Tag: revisional weight loss surgery
Dr. Facebook
March 22, 2019 8:24 am
We have become reliant on the information that we obtain from the internet, specifically platforms such as Facebook. In our practice we have to continuously correct information that patients have obtained from other patients, unmonitored sites, blogs, and postings. Most of this information is based on individual experiences that has become gospel. “Fat is good for you” is one of them. To clarify, some health fat (olive oil, avocado, Omega 3) is healthy and needed for all patients. We do not recommend “fat bombs” as a part of ones daily dietary intake.
The following article was written on the accuracy of nutritional posts in support groups on Facebook.
Koalall et. all in SAORD, December 2018 Volume 14, Issue 12, Pages 1897–1902 published
“Content and accuracy of nutrition-related posts in bariatric surgery Facebook support groups”
The conclusion, as suspected, that “Over half of the posts contained inaccurate content or information that was too ambiguous to determine accuracy..:”

It is our recommendation before any dietary recommendations are taken from facebook and the like, the source of the information should be verified. As I have stated in the past, a frequent flier passenger is probably not qualified to fly a
commercial airplane, any more than a previous weight loss surgical patient providing medical and nutritional advice. We realize that there is significant value to the forum for exchange of information and sharing of experiences with other weight loss surgical patients as long as the information is well sourced and verified.

