bowel is by any of the measures that we take in the office as a part of the routine exam.
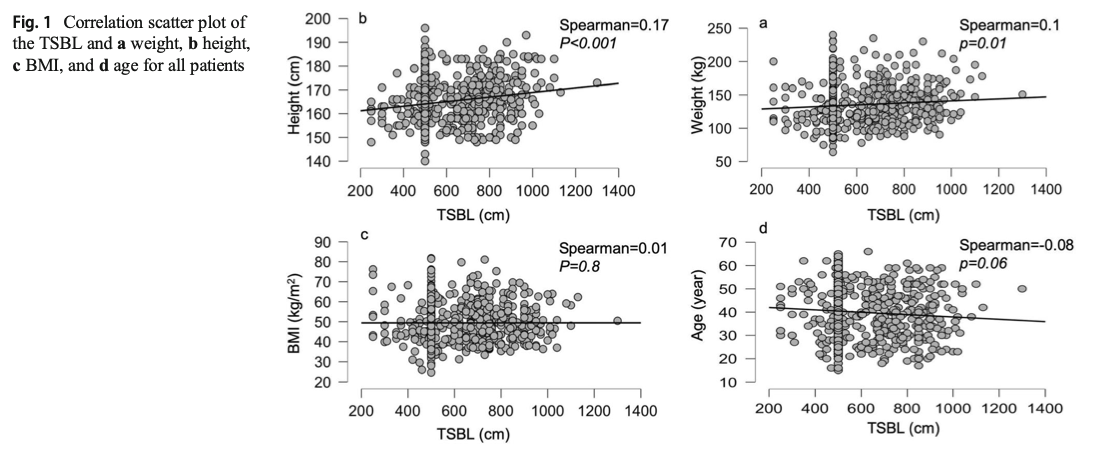
This raises, the concerns that I had raised previously. How could two similar patients who have the same weight, age, sex and BMI have the same surgery and expect the same result if one of them has TSBL of 400 cm and the other one 800cm?
Health Insurances Working Against You
July 09, 2018 12:01 pm
Are Health Insurances working against you? Especially in people who have the disease of obesity? Insurance companies continue to lengthen the pre-operative period. The time that is required to lapse has now in some cases been extended between 6-12 months for some commercial health plans. There are yet again studies that have shown no benefit to the patient with this mandated waiting periods imposed on the patients. Unfortunately, the patients need to challenge the health care insurance companies by the means of all options that may be available to them. This may include internal appeal to external evaluation by some state agency. There are numerous studies that show pre-operative dieting does not equal better weight loss or compliance.


Gas (Flatuence) GI upset
July 27, 2017 7:32 am
Following the Duodenal Switch operation, patients will have more frequent flatulence. The problem can get worse with specific dietary choices. A very simple way of looking at this would be that, in general, Carbohydrates contribute to gas and the fat contributes to causing loose bowel movements. Carbohydrate or gluten sensitivity can also increase stool production.There is a significant overlap of the effects of carbohydrates and fat intake and one has to remember that the symptoms of gas and loose stool can often accompany each other.
Weight Gain after Gastric Bypass
January 04, 2017 9:12 am
Weight loss surgical procedures have different long term results and some procedures have more dramatic weight loss than others. Some procedures also result in much more sustained and long term weight loss. Unfortunately, what may be not obvious is that the patient has very little control over the outcome of the surgery in most cases. IT is very easy to blame the patient for weight regain after weight loss surgery. However, it is important to remind ourselves that the long term data reporting outcomes of the surgical procedures in most cases, includes all patient population. All these studies include the most compliant and not so compliant patients. Comparison chart of outcomes of weight loss surgical procedures.

