Tag: SADI
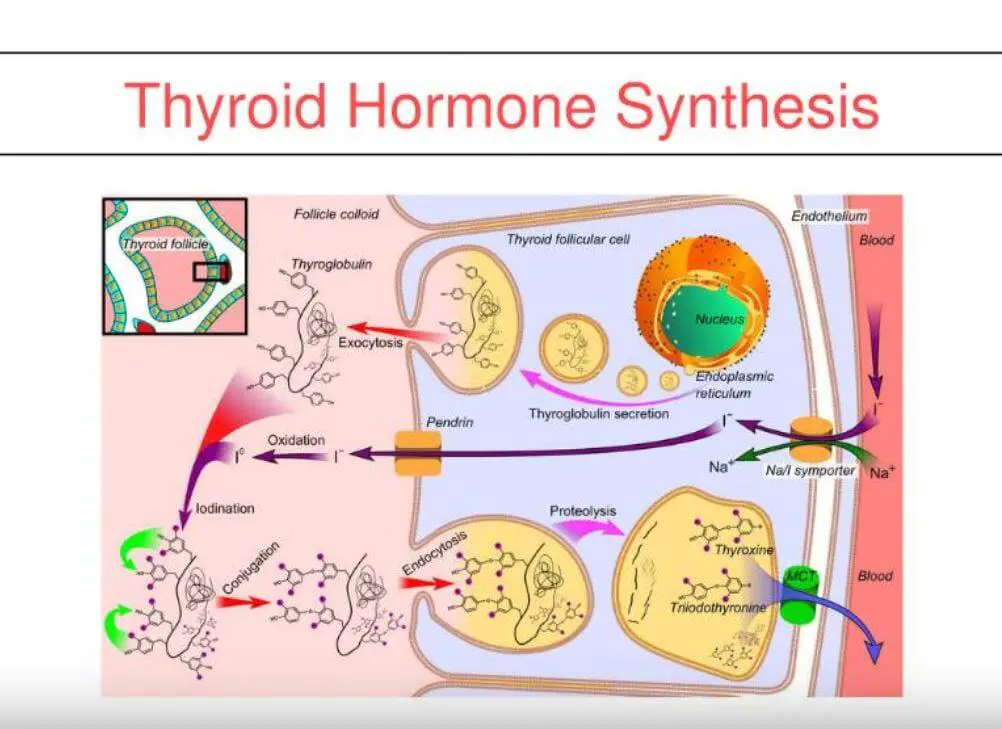
Thyroid Medication Absorption And Weight Loss Surgery
June 10, 2019 8:59 am
Question : “Do I have to take higher dose of thyroid medication after the duodenal switch? ”
Answer : “Maybe”
With all weight loss surgical procedures, there may be changes to absorption of medications. It is easily understood why duodenal switch may results in decreased absorption of fat-soluble medication. What is not as clear is the reduction in absorption of other medication with procedures that do not explicitly change the absorption at the level of the small bowel directly.
The research data is all over on this topic. There is published literature that shows improvement in the thyroid function after gastric bypass and the sleeve gastrectomy. However, the exact mechanism is not completely understood.
There is research that reports “…decreased postoperative levothyroxine requirements.” Other have shows no correlation between the length of the bowel distal to duodenum to absorption of thyroid medication.
With all this confusing data, the best course would be to always “treat the patient and not the lab results.”