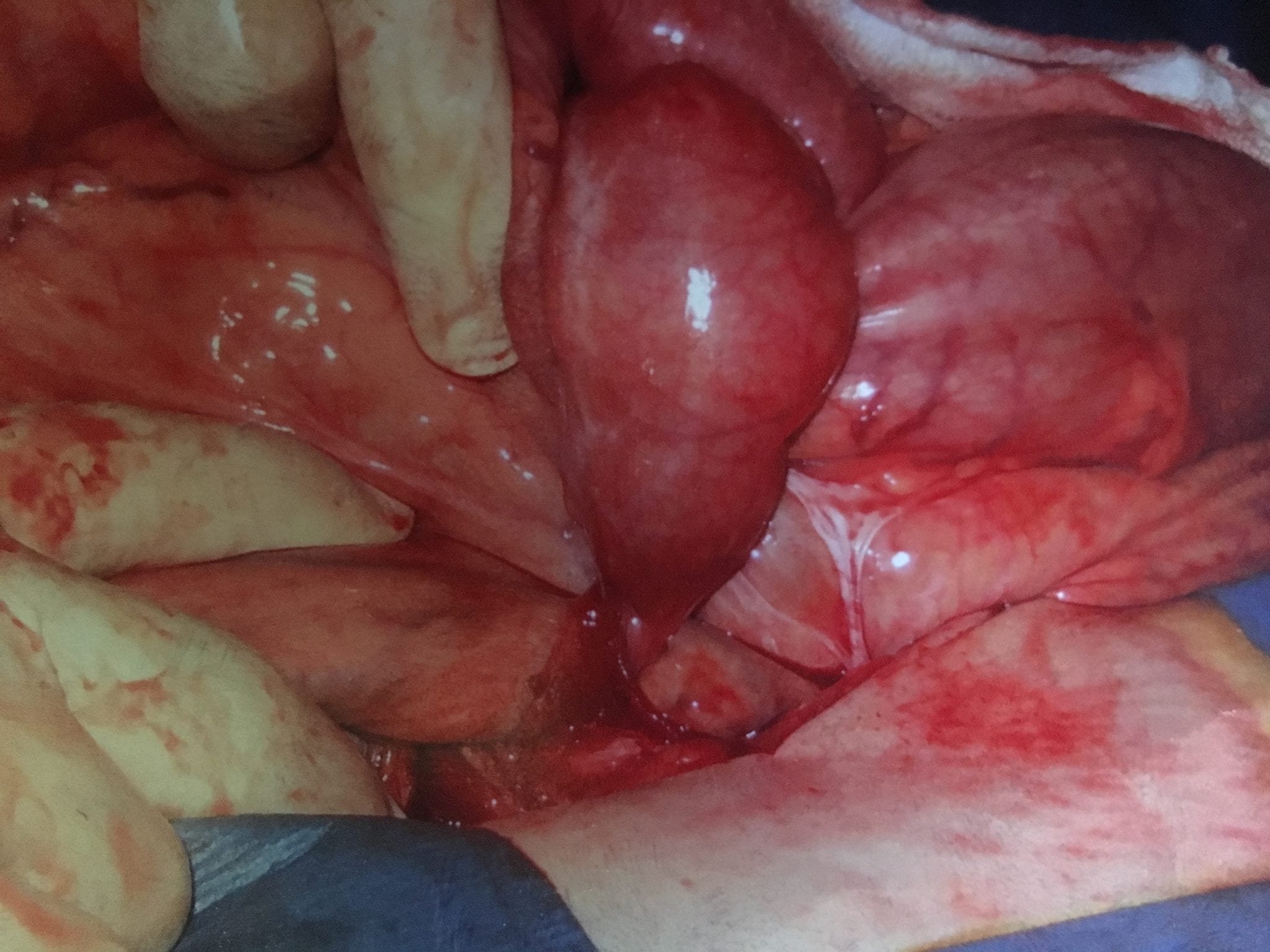
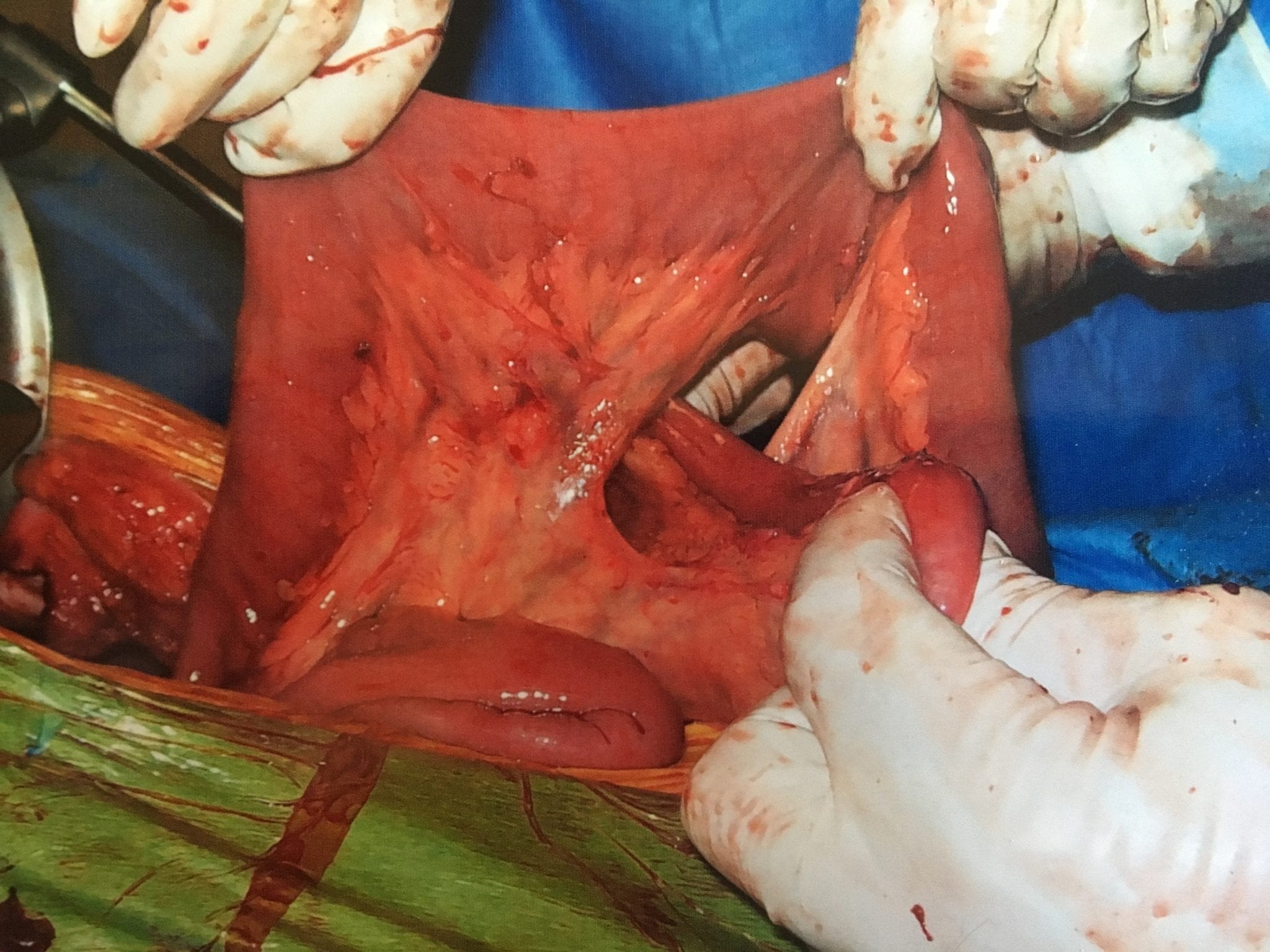
Adhesions, Internal Hernia And Bowel Obstruction
December 15, 2018 2:35 pm
Adhesions are fibrous bands of scar tissue that form during the healing process. Following surgery, many people live normally with this scar tissue. However, they are also the cause of bowel obstruction when the adhesions form in such a way that causes a segment of the bowel to either get trapped, or form a “knot”. In both of those cases, the end result is a partial narrowing or a complete blockage of the intestines. This is called bowel obstruction.
Without treatment, the blocked parts of the intestine can die, leading to serious issues. However, with prompt medical care, intestinal obstruction often can be successfully treated.
Other causes of bowel obstruction:
- In children, the most common cause of intestinal obstruction is telescoping of the intestine (intussusception).
- Intussusception telescoping of the interstine
- Hernias — portions of intestine that protrude into another part of your body
- Inflammatory bowel diseases, such as Crohn’s disease
- Diverticulitis — a condition in which small, bulging pouches (diverticula) in the digestive tract become inflamed or infected
- Twisting of the colon (volvulus)
- Impacted feces
- Colon Cancer
In patients who haven’t Bariatric / weight loss surgery or an untouched GI track, bowel obstruction may manifest itself by symptoms of loss of appetite, constipation, nausea, vomiting, enlarged abdomen, abdominal pain, cramping, with no passage of gas or bowel movements.
However, patients who have had a weight loss surgery (Duodenal Switch, or the Gastric Bypass) because of the parallel limbs of the small bowel, the symptoms outlined above may not present. The diagnosis of a bowel obstruction, when suspected, should be identified with CT scan of the abdomen and pelvis with Oral and IV contrast. A CT scan with no oral contrast or water instead of oral contrast is inadequate and may lead to a delay in diagnosis and surgical intervention. Examples of Bowel Obstruction CT findings were discussed previously.
The treatment for an internal hernia and adhesions causing a bowel obstruction depending on the severity may range from observation to surgical intervention in order to release the small bowel from the constraints of the adhesions.
Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP
Health Insurances Working Against You
July 09, 2018 12:01 pm
Are Health Insurances working against you? Especially in people who have the disease of obesity? Insurance companies continue to lengthen the pre-operative period. The time that is required to lapse has now in some cases been extended between 6-12 months for some commercial health plans. There are yet again studies that have shown no benefit to the patient with this mandated waiting periods imposed on the patients. Unfortunately, the patients need to challenge the health care insurance companies by the means of all options that may be available to them. This may include internal appeal to external evaluation by some state agency. There are numerous studies that show pre-operative dieting does not equal better weight loss or compliance.


Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

Candy Cane Gastric Bypass – RNY
June 21, 2018 1:05 pm
One of the findings following Gastric Bypass is a Candy Cane Gastric Bypass. Nausea and vomiting , upper abdominal pain is a common complaint of patient who have had the Gastric Bypass RNY operation. This is in addition to the high incidence of patients who experience the complications of weight regain and or dumping syndrome.
Quite frequently the symptoms of nausea, vomiting and upper abdominal pain of a patient with history of gastric bypass is evaluated by a primary care, referred to a gastroenterologist. The “routine” work up recommended is X-ray of the abdomen, maybe contrast study (Ct scan or upper GI) and for sure and upper endoscopy. The result quite frequently reported as “…nothing wrong”.
A typical upper GI in a Candy Cane Gastric Bypass situation may look like this:

A common and underreported problem may be a Candy Cane finding. The “blind” end of the small bowel anastomosis is too long and this results in food settling in the hook of the candy cane. The symptoms of the nausea, vomiting and upper abdominal pain may be from the residual food and liquids that do not drain from this area.

Candy Cane Gastric Bypass finding

Candy Cane Gastric Bypass cases will require surgical intervention to shorten the length of the blind segment of the small bowel to improve symptoms.
It is my recommendations that any patient with history of weight loss surgery who is having any persistent gastrointestinal symptoms be evaluated by weight loss surgeon.
Revision from failed AGB to Duodenal Switch
January 10, 2018 2:10 pm
A few times a month during consultation for weight loss surgery , I’m ask as to why I do not offer the adjustable gastric banding as an alternative to the patients. As I have said over the years when a patient considers an weight loss surgery the totality of the risk should be considered. This includes the operative, immediate postoperative course, the maintenance and the follow-ups needed. The potential complications of the procedure in addition to the long-term success off each operation should also be taken into account.
Unfortunately, some patients are led to believe that any perceived benefit in the short operative time and the ease of the adjustable gastric banding also translates to a better outcome. This is in fact the opposite of what the published data have shown, a recent study published in April 2017 by Vinzes et.al, shows that 71% of patient lost their band by 10 years out.




What is also interesting that more patients underwent revision from failed AGB to the duodenal switch than the sleeve gastrectomy (Fig 1.). This is what I also recommend.
More importantly, The patients who underwent a revision from failed AGB to the duodenal switch operation had the best long term results of all patients (Fig 2.) note the “rBPD” line that is the highest of %EBMIL.
Complication’s were broad and frequent (Table 3.)
Further information on revision from failed AGB to Duodenal Switch or other failed weight loss surgeries can be found here.
New Pasadena Office Map and Parking
August 12, 2017 8:35 am
We’ve created a helpful map and parking diagram for our new Pasadena, CA office location. It also has a general layout of the Huntington Memorial Hospital Campus and Pre-operative intake and testing area. We hope that you find it helpful on your next visit to see Dr. Ara Keshishian, General and Bariatric Surgeon.