A larger percentage of gastric bypass patients will require revision for weight regain, or other problems. There is no evidence that the size of the pouch or the anastomosis between the pouch and the small bowel changes the weight regain outcomes. Yet, quite frequently I will see patient who have had gastric bypass revision for weight regain, by reducing the size of the pouch or the anastomosis. Here are some publications that support the notion that other than extreme dilation, the size of the pouch and the size anastomosis does not predict the outcome of the surgery. There is some correlation with the site of the pouch, anatsmosis and weight loss, but there is no correlation between the size of the pooch, the opening and the failure rate. This means that patient with smaller pouch do not have better long term outcome that the ones with larger pouch, only that the patient with smaller pouch or anatsmaosis will loose more weight.
“Influence of pouch and stoma size on weight loss after gastric bypass”
Weight regain after RNY Gastric Bypass may also be caused by a Gastro-gastric fistula, which is a new connection between the pouch and the remnant stomach. Here is further information on Weight Loss Surgery Revisions.
When considering a primary weight loss surgical procedure, be informed. Investigate all your options and consider the long term outcomes. This may mean investigating different weight loss surgical procedures on your own.
Don’t lose your Pyloric Valve over a Failed Gastric Sleeve
June 22, 2016 9:32 am
In my opinion, there are very few reasons to lose your Pyloric Valve after sleeve gastrectomy. Recently, I am hearing of people who have had regain due to a failed Sleeve Gastrectomy being revised to Gastric Bypass RNY and then seeking a Duodenal Switch due to regain from Gastric Bypass RNY. A better option is to go from Sleeve Gastrectomy to Duodenal Switch, due to the long term excess weight loss maintenance of Duodenal Switch. The benefit of the pyloric valve can not be taken lightly.
Let’s start by reminding ourselves as to how the Sleeve Gastrectomy has gained popularity. In the quest for a simple solution to the complex problem of obesity, adjustable gastric banding gained popularity only fail to deliver anything close with the results that were promoted and heavily marketed. The focus was then changed to another seemingly simple procedure, laparoscopic sleeve gastrectomy. For some surgeons this is a new procedure. Surgeons that had been doing the duodenal switch operation for decades, sleeve gastrectomy has not been a new procedure. Surgeons that just started doing sleeve gastrectomy as a stand alone procedure started experiencing complications of the sleeve gastrectomy, such as regain and are now looking for another option for these patients. This complication are even more frequent when they’re done following a failed adjustable gastric band procedures due to the metabolic issues after revising one weight loss surgery to another. A similar short sighted approach is also being promoted with SIPS/SADI procedures, which is significantly simpler to perform than the duodenal switch operation.


Laparoscopic sleeve gastrectomy has a predictable profile for weight loss. It will not have as good on the long-term success rate as a duodenal switch operation. Complications of the sleeve gastrectomy including reflux, stricture, fistula, inadequate weight loss which may warrant evaluation and possible intervention. In my opinion, as a surgeon who does the duodenal switch operation routinely, a sleeve gastrectomy requiring revision should almost never be revised to a gastric bypass. I have seen number of patient’s who have had an adjustable gastric banding which was revised to the sleeve gastrectomy then to a gastric bypass. We are contacted for a possible revision to Duodenal Switch operation because of the weight regain. One can argue that the patient should not have had the sleeve gastrectomy or gastric bypass. It is critical that the complexity of the disease of the obesity is clearly appreciated that it purely restrictive procedure will not yield the desirable outcome long-term.
Benefits of the Pyloric Valve:
The pylorus is the valve located at the end of the stomach. It controls the release of the liquid mixture of food from the stomach into the small intestine.
The body naturally regulates the passage of food, so food will stay in the stomach for a certain period of time. We believe it is very important to continue that feeling of fullness in between meals. As a result, one of the principle functions of the pyloric valve is to regulate the amount of food products released into the small intestine where they are absorbed. This helps prevent dumping syndrome and ulceration.
The bodies natural diameter of stomach, pyloric valve and small intestine is left intact. This elevates stretching of the stomas created by RNY Gastric Bypass.
Summary
These failed Sleeve Gastrectomies should be revised to Duodenal Switch unless there are overwhelming health issues that would require another option. I always suggest several opinions from different Bariatric Surgeon’s who do a variety of Weight Loss Surgeries before deciding which type of revision to proceed with.
Shared Success Story Update- Cyndi RNY to Duodenal Switch
June 06, 2016 6:37 am
Three Years Out Cyndi E … RNY to Duodenal Switch Revision
The Journey to get to the three year mark, has been amazing! And truly, The JOY is in the JOURNEY.
I am a JOYFUL “Third Time’s the Charm Revisionista”…. This is my new title…. And I say this proudly!!
For too many years (like 45! at least) I carried the shame and blame of being overweight and beat myself up on the inside. I tried everything, from age 13. I tried every diet, every program, and yes, I will say it, I have had THREE, yes THREE surgeries. And then, I let others convince me, and I bought into this, that I was a failure… BUT, I am not a failure. Surgery fails. For a long time, I could not say that, again with the SHAME word. BUT, I am done with shame, and I am done with blame. I no longer blame myself and I no longer shame myself or my body, because now, she and I, my body and I, are friends, and we are nice to each other.
Thankfully for me, I was in the right place at the right time, and met Dr. Ara Keshishian… My story with Dr. Keshishian, is simple. Dr. K was the first Doctor that did not blame me for my weight. He explained that each weight loss surgery has different measures of success, and percentages by weight loss surgery and outcomes. He educated me. He did not blame or shame me, he encouraged me. He also did an Endoscopy and found that I has a Gastro-Gastric Fistula. Simply put, this was an abnormal connection between the bypassed stomach and the small pouch created by the RNY Gastric Bypass surgery. Food could travel two ways, thus rendering the Gastric Bypass ineffective causing weight gain.