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
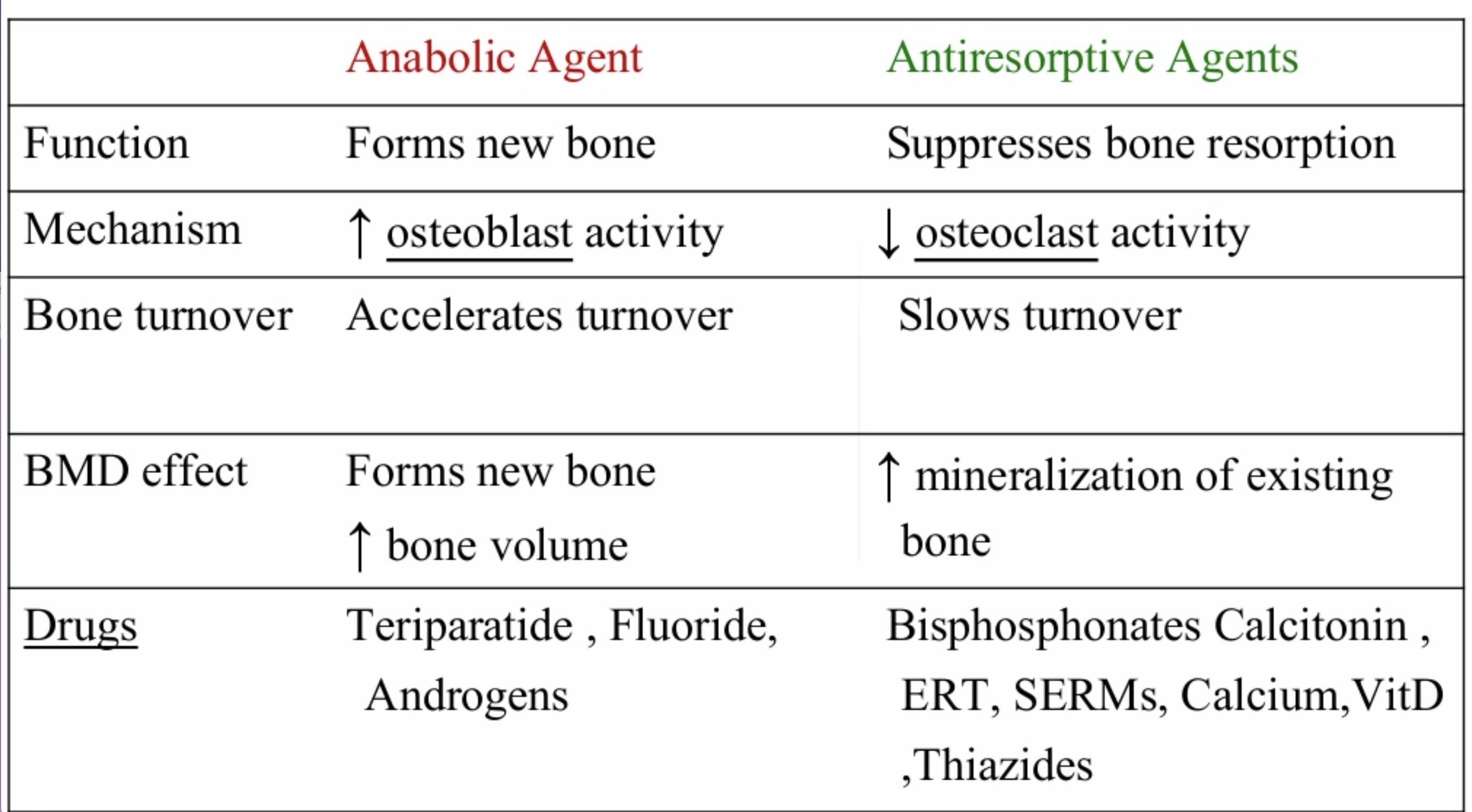
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
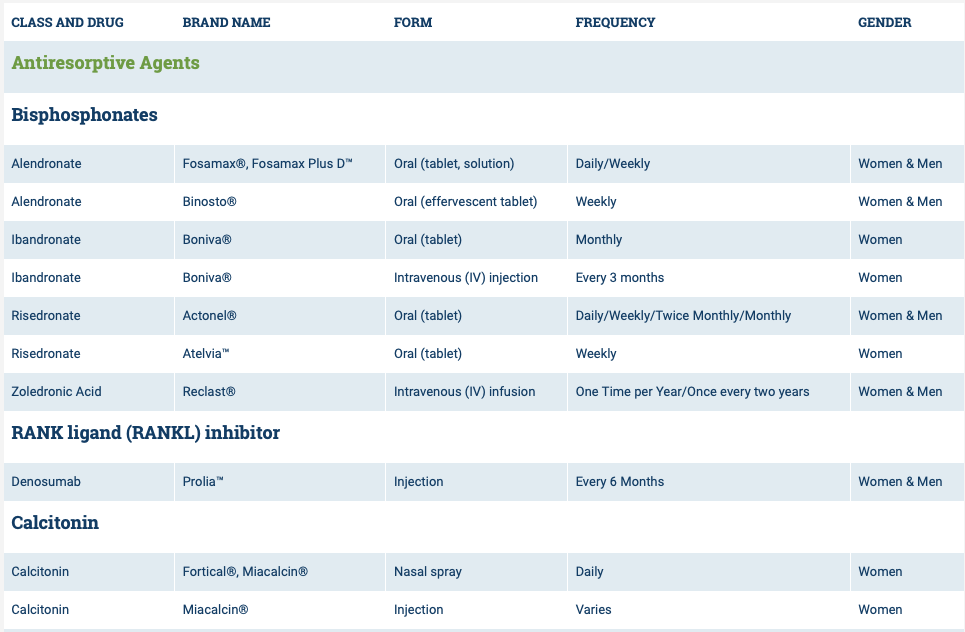
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

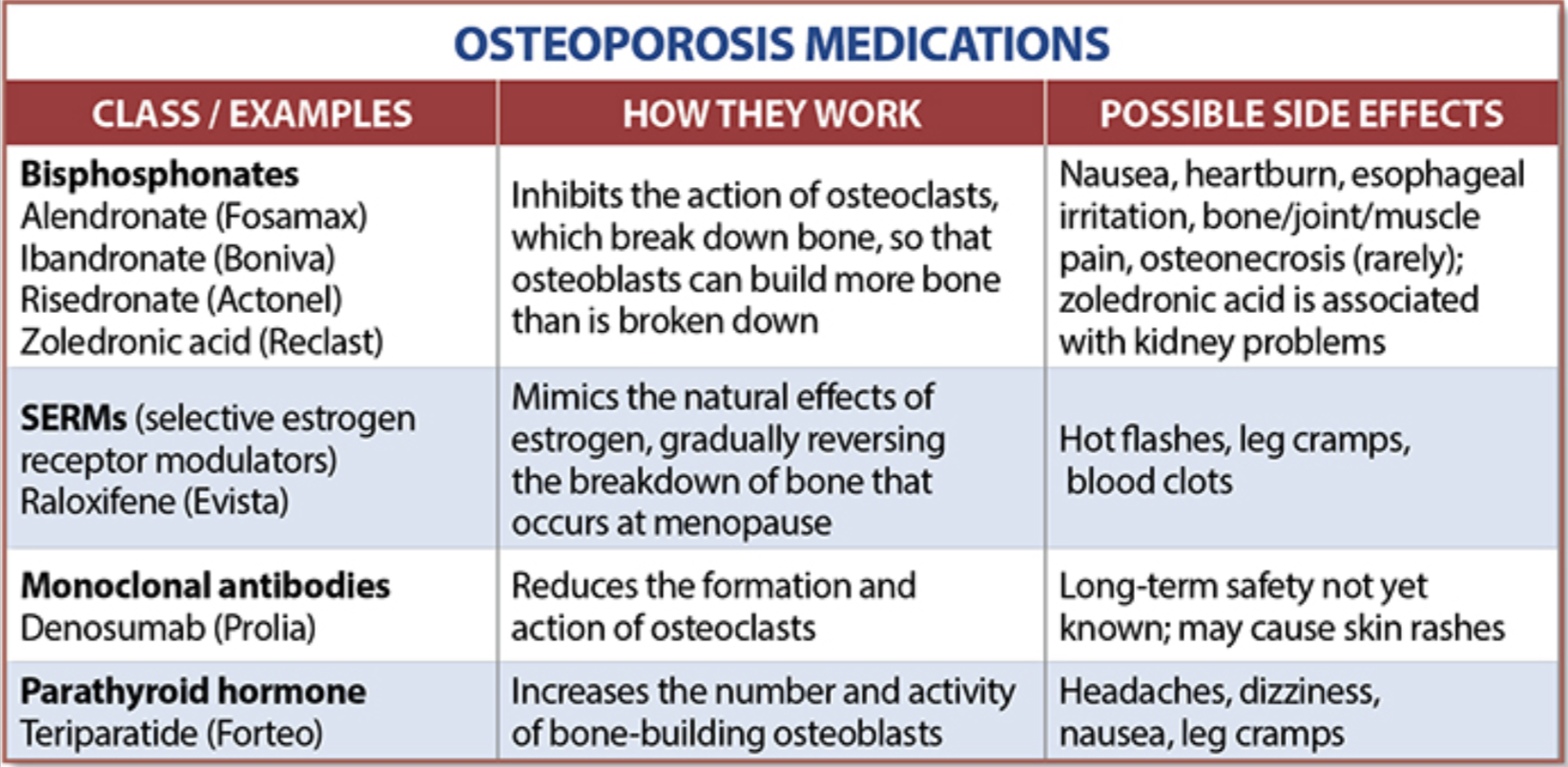
The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
GI Bleed following Weight Loss Surgery
September 17, 2018 10:28 am
Gastrointestinal (GI) Bleed following weight loss surgery is rare but does require knowledge of the particular bariatric surgical procedure the patients has and how to proceed with diagnostics to fully evaluate the situation. Acute or chronic gastrointestinal bleeding can cause anemia in patients. However, Anemia may also be caused by nutritional deficiencies (iron, vitamin , minerals), Kidney disease, bone marrow disease and others. The work-up for anemia following weight loss surgery follows a routine protocol. If there is an evidence of bleeding from intestine (bloody emesis, bloody bowel movement, “tar” like black bowel movements) then the diagnostic work up would include an upper and lower endoscopy.
