Category: calcium deficiency
Bile Reflux Gastritis
May 19, 2026 4:13 pm
Hello, it’s best to clarify a few points:
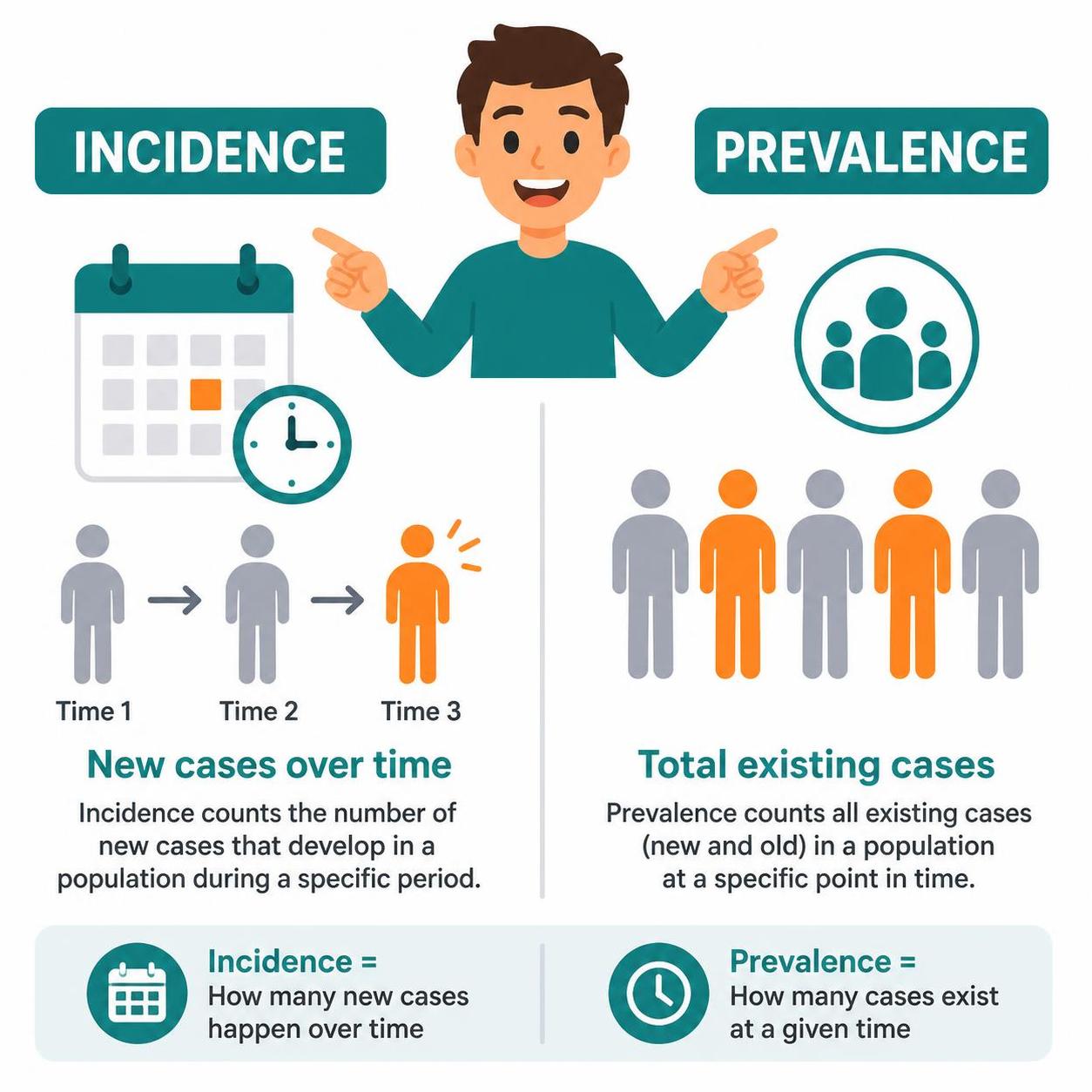
- The difference between prevalence and incidence.
- Incidence means new cases over
- Prevalence refers to existing cases at any time
- The difference between causation, coexistence, and correlation
- Causation refers to a condition causing an effect.
- Coincidence refers to two conditions present together at the same time, with neither causing the other.
- Correlation refers to two conditions that may occur together, with no causation.
- Study size refers to the research data on which the information is based. The larger the population size studied, the better the sample data and the more conclusive the results.
- Confounding factors.
