Category: Adhesions
Cholangitis
May 24, 2026 11:33 am
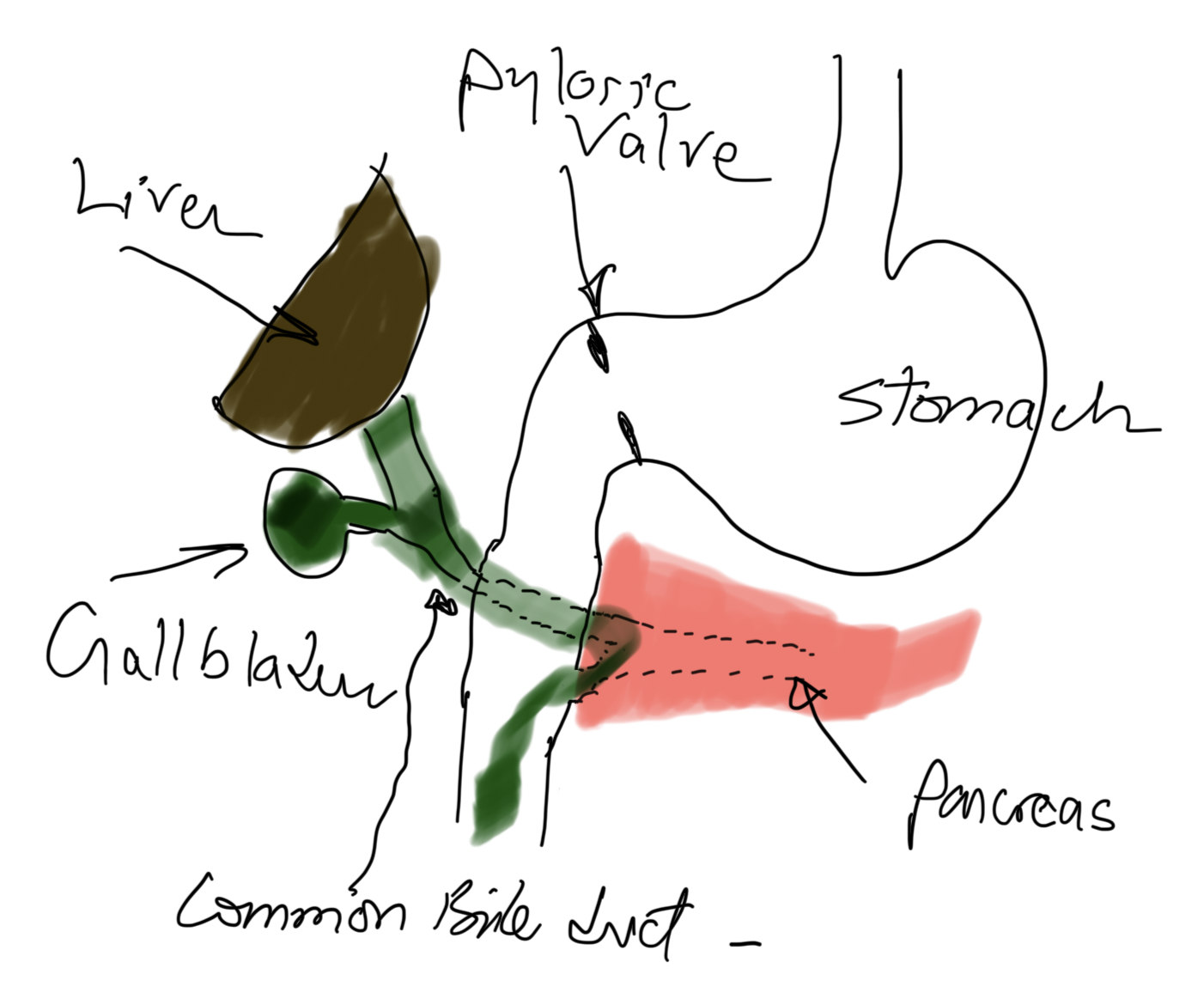
Cholangitis refers to infection and inflammation of the bile ducts because of obstruction and introduction of bacteria or other pathogens from the GI tract.