Dr. Ara Keshishian has performed more than 2,000 Duodenal Switch procedures, thousands of Sleeve Gastrectomies and more than 500 revisions from other Weight Loss Surgeries such as RNY Gastric Bypass, Adjustable Gastric Band, and Sleeve Gastrectomy to Duodenal Switch as well as General Surgical cases over the last 18 years of private practice.
Insurance Appeals And Denials
August 07, 2017 7:08 am
Whenever you are dealing with insurance issues it is important to have a general understanding of insurance ins and outs. The Obesity Action Coalition has a good general guide to the insurance process here. If you are having issues with out of network, out of area, or insurance appeals and denials for Duodenal Switch, there may be some additional assistance from two individuals who have had the Duodenal Switch procedure themselves. We are grateful that they have provided assistance throughout the years to the Duodenal Switch community. The following is their statement on insurance.
The majority of insurance companies are in the business of making money (for profit). They can deny requests for preauthorization with impunity. These denials are often complexly worded and difficult to comply with and overcome, and are definitely overwhelming to the patient, and the busy surgeon’s office. The vast majority of patients faced with demanding if not impossible to achieve prerequisites, or denial of the request for preauthorization simply give up, and the insurance companies pocket the savings.
If you find yourself facing impossible pre-op hurdles, or a denial, we urge you to appeal, and to seek assistance in preparing the appeal. You can hire an attorney, of course, but there is an informal and free resource we suggest that you investigate as well.
If you go to BariatricFacts.org (a non-profit, patient-run site), you will find individuals who are long-term DS postops, and patient advocates. They have been helping patients, pro bono (for free), for over 10 years. They will help you draft your appeal letters, provide supporting medical and legal documentation, and prepare draft letters of medical necessity to be reviewed and signed by your surgeon supporting your appeal. They will not represent you directly, but they will help you best represent yourself. in many cases it is necessary to exhaust all internal appeals (because the insurance companies are unlikely to overrule themselves), and then file for external review, where independent reviewers often overrule improper denials. If you join and then post on BariatricFacts.org asking for help, you will be connected with them and you can decide if you want their help.
Please note that this is just a suggestion. It is neither legal nor medical advice, nor a guaranty regarding their services, and you should always consider getting legal advice and assistance from an attorney who will represent you directly. The members at BariatricsFacts.org will help you draft your own letters, but will not be your legal or medical representatives; you will be required to do a fair amount of your own work on your appeals, and to sign them yourself.
It is suggested that before or at the same time as you contact the resources suggested at the site, you gather as much of the following information as you can:
- A copy of your Evidence of Coverage, which is the usually 100+ page insurance contract between your employer and the insurance company, which you can obtain it from your HR department. If you are self-insured, it will be available directly from your insurance company. Note: it is NOT the Summary of Benefits – it needs to be the contract itself.
- If your insurance is through an employer, you need to determine whether your plan is self-funded or fully-funded. Your rights are significantly different under the two types of plans.
- If your insurance company has a separate bariatric surgery policy, provide a copy of that, too.
- A copy of your surgeon’s request for preauthorization, which provides the ICD-10 and CPT codes submitted.
- A copy of your denial letter, including the section regarding your appeal rights.
* It is strongly recommended that you obtain a copy of your surgeon’s LOMN (letter of medical necessity) before it is submitted to your insurer or for external review, so we can assist your busy surgeon in making the strongest possible case for you.
Don’t be deterred by a denial. It is unfortunately more common than it should be, but it can often be overcome if you meet the requirements for bariatric surgery, if you get help navigating the process.
Shared Success- Samantha had a Sleeve to Duodenal Switch Revision
July 14, 2017 9:30 am
After struggling with obesity for most of my life I was finally fed up. I had heard about weight loss surgeries before but was always under the common misconception that it was for people who wanted the “easy” way out of a hard situation. I had been working out and reducing calories and tried every popular diet and trainer you could think of. I was still huge and each time I would stop one of these extreme programs I would only end up larger than I was before.
My husband’s cousin had the sleeve surgery and she raved about it. Watching her success is what started to open my mind to surgery, but I was only considering the sleeve gastrectomy. I went to a center in another state that offers Duodenal switch, lapband, RNY and the sleeve. The surgeon I met with strongly suggested RNY to me, but I was stuck on the sleeve. I didn’t want my intestines touched period. I had the sleeve surgery on October 9, 2013.
My high weight was 402 lbs and I weighed 343 on the day of my sleeve surgery. I actually did well with the sleeve and was able to get down to 218 as my lowest. However it was still much like dieting. It was so stressful. After a while my body wouldn’t drop the weight regardless of how little I ate and exercised. I was eating 800-1200 calories a day and low fat meals and working out and kept slowly gaining weight. I was frustrated and honestly I gave up. My reflux wouldn’t go away so I visited a bariatric surgeon in my area who suggested that we essentially re-do the sleeve surgery to make my sleeve small again so that I would eat less and lose weight again. I got a second opinion and that surgeon suggested I revise to RNY. I went to obesity help’s website to explain my situation and a lot of people with much more experience than me HIGHLY urged me to see Dr Keshishian before making a decision. He was said to be an expert in revision weight loss surgery. I almost cancelled my appointment and didn’t have hope with this doctor either, but since I was in a dead end I went anyway. Dr Keshishian told me it wasn’t my fault. WHAT!? I had never heard that before. I usually get the shame from doctors who assume I must not be trying or that I am secretly eating something wrong. He ordered tests and told me it was “simply science” and I just LOVED him! I had a stricture in my Sleeve that needed to be repaired so since I needed surgery anyway I decided to go ahead and revise to a surgery that has the highest success rate, Duodenal Switch.


I was so scared of my intestines being cut and Dr. Keshishian eased my fears. I wish I had went that route the first time but then I might not appreciate it like I do now. Duodenal switch is the ONLY surgery I would recommend to anyone. As Dr K says it’s simple numbers. It’s the surgery with the highest percent of excess weight lost and kept off. I was 252 before my revision from Sleeve to Duodenal Switch and I am just at a year out and today I weigh in the low 190’s and I am still losing. Dr K’s goal for me was about 180. My goal is about 175. I eat more fat now than I ever did even when I was 400 lbs. I enjoy what I eat and I enjoy exercising and most of all I get to enjoy seeing results from my hard work. Food no longer causes me stress and anxiety. I know with 100% certainty that I made the right decision. Thank you Dr. K for your great skill and I don’t mean just with the knife but with the way you are able to make a high anxiety situation seem like no big deal.