Types of HyperParathyroidism
February 20, 2026 4:05 pm
There are 4 parathyroid glands which are located behind the thyroid gland, among other functions, are the main regulators of calcium, phosphorous, and magnesium in the blood. Elevations of parathyroid hormone (hyperparathyroidism) can be: 1-Primary, 2-Secondary, 3-Tertiary

Primary hyperparathyroidism means the parathyroid glands themselves are hyperactive. This may involve only one of the four glands: a) an adenoma, a benign tumor that needs surgical removal, or b) hyperplasia, when all 4 glands are hyperactive and/or enlarged, and in some cases, most of the 4 glands need to be removed.
Secondary hyperparathyroidism means that the elevated PTH level is caused by an external regulatory stimulus, such as low calcium, which itself may be due to low vitamin D, low calcium intake, or other causes.
Tertiary hyperparathyroidism is seen only in specific renal failure and transplant patients.
Regardless of the type of hyperparathyroidism, the end result is the same. Because the parathyroid gland aims to maintain normal calcium levels, it will do everything to achieve them. This includes increasing calcium absorption from the GI tract, breaking down bone to increase the blood calcium supply, and increasing calcium reabsorption from the urine.
Distinguishing between primary and secondary is critical, as primary is more likely than not a surgical problem that needs to be addressed. Secondly, it may be responding to metabolic deficiencies (low CA, low Vitamin D) that need to be corrected and take some time.
Not all cases require surgical intervention, as labs (vitamin D, calcium, and alkaline phosphatase) and imaging studies, such as neck ultrasound, CT scan, and Sestamibi scan, provide the information needed to dictate the treatment plan. Please stay up to date with your yearly lab results to catch changes sooner rather than later.
Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium
Bowel Length in Duodenal Switch
November 09, 2015 6:25 am
Malnutrition is one of the most feared complication of the duodenal switch operation. It may present years after surgery. What is common is a mix of nutritional deficiencies which include fat soluble vitamins, and protein calorie malnutrition. These all point to possible excessive shortening of the common channel. In my practice we have seen patients that have had lengthening of their common channel to improve their metabolic picture. What is very obvious to us, is that we see disproportionately higher number of cases coming to us for revision from practices where the common and alimentary lengths are done as a “standard” numbers with no specific adjustments made for the patient, their anatomy and situation. I have said for years, that the length of the bowel that is measured to be become the common and the alimentary limb should be a percentage of the total length of small bowel, rather than a pre-determined measurement. Here is a visual description of how this works.
If a common channel and the alimentary limb is measured to be a percent of the total length then the chance of protein calorie malnutrition is minimized since this will take into account the bowels absorptive capacity which is being reduced. This decrease in the absorption is done as a fraction of the total length.
Raines et al. published a study in 2014, that showed how small bowel length is related more closely to a patient’s height and not weight. And yet, some surgeons totally based the length of the common channel and the alimentary limb arbitrarily based on the patient pre operative BMI and nothing else. Could this be the cause of why I see some patients coming to us for revision of their duodenal switch for malnutrition?
Calcium – Revisited !Exclusive Member Content
October 05, 2015 8:06 am
August 6, 2014 Group Meeting Recap
August 08, 2014 6:35 pm
August’s group meeting/webinar topic was Vitamin D. Dr. Keshishian will be adding the voice over to the slides and it will be uploaded to when it’s completed. But in the meantime here are some highlights. Webinar here.
Vitamin D is a fat soluble vitamin has many important functions including bone health, cardiovascular health, blood glucose regulation, anti-cancer, anti-inflammatory, muscle function, respirator function, brain development and health, and immune function. There are several very large studies investigating other functions of Vitamin D. Vitamin D knowledge is in the midst of huge changes due to these upcoming studies.
Vitamin D metabolism is a complicated process whether via photo conversion in the skin or supplementation. Either way Vitamin D metabolism requires cholesterol to be converted to its active form. The fat-solubility is the primary reason for deficiency after Doudenal Switch, due to malabsorption of fat needed for conversion of Vitamin D. The Parathyroid gland helps to regulate absorption of Vitamin D. It is an inverse mechanism, meaning a high Parathyroid level signals more absorption of Vitamin D and calcium also.

Vitamin D deficiency is a World Health Organization priority. There are several causes some related to sunscreen use, disease processes, WLS, cola intake, diet related and medications. These can compound Vitamin D deficiencies.