- Hydration with IV fluids,
- Broad coverage with IV antibiotics administration and
- Drainage procedure (ERCP, papillotomy, Stent placement, Cholecystectomy with common duct exploration, and T-tube placement)
These steps are almost all taking place concurrently and urgently. This is not something a patient waits and sees how it goes- it only goes one direction, from bad to worse. This is not to sound alarmist; a correct diagnosis is critical.
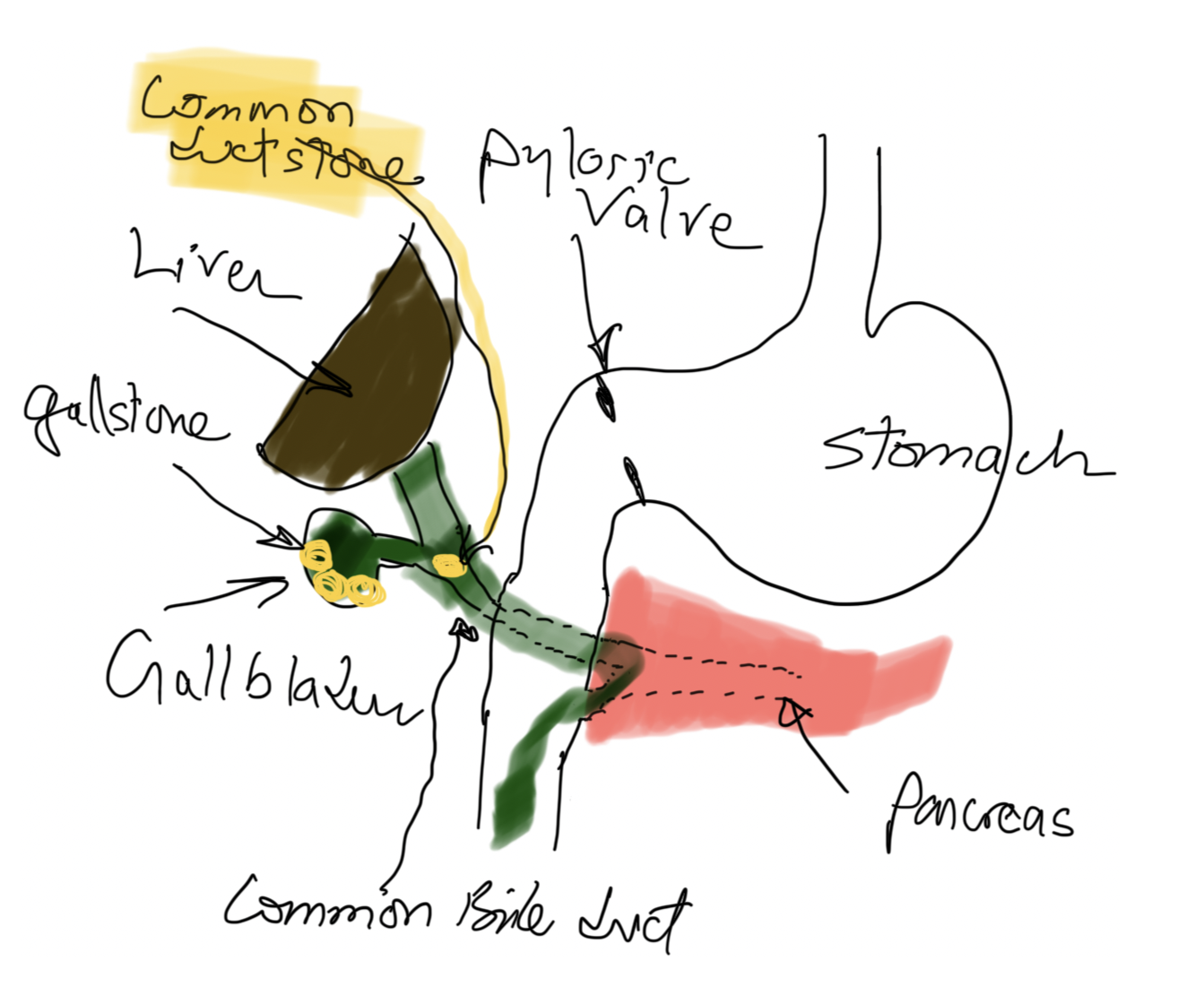
Risk factors for cholangitis may include gallstones that travel down the bile duct and cause jaundice, pancreatitis if passed, immunosuppression, malnutrition, and diabetes, to name a few.
