Category: common channel
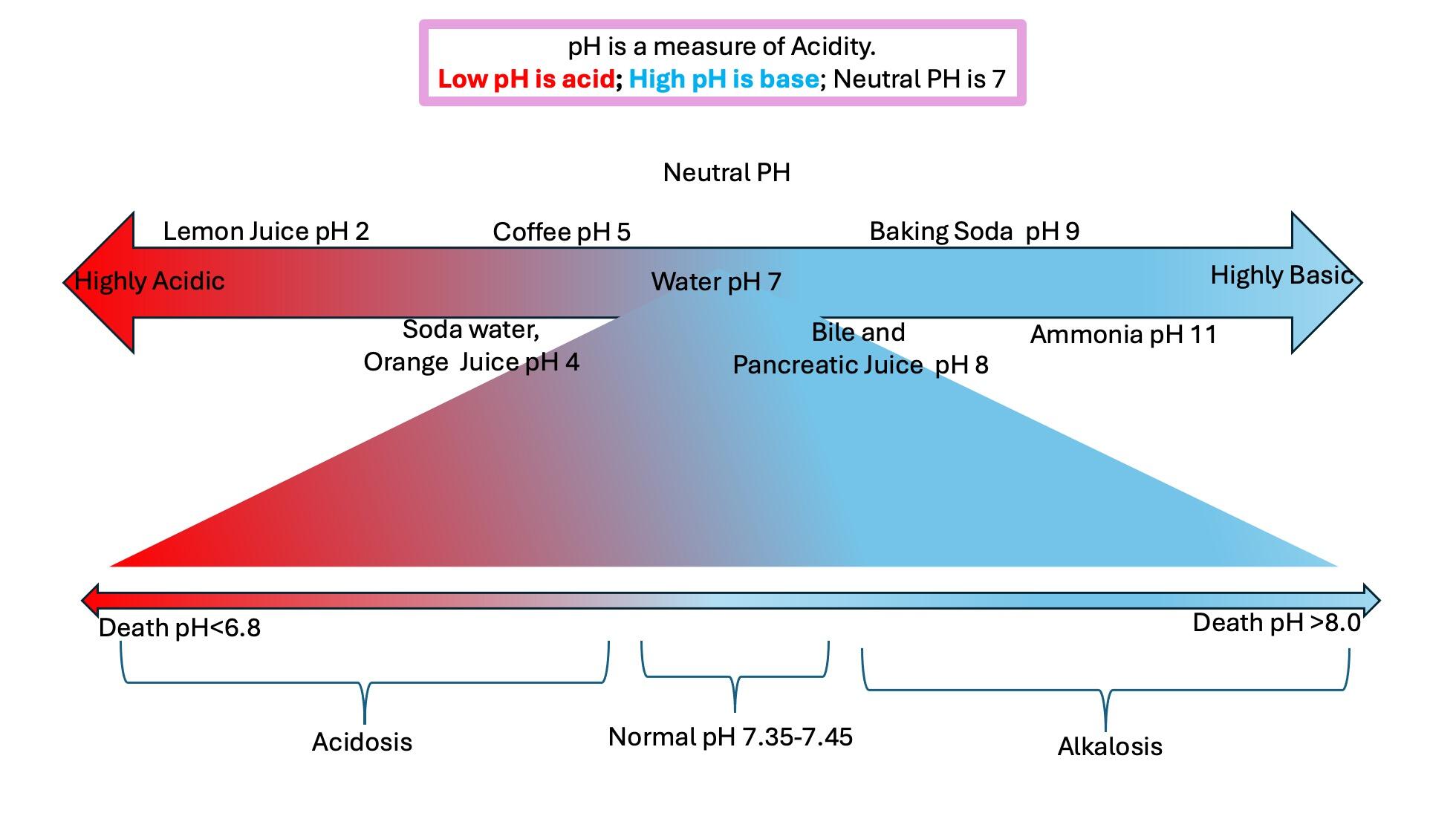
Digestive Juices
December 16, 2024 9:04 am
Fat Soluble Vitamins
April 26, 2020 10:20 am
Written By: Maria Vardapetyan, Eric Baghdasaryan, Osheen Abnous
Vitamins are chemicals that facilitate many processes in the human body such as blood clot formation, good vision, fight infections etc. There are two classes of vitamins. Water soluble vitamins and fat soluble vitamins. Water soluble vitamins dissolve in water. This makes it possible for them to be absorbed through all mucous membranes. Fat soluble vitamins on the other hand do not dissolve or pass through mucous membranes. Fat-soluble vitamins are absorbed in the intestine along with fats in the diet. These vitamins have the ability to be stored in the fat tissues of the human body. Water-soluble vitamins are not stored in the body and have to be taken in daily with the food and dietary supplements. Solubility of a vitamin is not a function of its physical state. There are fat soluble vitamins that have a liquid form and almost all of the water soluble vitamins come in form of pills or powders.