Endoscopic Procedures:
Upper endoscopy Esophagogastroduodenoscopy (EGD): evaluates the esophagus, stomach and a limited area of the duodenum past pyloric valve.

Lower endoscopy Colonoscopy or coloscopy: evaluates the rectus and the entire colon.
Between these two tests, there is still a considerable amount of the small bowel that is not accessible or visualized with endoscopic procedures. For the small bowel, examination Capsule endoscopy is an option in an intact GI tract. Patients who have had Gastric bypass RNY or the Duodenal Switch, the large segments of the small bowel can not be visualized or examined with capsule endoscopy.



Patients who have had Duodenal Switch, Gastric Bypass and SADI – S would need a tagged red cell scan or CT angiography if GI bleed is suspected in areas of the small intestine that are inaccessible by endoscopic procedures.
PolyCystic Ovarian Syndrome PCOS
September 04, 2018 9:58 am
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.

Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
Bariatric Surgery can improve PCOS in those individuals with Type 2 Diabetes Mellitus. Further information on weight loss surgery and its effect on PCOS here.
Standard Common Channel In Duodenal Switch Will Result In Weight Regain.
December 16, 2016 1:57 pm
Stéfane Lebel, M.D.*, Geneviève Dion, M.D., Simon Marceau, M.D., Simon Biron, M.D., M.Sc., Maud Robert, M.D., Laurent Biertho, M.D. earlier this year released a research article comparing patients undergoing standard common channel of 100cm and standard common channel 200cm. The conclusion of this article was: “In this population, BPD-DS with a 200-cm common channel offered similar remission rate of co-morbidities compared with standard BPD-DS. It was associated with similar weight loss at nadir, followed by a more significant weight regain. It might yield a lower rate of nutritional complications. Long-term randomized data are needed to detect other potential advantages.”