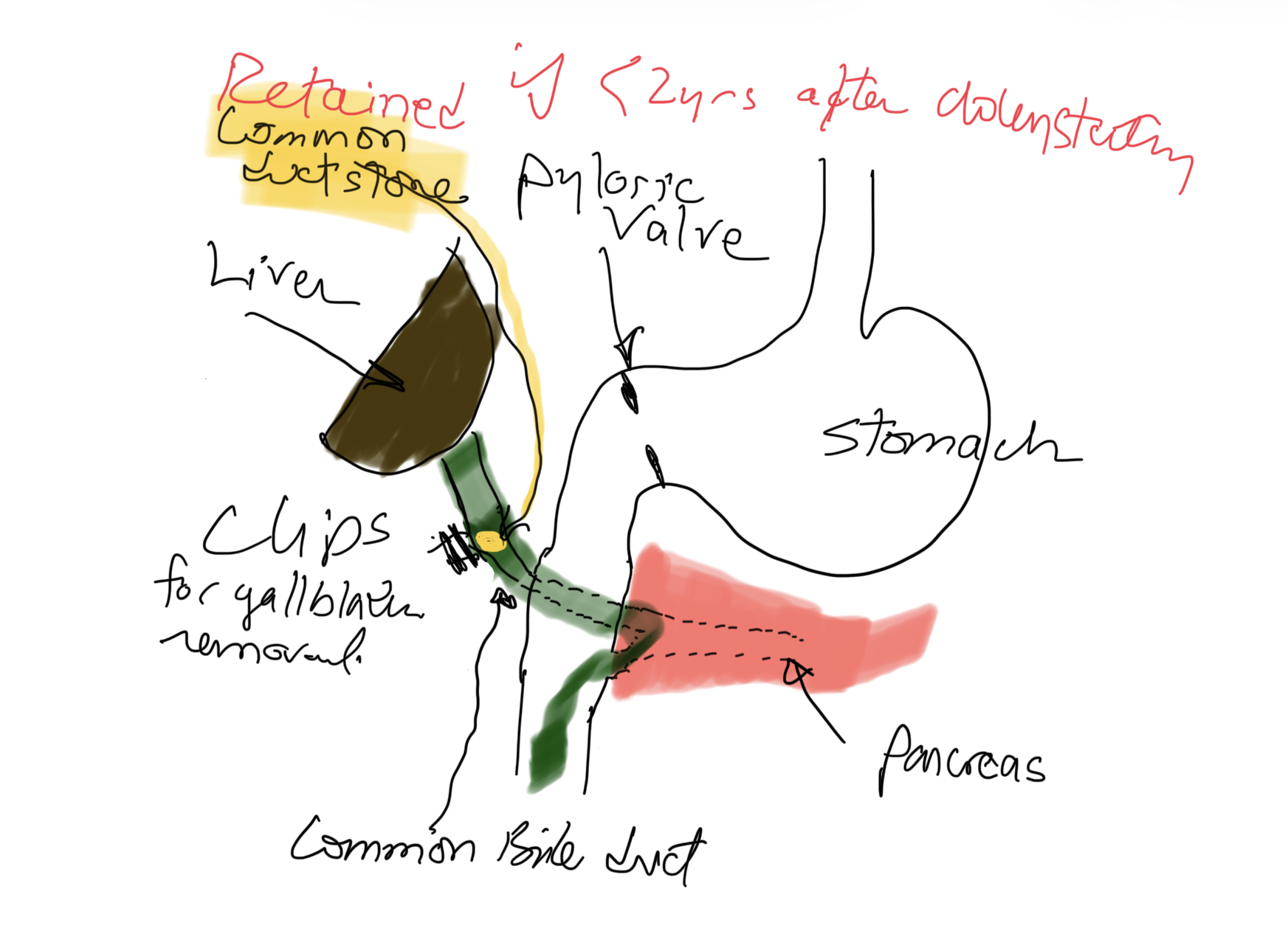
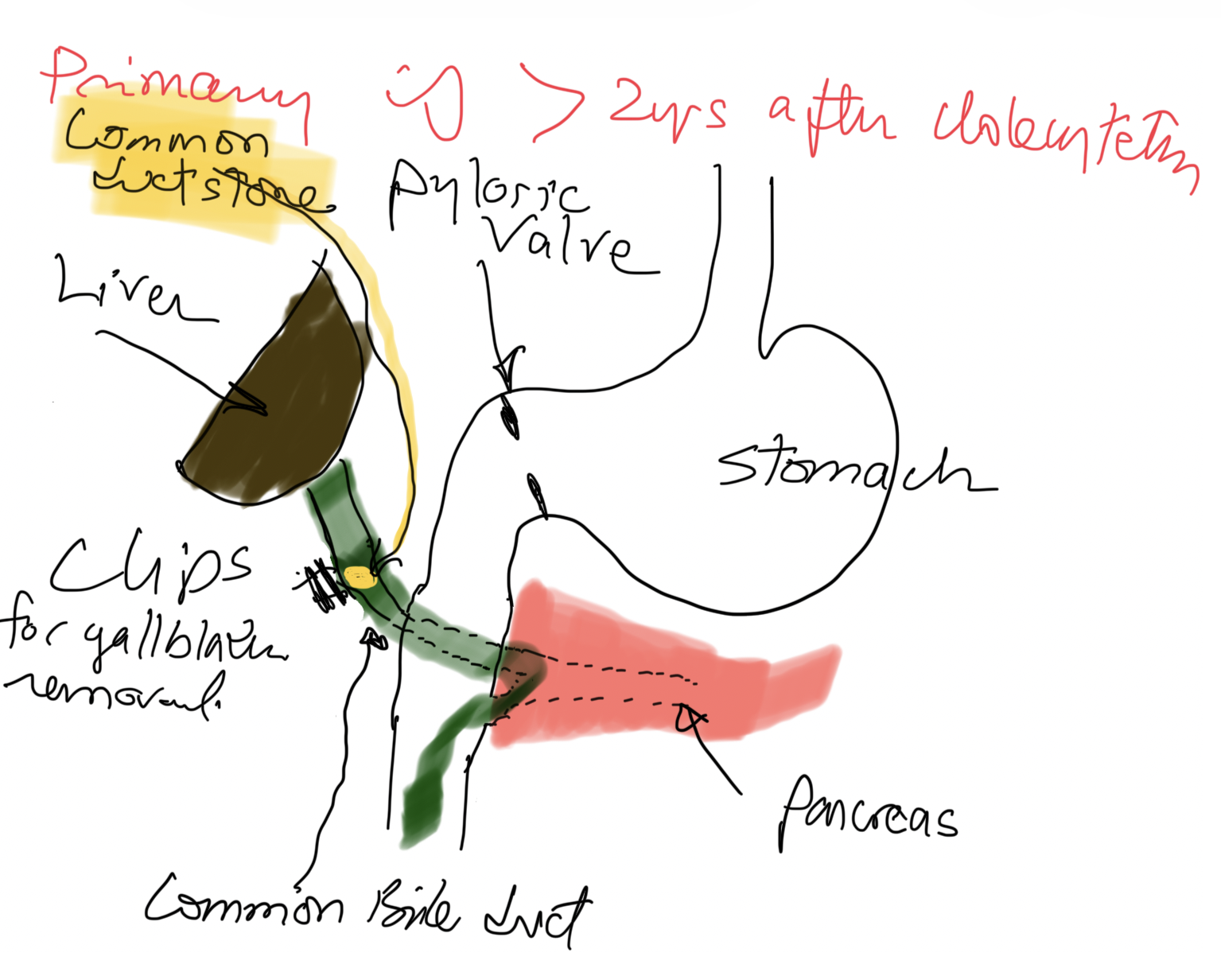
If a patient has gallstones in the bile duct less than 2 years after cholecystectomy, it is a Retained Stone(s), meaning there was a small stone that was not in the gallbladder and was not seen on US, intraoperative cholangiogram, or ERCP (if performed before surgery).