Dr. Keshishian has new guide lines for Vitamin D levels. Due to the changing research regarding Vitamin D these guidelines are changing. There are some endocrinologists in Vitamin D research that are recommending even high standard of Vitamin D. DS patients should be well above the border of insufficient and sufficient due to underlining contributing facts for deficiencies and the lack of absorption. Parathyroid Hormone levels are inversely related. High PTH level can indicate Vitamin D deficiency and increase need for calcium. Calcium blood levels are not a good indicator of calcium or Vitamin D needs as the body is efficient at maintaining Calcium blood levels by breaking down bone mass due to the critic bodies need for circulating calcium.

Supplementation options are as follows: Please note that most over the counter Vitamin D is not appropriate for DS absorption. DS patients need to take “Dry” water miscible Vitamin D3. Please see the previous blog post regarding https://blog.dssurgery.com/2013/08/vitamin-d-and-dry-water-soluble.html for more information and pictures of this type of Vitamin D. Vitamin D is tied to several other nutrients for metabolism such as protein, calcium, magnesium, zinc and potassium. Treatment for correcting iron deficiency and phosphorus intake counter act Vitamin D absorption as do other previous discussed dietary issues. Take oral Vitamin D supplements even if you are receiving injectable Vitamin D.

Be proactive in Vitamin D supplements by monitoring your yearly DS laboratory studies. Please call the office with any questions. If in need of Vitamin D injections please see the previous blog post for related research article and compounding pharmacies. Vitamin D injections are not common place.
Please take the Vitamin D injections post to your treating physician if you are unable to see Dr. Keshishian and are in need of Vitamin D injections. If your treating physician has any questions please let them know Dr. Keshishian is available to answer their questions.
Our food selections for the meeting where all high Vitamin D recipes. Tuna stuff mushroom (Tuna for Vitamin D and mushrooms are a good source of zinc), crustless artichoke and spinach quiche ignore the part of the recipe for the crust and just bake in pie plate without the crust, Panna cotta with a strawberry balsamic compote and toasted flax seed and hemp hulls. The panna cotta is made with milk or almond milk and gelatin which are all important in bone health. Hemp hulls are a protein source as is the milk.
Strawberry Balsamic Compote taken from https://nomnompaleo.com
1/4 C balsamic Vinegar
2C hulled strawberries, thinly sliced
2 TBSP honey
1 TBSP fresh lemon juice
1tsp vanilla extract
1/4 tsp salt
In a sauce pan heat Balsamic vinegar until reduced by half and is a thick syrup. Add the rest of ingredients and simmer over medium heat for 5-10 minutes. Remove pan from heat and use an immersion blender to puree some of the sauce. The texture is to your liking, so puree as much or as little as you would like. Store in a sealed container for up to a week or you can freeze it for long term storage. This site also has a almond milk Panna Cotta but this is not the recipe use at the group meeting.
Panna Cotta Recipe
1/2 C 2% milk mix with 2 1/2 tsp of unflavored gelatin in a bowl to rehydrate the gelatin let sit for 5-10 minutes
In a medium saucepan mix
3 C 2% milk or whole milk
one vanilla bean split in half or 1 tsp vanilla extract
2 TBSP maple syrup
1 tsp salt
heat until steaming but not boiling, about 5-7 minutes. Take off heat.
Mix 1/4C greek style yogurt into the milk and rehydrated gelatin. Then whisk about 1 C of hot milk mixture into the gelatin/milk. Add this mixture into pan of hot milk and whisk well. Pour hot Panna Cotta mixture into ramekins. Refrigerate until set, about 2 hours.
In a small frying pan toast 2 TBSP Flax seed and mix with 2 TBSP hemp hulls. Before serving top with Strawberry Balsamic Compote and flax seed/hemp seed mixture to your taste.