Dr. Keshishian performed my revision from RNY to Duodenal Switch on May 31, 2013. The procedure corrected my anatomy, enabling me to lose weight and regain my health. I have no complications, no issues post surgery.
Today, being a “Three Year Old” RNY to Duodenal Switch revisionista, I have a better perspective as a relative “newbie”. I am not a prisoner of my weight. I have lost 125-130 pounds, I am 5’12” (6 feet lol) 61 years old and for the first time in my life at a NORMAL WEIGHT! I do not fear, any longer, that I will gain my weight back. I am, however, mindful that I am consistent in my new habits and patterns that I have put in place, that keep me on track. I am also accountable. To myself, also to my Weight Loss Support Group, here in Paso Robles, to some fellow DS girlfriends that
I talk with about challenges, and with Dr. Keshishian. I am not held captive by my limitations, or my weight, and now I live with the possibilities each day brings and the fun challenges I put in front of me to conquer.
To the “newbies” I say, please take your time, treat yourself kindly, with your inner voice. This is not a race, this is a journey. Don’t rush, it’s ok to take it slow, listen to your body. And do not compare your journey to anyone else. You are you! You do you! You can do this well, one day at a time. Listen to the sage advice of those who went before you. We too have learned by trial and error. Be willing to sacrifice in the short term, for the gift of the long term life. Your DS is forgiving, you be forgiving as well!!!
Remember: WATER, PROTEIN, SUPPLEMENTS, EVERYTHING ELSE, EAT CLOSE TO THE DIRT, ELMO DIET
With JOY, Cyndi
2015 ASMBS Summary
November 11, 2015 7:31 am
The 2015 ASMBS meeting was held November 2-6, 2015. It was combined with TOS (The Obesity Society) and had more than 5,600 attendees from all over the world in every aspect of obesity treatment. There were some interesting additions and deletions from this meeting compared to the past.
The one sentence that comes to my mind is “I told you so”.
One important addition was a DS course for Surgeons and Allied Health. This was very exciting, except the content and questions seemed to gravitate to SADI/SIPS/Loop rather than DS. Dr. Cottam was one of the moderators of the course. It seems that they have found the value in preserving the pyloric valve. It was clear that the discussion was driven by the need to come legitimize the single anastomosis procedures at this early stage with almost no data to prove long term outcome. With many of the Vertical Sleeve Gastrectomies having re-gain and the they are looking for a surgery that the “masses” can perform. This was actually the term used by one of the presenters, implying that the duodenal switch needed to be simplified so that all surgeons, those who have pushed all other procedures can not offer Duodenal Switch to their patients with less than desirable outcome. Several surgeons also voiced their concern and dissatisfaction with the issues and complication of the RNY and want an alternative. There was much discussion regarding SADI/SIPS/Loop being investigational and that it shouldn’t be as it is a Sleeve Gastrectomy with a Billroth II. Dr. Roslin and Dr. Cottam discussed their SIPS nomenclature saying they wanted to stay away from something that had Ileostomy, suggesting bowel issues, or the word “SAD”i due to negative connotations. The point to be made is that the SADI and SIPS and the loop are all the same. I have also noticed other surgeons using SADS (Single Anastomosis Duodenal Switch). There is a great deal of industry behind these procedures and many surgeons being trained in courses funded by industry. One surgeon stood up and informed the entire course that they need to be clear with their patients about the surgery they are performing, as he had been in Bariatric chat rooms and there is upset within the community about SADI/SIPS/Loop being toted as “the same or similar to Duodenal Switch”.
There was also presenter who said “We are doing something new about every five years.” No, “we” are not. Some of us have stood by the surgery and techniques with the best long term outcomes and not gone with every “new” thing out there. The process of Duodenal Switch may have changes, open Vs. Lap, drains, location of incisions, post operative care and stay, but the tested procedure with the best outcome has been the duodenal switch operation and not the shortcut versions. Although, those of us that are standing by long term results seems to be in the minority. Why do I stand by Duodenal Switch? Because it works, when done correctly by making the length of the bowel proportional to the patient total bowel length, and height, and not just cookie cutter length for all patients, with the right follow-up, patient education, vitamin and mineral regime and eating habits.
A new addition was the Gastric Balloon, which in the research presented had a 60-70% re-gain rate and a no more than 10-15% weight loss one year only. This data represents more than 70% weight regain when the balloon is taken out. The Gastric Balloons can be left in between 4-6 months depending on the brand or type of balloon. The Gastric Balloon is not new to the Bariatrics and was first introduced in 1985. After 20 years and 3,608 patients the results were and average of 17.6% excess weight loss. It seems that we are re-gurgiating old procedures. There are many new medications that were front and center in this meeting.
The Adjustable Gastric Bands were missing from the exhibit hall this year. It is my hope and feeling from the other attendees that we may be seeing the era of the Adjustable Gastric Band being placed in patients come to an end. Although there are some still holding out that there are some patients that can do well with the Band.
Attending the 2015 ASMBS meeting this year, as it has every year, only reemphasized the importance of avoiding what has become the norm of chasing a simple solution that is fashionable and easy now. We stay convinced that the duodenal switch operation with the common channel and the alimentary length measured as a percentage of the total length is by far the best procedure with the proven track record. The patient should avoid the temptation of settling for an unproven procedure or device, because if history holds true, there will be a need for revision surgeries in the future.
Revision of a Sleeve Gastrectomy or RNY
August 31, 2015 6:32 am
These are examples of two types of patients referred to us for revision surgery.
The first example is a gastric bypass that we revise to the duodenal switch operation. The upper GI series after the revision, shows a “banana shaped” stomach, the pyloric valve and the duodo-ilesotomy anatomosis component of the duodenal switch.