Colonic Volvulus
March 15, 2025 11:23 am
A volvulus is when a loop of intestine twists around itself and the mesentery that supports it, resulting in a bowel obstruction that can compromise intestinal blood flow. For this reason, it tends to be a surgical emergency which requires prompt attention; failure to recognize the signs and symptoms of intestinal volvulus may lead to bowel ischemia and perforation. A volvulus can develop anywhere along the intestine, however for this blog we will discuss types of Colonic Volvulus.

The most common forms of volvulus in the gastrointestinal tract are sigmoid and cecal volvulus, both colonic volvulus. Sigmoid volvulus is responsible for 80% of intestinal obstructions.
Volvulus can occur anywhere in the large and small GI tract. This is caused by a bowel twist around an anchor position, which may be the mesentery. Think about how the loose skin hangs lower with weight loss. We see the mesentery fat thinning, which causes the bowel to twist around it. A very high degree of suspicion is needed to make the diagnosis.

High-fiber diets and chronic constipation are common risk factors because they cause increased gas and sigmoid colon elongation. Worldwide, the incidence of men is much higher than in women, which may be explained by the mesenteric shape, which tends to be longer and has a narrower base. In weight loss surgical patients specifically, such as Duodenal Switch, increased gas and diarrhea are shared in patients with carbohydrate and fiber-rich diets. In some cases, they are recommended to have a high fiber diet