In this article, we are going to focus on fat soluble vitamins. They are all complex molecules made of carbon, hydrogen, and oxygen in different arrangements (see figures 1, 2, 3 and 4). These fat soluble vitamins are vitamin A, D, E and K.
Vitamin A
Vitamin A has a major role in vision, immune function, cell growth, and maintenance of organs such as heart, kidneys, lungs, etc. It plays a pivotal role in the health of our eyes, specifically the retina1. Rhodopsin protein, a major protein that has the leading role in the process of vision, is found in the retina where it allows us to perceive light. This protein requires vitamin A to function properly. Without vitamin A, rhodopsin cannot sense light and thus cannot initiate the process by which vision occurs.

Figure 1: Chemical structure of Vitamin A molecule
Vitamin D
Vitamin D regulates different chemical reactions that are associated with bones, muscles, and the immune system. The simplified way it does this regulation is it helps absorb calcium from dietary nutrients which in turn strengthens the bones, helps neurons exchange signals to move muscles and helps the immune system to fight against viruses and bacteria2.
 Figure 2: Chemical structure of Vitamin D molecule
Figure 2: Chemical structure of Vitamin D molecule
Vitamin E
Vitamin E acts as an antioxidant. Antioxidants are naturally occurring chemicals that neutralize toxic byproducts of many chemical reactions in the human body. When food is consumed and digested, the human body converts it into energy. As a result of metabolism free radicals (toxic byproducts) are formed and are neutralized with the help of vitamin E. In addition, free radicals are also in the environment. Furthermore, vitamin E stimulates the immune system to fight against bacteria and viruses3.
 Figure 3: Chemical structure of Vitamin E molecule
Figure 3: Chemical structure of Vitamin E molecule
Vitamin K
Vitamin K can be obtained from food and dietary supplements. There are two forms of vitamin K: phylloquinone (Vitamin K1), which is found in spinach, kale and other greens and menaquinone-4 (Vitamin K2), which is found in animal products. Vitamin K1 is involved in blood clotting, and Vitamin K2 is involved in bone tissue building. Vitamin K1 is the main Vitamin K in human diet (75-90% of all vitamin K consumed), however, it is poorly absorbed in the body4,5.

Figure 4: Chemical structures of Vitamin K1 and K2 molecules
Absorption of fat soluble vitamins
Polarity describes the inherent charge(positive or negative) or lack of charge for any given substance or molecule. Molecules that are charged are referred to as “polar”, while those that lack charge are “nonpolar”. When discussing solubility, it is important to remember the phrase “like dissolves like”. That means polar (charged) substances like to interact with a polar environment like water, since water contains a slight negative charge. Hence, charged substances are water-soluble. Nonpolar substances on the other hand readily interact with nonpolar environments such as fat, which contains no charge. Therefore, molecules that lack a charge such as vitamins A, D, E, and K are referred to as fat soluble.
Due to their water fearing nature, these fat soluble vitamins cannot simply be absorbed directly into the bloodstream (which is mostly water) like the sugars and amino acids in our diet. As their name suggests, these fat soluble vitamins like to be embedded in fatty droplets, which facilitate their absorption in the following way. Fat soluble vitamins group together with other fat molecules to form fatty droplets, effectively reducing the amount of interaction with the watery environment of the intestines. Therefore, without an adequate amount of fat in your diet, your body is unable to effectively absorb these fat-soluble vitamins. This may be true in an intact anatomy, however, post weight loss surgical patients can not increase their fat soluble vitamin levels by increasing their fat intake. This is due to the fact that a high fat diet causes excessive bowel movement which in turn washes away any vitamins taken by mouth. DS limits fat absorption (thus the great weight loss) which can cause vitamin A and D deficiency that can not be easily corrected with oral supplementation.
As mentioned before, fat soluble vitamins are hydrophobic and nonpolar, which means they are also fat loving or lipophilic. Excess fat soluble vitamins can be stored in the liver and fat tissue. Therefore, these vitamins do not need to be eaten every single day since stores of these vitamins can sustain a person for some time. It may take several weeks or months for our body to deplete these stores of fat soluble vitamins which is why it generally takes a longer amount of time for fat soluble vitamin deficiencies to manifest themselves. The ability to store these fat soluble vitamins in tissues can also lead to vitamin toxicity – marked by an excess of vitamin stores in our body.
Clinical manifestations of A, D, E, K deficiency
| Vitamin | Clinical Deficiency manifestations |
| Vitamin A | Vision Problems
Dryness of the eye |
| Vitamin D | Softening and weakening of the bones
Bone shape distortion Bowed legs (generally in children) Hypocalcemia |
| Vitamin E | Damage to red blood cells
Tissue/organ damage due to inability to supply enough blood Vision problems Nervous tissue malfunction |
| Vitamin K1 | Excessive bruising
Increased bleeding time Small blood clots under nails Increased bleeding in mucous membrane |
| Vitamin K2 | Weak bones
Increased plaque deposits along gumline Arterial calcification |
References
- Office of Dietary Supplements – Vitamin A. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/#. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin D. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminD-Consumer/. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin E. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminE-Consumer/. Accessed April 26, 2020.