Vitamins And Minerals
March 29, 2014 5:26 pm
|
Vitamins -Minerals |
Function |
Source |
Problems with deficiency |
|
B1 (Thiamine) |
Carbohydrate conversion, breaks down fats and protein, digestion, nervous system, skin, hair, eyes, mouth, liver, immune system |
Pork, organ meats, whole grain and enriched cereals, brown rice, wheat germ, bran, brewer’s yeast, blackstrap molasses |
Heart, age-related cognitive decline, Alzheimer’s, fatigue |
|
B2 (Riboflavin) |
Metabolism, carbohydrate conversion, breaks down fat and protein, digestion, nervous system, skin, hair, eyes, mouth, liver, antioxidant |
Brewer’s yeast, almonds, organ meats, whole grains, wheat germ, mushrooms, soy, dairy, eggs, green vegetables |
Anemia, decreased free radical protection, cataracts, poor thyroid function, B6 deficiency, fatigue, elevated homocysteine |
|
B3 (Niacin) |
Energy, digestion, nervous system, skin, hair, eyes, liver, eliminates toxins, sex/stress hormones, improves circulation |
Beets, brewer’s yeast, meat, poultry, organ meats, fish, seeds, and nuts |
Cracking, scaling skin, digestive problems, confusion, anxiety, fatigue |
|
B5 (Pantothenate) |
RBC production, sex and stress-related hormones, immune function, healthy digestion, helps use other vitamins |
Meat, vegetables, whole grains, legumes, lentils, egg yolks, milk, sweet potatoes, seeds, nuts, wheat germ, salmon |
Stress tolerance, wound healing, skin problems, fatigue |
|
B6 (Pyridoxine) |
Enzyme protein metabolism, RBC production, reduces homocysteine, nerve and muscle cells, DNA and RNA, B12 absorption, immune function |
Poultry, tuna, salmon, shrimp, beef liver, lentils, soybeans, seeds, nuts, avocados, bananas, carrots, brown rice, bran, wheat germ, whole grain flour |
Depression, sleep and skin problems, elevated homocysteine, increased heart disease risk |
|
B12 (Cobalamin) |
Healthy nerve cells, DNA/RNA, RBC production, iron function |
Fish, meat, poultry, eggs, milk and milk products |
Anemia, fatigue, constipation, loss of appetite, weight, numbness and tingling in the hands ad feet, depression, dementia, poor memory, oral soreness |
|
Biotin |
Carbs, fat, and amino acid metabolism (the building blocks of protein) |
Salmon, meats, vegetables, grains, legumes, lentils, egg yolks, milk, sweet potatoes, seeds, nuts, wheat germ |
Depression, nervous system, premature graying, hair, skin |
|
Folate |
Mental health, infant DNA/RNA, adolescence and pregnancy, with B12 to regulate RBC production, iron function, reduce homocysteine |
Supplementation, fortified grains, tomato juice, green vegetables, black-eyed peas, lentils, beans |
Anemia, immune function, fatigue, insomnia, hair, high homocysteine, heart disease |
|
Eyes, immune function, skin, essential cell growth and development |
Milk, eggs, liver, fortified cereals, orange or green vegetables and fruits |
Night blindness, immune function, zinc deficiency, fat malabsorption |
|
|
Calcium and phosphorus levels, calcium absorption, bone mineralization |
Sunlight, milk, egg yolk, liver, fish |
Osteoporosis, calcium absorption, thyroid |
|
|
Vitamin E |
Antioxidant, regulates oxidation reactions, stabilizes cell membrane, immune function, protects against cardiovascular disease, cataracts, macular degeneration |
Wheat germ, liver, eggs, nuts, seeds, cold pressed vegetable oils, dark leafy greens, sweet potatoes, avocado, asparagus |
Skin, hair, rupturing of red blood cells, anemia, bruising, PMS< hot flashes, eczema, psoriasis, cataracts, wound healing, muscle weakness, sterility |
|
Calcium |
Bones, teeth, helps heart, nerves, muscles, body systems work properly, needs other nutrients to function |
Dairy, wheat/soy flour, molasses, brewer’s yeast, Brazil nuts, broccoli, cabbage, dark leafy greens, hazelnuts, oysters, sardines, canned salmon |
Osteoporosis, osteomalacia, osteoarthritis, muscle cramps, irritability, acute anxiety, colon cancer risk |
|
Chromium |
Assists insulin function, increased fertility, carbohydrate/fat metabolism, essential for fetal growth/development |
Supplementation, brewer’s yeast, whole grains, seafood, green beans, broccoli, prunes, nuts, potatoes, meat |
Metabolic syndrome, insulin resistance decreased fertility |
|
Magnesium |
300 biochemical reactions, muscle/nerve function, heart rhythm, immune system, strong bones, regulates calcium, copper, zinc, potassium, vitamin D |
Green vegetables, beans & peas, nuts and seeds, whole unprocessed grain |
Appetite, nausea, vomiting, fatigue, numbness, tingling, cramps, seizures, personality changes, heart rhythm, heart spasms |
|
Selenium |
Antioxidant, works with vitamin E, immune function, prostaglandin production |