Our Experience:
One of the most dreaded outcomes of any weight loss surgical procedure is weight regain. This is assuming that initial adequate weight was lost to result in resolution of the co-morbidities in the first place. As the weight loss surgical field has changed over the years so has been the cases of regain that we have seen.
There was a time when Lap bands were being revised for inadequate weight loss and weight regain. Not to mention the complications of reflux, difficulty swallowing and persistent Nausea and vomiting. Then as more Gastric bypass procedures “aged” the number of patients that started looking for revision for weight regain increased. The latest fad is the Vertical Sleeve Gastrectomy that are done with false sense of expectation and results. The long term outcome of Vertical Sleeve Gastrectomy is no where close to that of the Duodenal Switch, independent of the size of the sleeve. In fact, more surgeons are trying to get a little more weight loss by making the sleeve too tight. All they are doing is creating a significant and debilitating set of problems such as reflux, nausea, and solid intolerance.
The ideal revisional procedure for these patients should be the Duodenal Switch. Some surgeons, however, have started advocating “single anastomosis” knock off the duodenal switch. Others do “standard length common channel” rather than a Hess method Duodenal Switch. I have always performed a traditional Hess method Duodenal Switch. The Hess method Duodenal Switch has held the largest and longest excess weight loss maintenance for 28 years, going into 29 years. Here is a past blog regarding small bowel length.
The predetermined standard common channel results in weight regain. Study
Minimally Invasive Weight Loss Surgery
May 17, 2016 9:02 am
Minimally Invasive does not mean better, easier, proven outcomes or good excess weight loss. Weight loss surgical patients should be careful of catch phrases such as “less invasive”, “simpler”, “shorter recovery”, “outpatient” and many others that had been used to described procedures with less than optimal outcome. We should not forget the lessons learned from adjustable gastric banding which was also promoted as ” less invasive, simpler to perform, and be done as an outpatient with a short recovery “. We all know how that story has panned out. The overwhelming majority of patients who had an adjustable gastric banding have undergone revision, had it removed or had additional surgeries following the complications which were associated with this simple procedure.
When evaluating outcome data for weight loss surgical procedures, it is important to bear in mind that the long-term success of these procedures will take years to document. More often than not the early weight loss is significantly better than the long-term stable weight loss. This has been clearly documented in the case of the adjustable gastric banding and the gastric bypass and laparoscopic sleeve gastrectomy operation. Duodenal switch , as described by Dr. Hess using the percentage based technique, has the best long-term documented success of all of the weight loss surgical procedures. The scientific data reports 20+ years of successful excess weight loss with a Hess Duodenal Switch procedure. There has been an alternative proposed to Duodenal Switch recently, the SIPS and SADI procedures. As I have already stated in the past, these are not the same as the duodenal switch operation. Any suggestion or innuendos that SIPS/SADI is the same as the Duodenal Switch is deceptive and misleading. We have also seen attempts to use the same catch phrases as described above to promote these unproven procedures. The published data that’s been reported with SIPS/SADI is mostly short-term in small population studies. There are no long-term studies that have documented the efficacy of the SIPS/SADI procedure and “simpler” or minimally invasive does not mean better.
Billroth I or II and Diabetes
March 01, 2016 8:37 am
I have previously discussed the two variations of anastomosis that can be created between the stomach and the first segment of the small bowel. Historically, Billroth I and II procedures were named after Dr. Theodor Billroth who did the first of this type of operation in the 1881 (BI) and then in 1885 (BII).
The following article published in Bariatric Times 2016;13(2);8-10. discusses the resolution of diabetes and its outcomes based on these two types of the anastomosis between the stomach and the small bowel.


Billroth I VS Billroth II
This study concludes that “In summary, we concluded that based on our analysis of the literature, BII reconstruction is more effective than BI reconstruction for achieving postoperative diabetes control.”
Lets remind ourselves that Duodenal switch is a BII reconstruction where as the SIPS, SADI and other lookalikes are BI.