The second example, images noted below, is that of a sleeve revised to the duodenal switch – both operations done at different institution. Note how the stomach is not a “banana shaped” and more like a funnel with a narrowing at the bottom of the stomach- a stricture.


Informed Surgical Consent
July 18, 2015 9:39 pm
Surgical informed consent is the document that summarizes the discussion that has been carried out between the treating physician and the patient. It also outlines the expectations as well as the potential complications of the treatment being proposed.
An informed consent should mean that the patient is absolutely clear as to the procedure agreed upon and that is reflected on the consent. No abbreviations are allowed on the consent forms. Clearly, there are instances when a physician or surgeon providing service may have to deviate from the proposed plan and agreed upon procedure on the consent because of unexpected findings in the operating room.
Any patient undergoing surgery should be acutely aware of the terminology and the language used. With regards to weight loss surgical procedures, RNY and GB is not acceptable because they are both abbreviations.
Duodenal Switch is a distinct well described procedure with its unique identifiable code (43845 for open procedure) that is recognized by hospitals, insurance companies and the surgical societies.
Duodenal Switch operation is not SADI, SIPS nor a loop Duodenal switch. Any attempt to interchanges these terms or operations is inaccurate the say the least.


A surgical informed consent is signed by the patient ( or the guardian) and the treating physician. This document however is reviewed and confirmed by all those involved in the patient’s care delivered in the hospital. The consent is reviewed by the admission staff when taking the patient for surgery, preoperative nursing and administrative staff, operating room circulating nurse as well as the anesthesia staff. One step most patients may not be aware is initiated after the general anesthesia is induced. The operating room staff, anesthesia staff and the operating physician all go through a set of checklist known as “Time out”.
“Time out” involves confirming the patient’s identification as well as the proposed procedure as the patient had discussed with the staff and confirming the consent.
It is imperative that a patient have complete understanding of their surgical options available to them and critical that they have full knowledge of the type of surgical procedure that has been consented to and performed.