Brewer’s yeast, wheat germ, liver, butter, cold water fish, shellfish, garlic, whole grains, sunflower seeds, Brazil nuts |
Destruction to heart/pancreas, sore muscles, fragility of red blood cells, immune system |
|
Zinc |
Supports enzymes, immune system, wound healing, taste/smell, DNA synthesis, normal growth & development during pregnancy, childhood adolescence |
Oysters, red meat, poultry, beans, nuts, seafood, whole grains, fortified breakfast cereals, and dairy |
Growth retardation, hair loss, diarrhea, impotence, eye & skin lesions, loss of appetite, taste, weight loss, wound healing, mental lethargy |
|
COQ10 |
Powerful antioxidant, stops oxidation of LDL cholesterol, energy production, important to heart, liver, and kidneys |
Oily fish, organ meats, and whole grains |
Congestive heart failure, high blood pressure, angina, mitral valve prolapsed, fatigue, gingivitis, immune system stroke, cardiac arrhythmias |
|
Carnitine |
Energy, heart function, oxidize amino acids for energy, metabolize ketones |
Red meat, dairy, fish, poultry, (fermented soybeans), wheat, asparagus, avocados, peanut butter |
Elevated cholesterol, liver function, muscle weakness, reduced energy, impaired glucose control |
|
N-Acetyl Cystein (NAC) & Glutathione |
Glutathione production, lowers homocysteine, lipoprotein, heal lungs, inflammation, decrease muscle fatigue, liver detoxification, immune function |
Meats, ricotta, cottage cheese, yogurt, wheat germ, granola, and oat flakes |
Free radical overload, elevated homocysteine, cancer risk, cataracts, macular degeneration, immune function, toxin elimination |
|
Alpha Lipoic Acid |
Energy, blood flow to nerves, glutathione levels in brain, insulin sensitivity, effectiveness of vitamins C, E, antioxidants |
Supplementation, spinach, broccoli, beef, brewer’s yeast, some organ meats |
Diabetic neuropathy, reduced muscle mass, atherosclerosis, Alzheimer’s, failure to thrive, brain atrophy, high lactic acid |
What does elevated Alkaline Phosphatase level mean?
March 18, 2014 2:17 am
There are laboratory studies that can distinguish between 2 primary sources of the ALP. The two “isoenzymes” are bone ALP and liver ALP.
Injectable Vitamin A and Vitamin D
June 20, 2013 11:24 pm
Injectable Vitamin A and Vitamin D can improve vitamin status post weight loss surgery. One of the common side effect of all weight loss surgical procedures is nutritional and/or mineral deficiencies. Patients undergoing weight loss surgical procedures are always instructed to supplement their diet with multivitamin, calcium, iron, vitamin D and other supplements or minerals. If you do not take your supplements regularly you can become deficient. The symptoms associated with vitamin A deficiency is night blindness. Chronic vitamin D deficiency may result in low calcium, osteoporosis and other health-related issues.
Vitamin A and vitamin D, both fat-soluble vitamins, are absorbed by duodenal switch patients only if taken and a dry formulation. An alternative to oral supplement, would be injectable form of these two vitamins. Both of these vitamins can be formulated and purchased from compounding pharmacies that are equipped and experienced with the interpretation of injectable vitamins and minerals. Your primary care WILL need to contact the pharmacy of their choice for the recommendations and be willing to make the injections available to you.
We will gladly be able to provide injectable Vitamin A and Vitamin D for patients whose data laboratory studies are available to us and see us in the office.Please be aware that these are compounded and are not covered by insurance.
We will not be able to provide prescriptions for injectable vitamins to be sent to your primary care or other physicians to provide the injections.
Vitamin D supplement has been discussed previously in my Blog .
The common dosing for the vitamin D is 600,000 IU, deep IM every 6 months till the levels are normalized. The patient then can take the oral supplements only.
Vitamin A supplements was also discussed in my Blog.


The common dosing for the vitamin D is 100,000 IU, deep IM every 2-6 months till the levels are normalized. The patient then can take the oral supplements only.
Vitamin A supplements was also discussed in my Blog.
The common dosing for injectable vitamin A is 50,000 IU, deep IM every 6 months till the blood levels are corrected, and the patient symptoms are resolved.
Just as a reminder, we have no financial interest in any of the vendors that are recommended on our website. Also, note that this is not in any form or fashion a substitute for an evaluation by your primary care physician or your surgeon. This is for information only, and is not to be taken as a recommendation for any particular patients’ condition.