by other providers who may not be aware that this may only complicate the problem and exacerbate the symptoms. The solution would not include adding fiber but eliminating the underlying food items causing the increased gas and diarrhea.

A definitive diagnosis is made with a CT scan, and the treatment is generally a bowel resection. However, in the case of a sigmoid volvulus, an urgent endoscopic detorsion may be attempted first, only if there are no signs of ischemia. The risk of recurrence following endoscopic detorsion alone is as high as 90% and carries a high risk of mortality up to 35%, therefore definitive elective sigmoid resection is recommended.
Here is a short video of an operation.
We want to thank Miguel Rosado, MD, for his significant contributions provided in this Blog.
Adhesions, Internal Hernia And Bowel Obstruction
December 15, 2018 2:35 pm
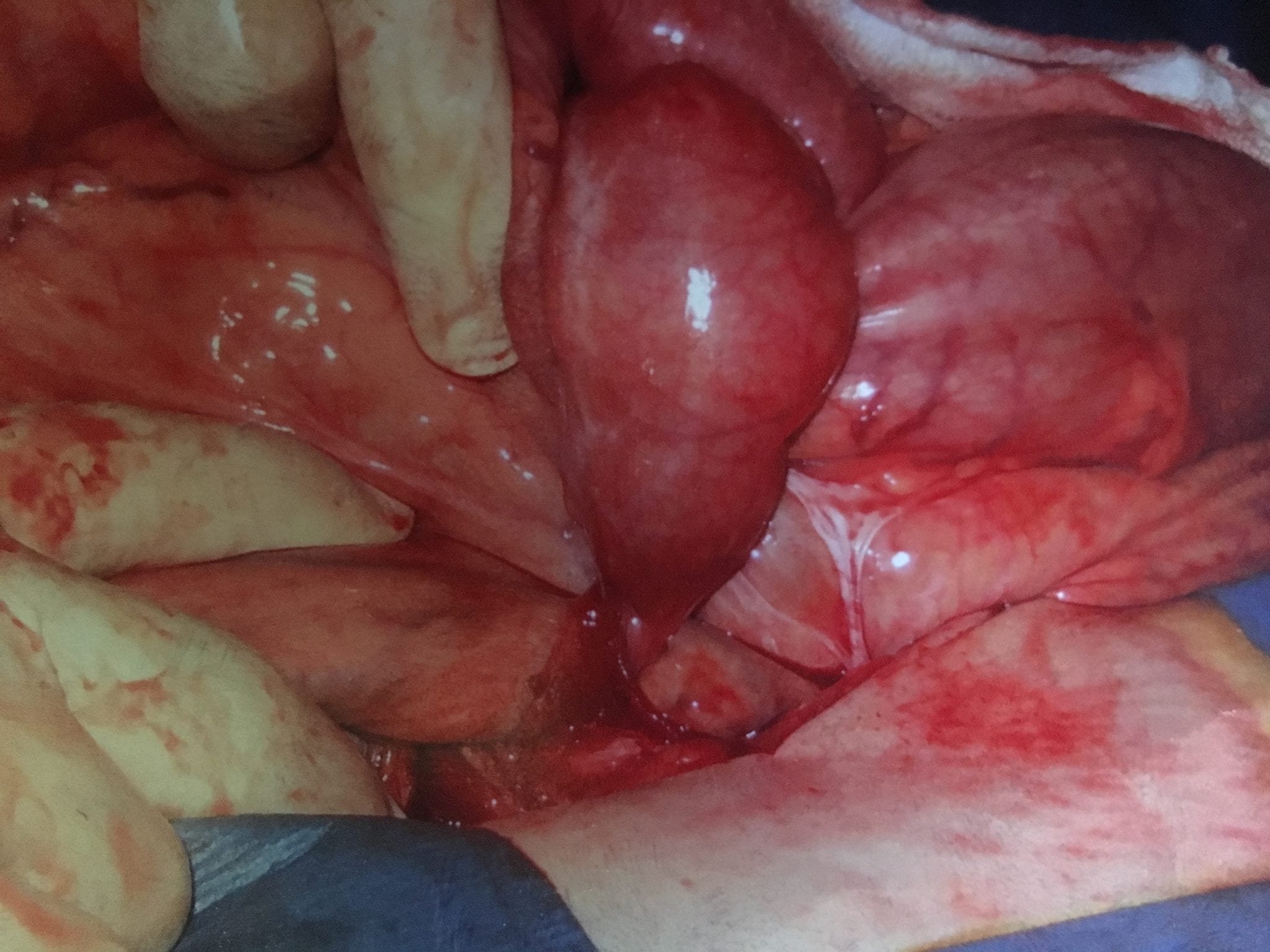
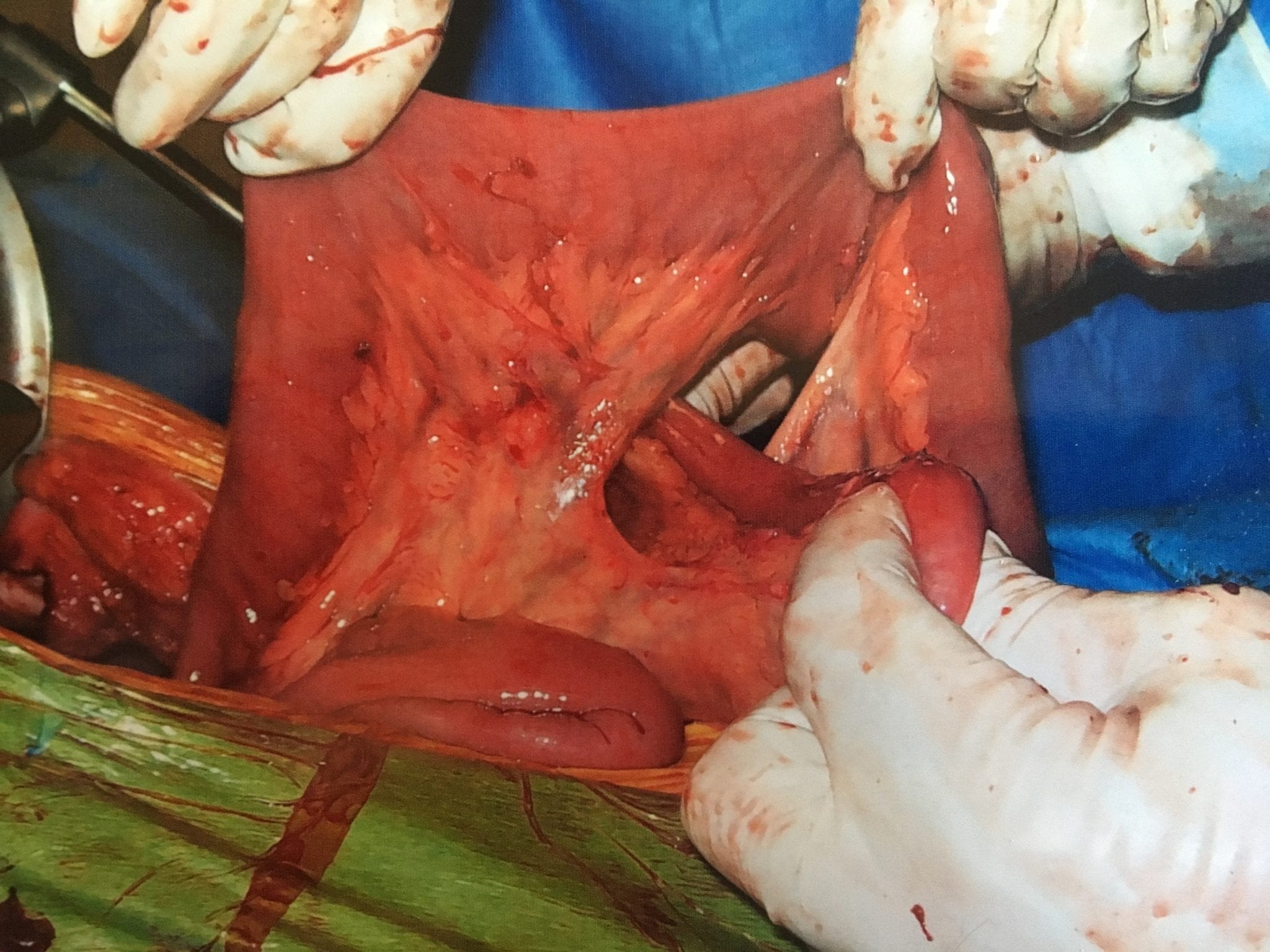
Adhesions are fibrous bands of scar tissue that form during the healing process. Following surgery, many people live normally with this scar tissue. However, they are also the cause of bowel obstruction when the adhesions form in such a way that causes a segment of the bowel to either get trapped, or form a “knot”. In both of those cases, the end result is a partial narrowing or a complete blockage of the intestines. This is called bowel obstruction.
Without treatment, the blocked parts of the intestine can die, leading to serious issues. However, with prompt medical care, intestinal obstruction often can be successfully treated.