This study only reiterates that these unproven operations need to be studies further and that the patients need to be aware of the consequences of their decisions when choosing a particular operation. Be aware and informed to know the differences between Duodenal Switch and the procedures that are promoted as similar one – which they are not.
Visual comparison of Duodenal Switch and SADI/SIPS/Loop here.
Further description of Duodenal Switch here.
2015 ASMBS Summary
November 11, 2015 7:31 am
The 2015 ASMBS meeting was held November 2-6, 2015. It was combined with TOS (The Obesity Society) and had more than 5,600 attendees from all over the world in every aspect of obesity treatment. There were some interesting additions and deletions from this meeting compared to the past.
The one sentence that comes to my mind is “I told you so”.
One important addition was a DS course for Surgeons and Allied Health. This was very exciting, except the content and questions seemed to gravitate to SADI/SIPS/Loop rather than DS. Dr. Cottam was one of the moderators of the course. It seems that they have found the value in preserving the pyloric valve. It was clear that the discussion was driven by the need to come legitimize the single anastomosis procedures at this early stage with almost no data to prove long term outcome. With many of the Vertical Sleeve Gastrectomies having re-gain and the they are looking for a surgery that the “masses” can perform. This was actually the term used by one of the presenters, implying that the duodenal switch needed to be simplified so that all surgeons, those who have pushed all other procedures can not offer Duodenal Switch to their patients with less than desirable outcome. Several surgeons also voiced their concern and dissatisfaction with the issues and complication of the RNY and want an alternative. There was much discussion regarding SADI/SIPS/Loop being investigational and that it shouldn’t be as it is a Sleeve Gastrectomy with a Billroth II. Dr. Roslin and Dr. Cottam discussed their SIPS nomenclature saying they wanted to stay away from something that had Ileostomy, suggesting bowel issues, or the word “SAD”i due to negative connotations. The point to be made is that the SADI and SIPS and the loop are all the same. I have also noticed other surgeons using SADS (Single Anastomosis Duodenal Switch). There is a great deal of industry behind these procedures and many surgeons being trained in courses funded by industry. One surgeon stood up and informed the entire course that they need to be clear with their patients about the surgery they are performing, as he had been in Bariatric chat rooms and there is upset within the community about SADI/SIPS/Loop being toted as “the same or similar to Duodenal Switch”.
There was also presenter who said “We are doing something new about every five years.” No, “we” are not. Some of us have stood by the surgery and techniques with the best long term outcomes and not gone with every “new” thing out there. The process of Duodenal Switch may have changes, open Vs. Lap, drains, location of incisions, post operative care and stay, but the tested procedure with the best outcome has been the duodenal switch operation and not the shortcut versions. Although, those of us that are standing by long term results seems to be in the minority. Why do I stand by Duodenal Switch? Because it works, when done correctly by making the length of the bowel proportional to the patient total bowel length, and height, and not just cookie cutter length for all patients, with the right follow-up, patient education, vitamin and mineral regime and eating habits.
A new addition was the Gastric Balloon, which in the research presented had a 60-70% re-gain rate and a no more than 10-15% weight loss one year only. This data represents more than 70% weight regain when the balloon is taken out. The Gastric Balloons can be left in between 4-6 months depending on the brand or type of balloon. The Gastric Balloon is not new to the Bariatrics and was first introduced in 1985. After 20 years and 3,608 patients the results were and average of 17.6% excess weight loss. It seems that we are re-gurgiating old procedures. There are many new medications that were front and center in this meeting.
The Adjustable Gastric Bands were missing from the exhibit hall this year. It is my hope and feeling from the other attendees that we may be seeing the era of the Adjustable Gastric Band being placed in patients come to an end. Although there are some still holding out that there are some patients that can do well with the Band.
Attending the 2015 ASMBS meeting this year, as it has every year, only reemphasized the importance of avoiding what has become the norm of chasing a simple solution that is fashionable and easy now. We stay convinced that the duodenal switch operation with the common channel and the alimentary length measured as a percentage of the total length is by far the best procedure with the proven track record. The patient should avoid the temptation of settling for an unproven procedure or device, because if history holds true, there will be a need for revision surgeries in the future.