Absorption of Minerals and Metals
January 12, 2009 6:42 am
The vast bulk of mineral absorption occurs in the small intestine. The best-studied mechanisms of absorption are clearly for calcium and iron, deficiencies of which are significant health problems throughout the world.
Minerals are clearly required for health, but most also are quite toxic when present at higher than normal concentrations. Thus, there is a physiologic challenge of supporting efficient but limited absorption. In many cases intestinal absorption is a key regulatory step in mineral homeostasis.
Calcium
The quantity of calcium absorbed in the intestine is controlled by how much calcium has been in the diet during recent periods of time. Calcium is absorbed by two distinct mechanism, and their relative magnitude of importance is set by dietary calcium “history”:.

- Active, transcellular absorption occurs only in the duodenum when calcium intake has been low. This process involves import of calcium into the enterocyte, transport across the cell, and export into extracellular fluid and blood. Calcium enters the intestinal epithelial cells through voltage insensitive channels and is pumped out of the cell via a calcium- ATPase.The rate limiting step in transcellular calcium absorption is transport across the epithelial cell, which is greatly enhanced by the carrier protein calbindin, the synthesis of which is totally dependent on vitamin D.
- Passive, paracellular absorption occurs in the jejunum and ileum, and, to a much lesser extent, in the colon when dietary calcium levels have been moderate or high. In this case, ionized calcium diffuses through tight junctions into the basolateral spaces around enterocytes, and hence into blood. Such transport depends on having higher concentrations of free calcium in the intestinal lumen than in blood. Additional Calcium information here.
Phosphorus
Phosphorus is predominantly absorbed as inorganic phosphate in the upper small intestine. Phosphate is transported into the epithelial cells by contransport with sodium, and expression of this (or these) transporters is enhanced by vitamin D.
Iron
Iron homeostasis is regulated at the level of intestinal absorption, and it is important that adequate but not excessive quantities of iron be absorbed from the diet. Inadequate absorption can lead to iron-deficiency disorders such as anemia. On the other hand, excessive iron is toxic because mammals do not have a physiologic pathway for its elimination. Iron is absorbed by villus enterocytes in the proximal duodenum. Efficient absorption requires an acidic environment, and antacids or other conditions that interfere with gastric acid secretion can interfere with iron absorption.
Ferric iron (Fe+++) in the duodenal lumen is reduced to its ferrous form through the action of a brush border ferrireductase. Iron is the co-transported with a proton into the enterocyte via the divalent metal transporter DMT-1. This transporter is not specific for iron, and also transports many divalent metal ions.

Once inside the enterocyte, iron follows one of two major pathways. Which path is taken depends on a complex programming of the cell based on both dietary and systemic iron loads:
- Iron abundance states: iron within the enterocyte is trapped by incorporation into ferritin and hence, not transported into blood. When the enterocyte dies and is shed, this iron is lost.
- Iron limiting states: iron is exported out of the enterocyte via a transporter (ferroportin) located in the basolateral membrane. It then binds to the iron-carrier transferrin for transport throughout the body.
Iron in the form of heme, from ingestion of hemoglobin or myoglobin, is also readily absorbed. In this case, it appears that intact heme is take up by the small intestinal enterocyte by endocytosis. Once inside the enterocyte, iron is liberated and essentially follows the same pathway for export as absorbed inorganic iron. Some heme may be transported intact into the circulation. Additional Iron information here.
Copper
There appear to be two processes responsible for copper absorption – a rapid, low capacity system and a slower, high capacity system, which may be similar to the two processes seen with calcium absorption. Many of the molecular details of copper absorption remain to be elucidated. Inactivating mutations in the gene encoding an intracellular copper ATPase have been shown responsible for the failure of intestinal copper absorption in Menkes disease. A number of dietary factors have been shown to influence copper absorption. For example, excessive dietary intake of either zinc or olybdenum can induce secondary copper deficiency states. Additional Copper information here.
Zinc
Zinc homeostasis is largely regulated by its uptake and loss through the small intestine. Although a number of zinc transporters and binding proteins have been identified in villus epithelial cells, a detailed picture of the molecules involved in zinc absorption is not yet in hand. Intestinal excretion of zinc occurs via shedding of epithelial cells and in pancreatic and biliary secretions. A number of nutritional factors have been identified that modulate zinc absorption. Certain animal proteins in the diet enhance zinc absorption. Phytates from dietary plant material (including cereal grains, corn, rice) chelate zinc and inhibit its absorption. Subsistence on phytate-rich diets is thought responsible for a considerable fraction of human zinc deficiencies. Additional Zinc Information here