Other causes of bowel obstruction:
- In children, the most common cause of intestinal obstruction is telescoping of the intestine (intussusception).
- Intussusception telescoping of the interstine
- Hernias — portions of intestine that protrude into another part of your body
- Inflammatory bowel diseases, such as Crohn’s disease
- Diverticulitis — a condition in which small, bulging pouches (diverticula) in the digestive tract become inflamed or infected
- Twisting of the colon (volvulus)
- Impacted feces
- Colon Cancer
In patients who haven’t Bariatric / weight loss surgery or an untouched GI track, bowel obstruction may manifest itself by symptoms of loss of appetite, constipation, nausea, vomiting, enlarged abdomen, abdominal pain, cramping, with no passage of gas or bowel movements.
However, patients who have had a weight loss surgery (Duodenal Switch, or the Gastric Bypass) because of the parallel limbs of the small bowel, the symptoms outlined above may not present. The diagnosis of a bowel obstruction, when suspected, should be identified with CT scan of the abdomen and pelvis with Oral and IV contrast. A CT scan with no oral contrast or water instead of oral contrast is inadequate and may lead to a delay in diagnosis and surgical intervention. Examples of Bowel Obstruction CT findings were discussed previously.
The treatment for an internal hernia and adhesions causing a bowel obstruction depending on the severity may range from observation to surgical intervention in order to release the small bowel from the constraints of the adhesions.