Duodenal Switch Look Alikes- SADI/SIPS/Loop
October 23, 2015 4:06 pm
There is no substitute for the Duodenal Switch (DS) operation. The other easier procedures that are being presented as DS equivalent are untested, and unproven operations that in my opinion will fall short of the outcome patients expect. The coding definition of BPD/DS is as follows: A Gastric restrictive procedure with partial gastrectomy, pylorus-preserving duodenoileostomy and ileoileostomy (50 to 100cm common channel) to limit absorption (biliopancreatic diversion with duodenal switch) Please not that there are two anastomosis within the definition.
As a patient advocate and a surgeon who has seen a number of recent complications (significant bile reflux gastritis, inadequate weight loss, etc..) of these “Duodenal Switch” substitute procedures, (SADI/SIPS/Loop) I would recommend that any patient considering anything other than the anatomically accurate and proven standard DS procedure realize that they are being subjected to a procedure with an unknown long-term outcome other than what is published in a few studies with a very short-term follow-up. The weight loss of SADI/SIPS/Loop studies have only been measured in terms of months versus years. I would predict that for the majority of those patients, the long-term weight loss will be inadequate and further corrective surgery will be needed, either for inadequate weight loss or other complications such as bile reflux.
Single-Anastomosis DuodenoIleal Bypass (SADI), SIPS, Loop
June 23, 2014 1:45 pm
Single anastomosis duodenal switch, also known as Single Anastomosis DuodenoIleal Bypass (SADI) is a procedure that is being discussed more frequently in the literature. There have been a few series of case reports that have been published in the last few years. I would like to review the procedure and share my opinion.
The theory behind the SADI has been to simplify the duodenal switch procedure. In “classical” duodenal switch procedure, the small bowel is divided in two places, (duodenum, and distal ileum) and two anastomosis are created (duodeno-ileostomy, and ileo-lieostomy). This can theoretically provide two potential places for leak, bleeding, adhesions as complications. In SADI, there is a single bowel division of the duodenum and a single anastomosis of the duodenum and the ileum. The sleeve component of the procedure is the same for both procedures. This is where their similarities end.
In the duodenal switch operation, the bowel is partitioned in to two parallel limbs- one that carries the biliopancreatic juices and a parallel limb that bring the food down from the post pyloric duodenum. They then join and form the common channel. The length of the biliopancreatic limb is so long that it does not allow bile to reflux back into the duodenum or back to the stomach causing the complication of bile reflux gastritis. With the single anastomosis of the SADI, the length of the bowel where the bile meets the duodenum is shorter than it is in normal anatomy. This significantly increases the possibility of the bile reflux. The second difference is the selective nature of the reduced absorption of the fat in the duodenal switch, in comparison to that of the carbohydrates. Duodenal switch operation has two absorptive lengths- the Alimentary channel, which is involved with protein and carbohydrate absorption, and the common channel that absorbs, fat, protein and carbohydrates. One can make changes to the common channel and impact the fat absorption significantly more than that of the carbohydrate and the proteins. In SADI procedure, that common channel and the alimentary limb are both the same- there is no way to selectively adjust the fat absorption without making significant changes to that of the protein and carbohydrate absorption.
Other than the obvious anatomical variations described above, it is important to mention that the concerns outlined above are mostly theoretical.
There are a number of publications that have reported the short-term outcome of the SADI procedure. They appear promising, but they are short-term results. Long-term data is needed. If the outcome does not change significantly over time, then I could see a role for SADI in the treatment for obesity. In the mean time, patients need to be made aware that the suggestion that SADI is the same as the duodenal switch is probably not correct since we do not have the data to support this oversimplification.
The animation of the Duodenal switch is here.
For comparison of duodenal Switch and SADI please check our web site here.