- Vitamin K. The Nutrition Source. https://www.hsph.harvard.edu/nutritionsource/vitamin-k/. Published July 2, 2019. Accessed April 26, 2020.
- Beulens JWJ, Booth SL, van den Heuvel EGHM, Stoecklin E, Baka A, Vermeer C. The role of menaquinones (vitamin K₂) in human health. The British journal of nutrition. https://www.ncbi.nlm.nih.gov/pubmed/23590754. Published October 2013. Accessed April 26, 2020.
Stapled Anastomosis
December 30, 2019 11:23 am
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
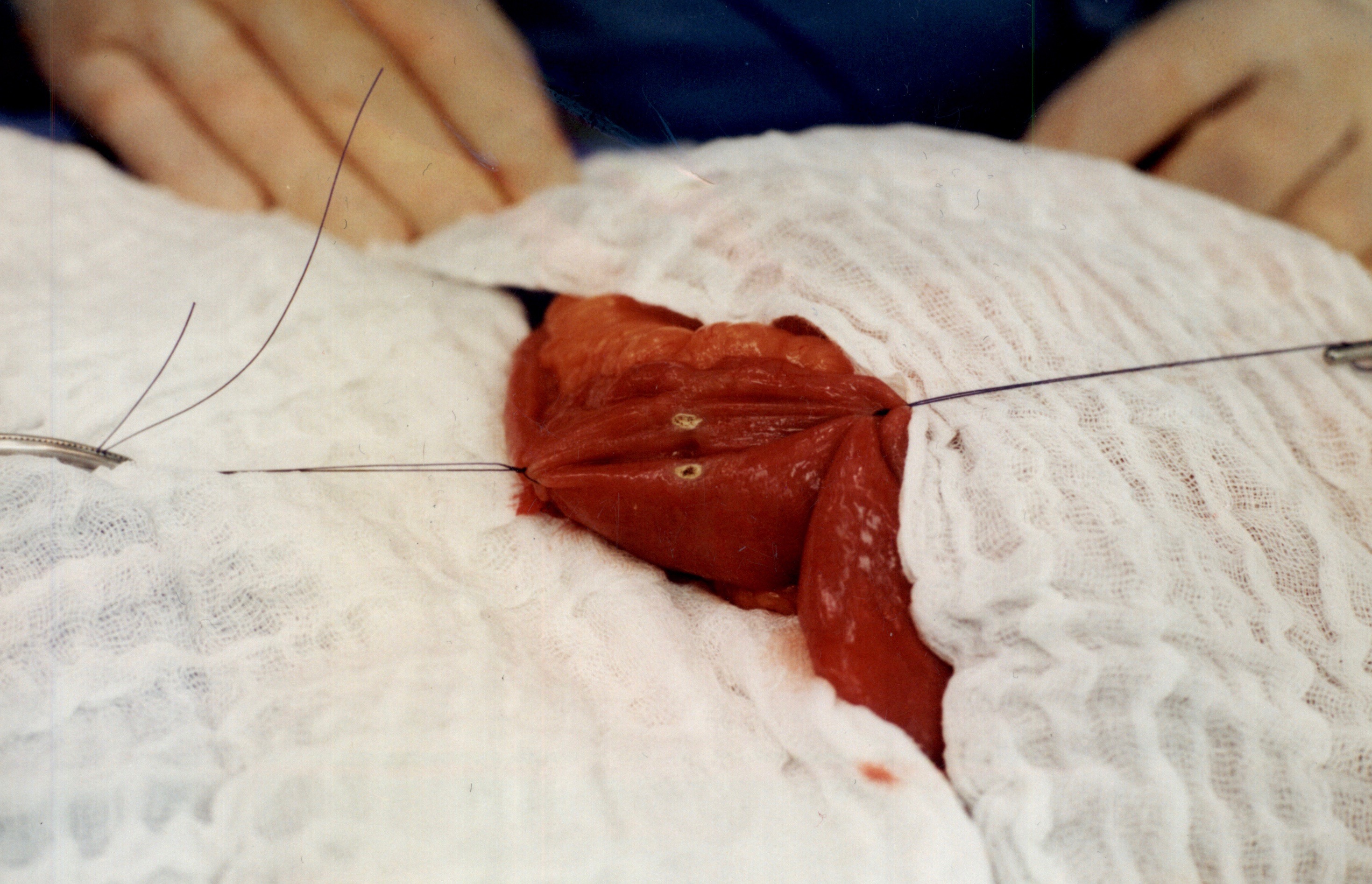
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
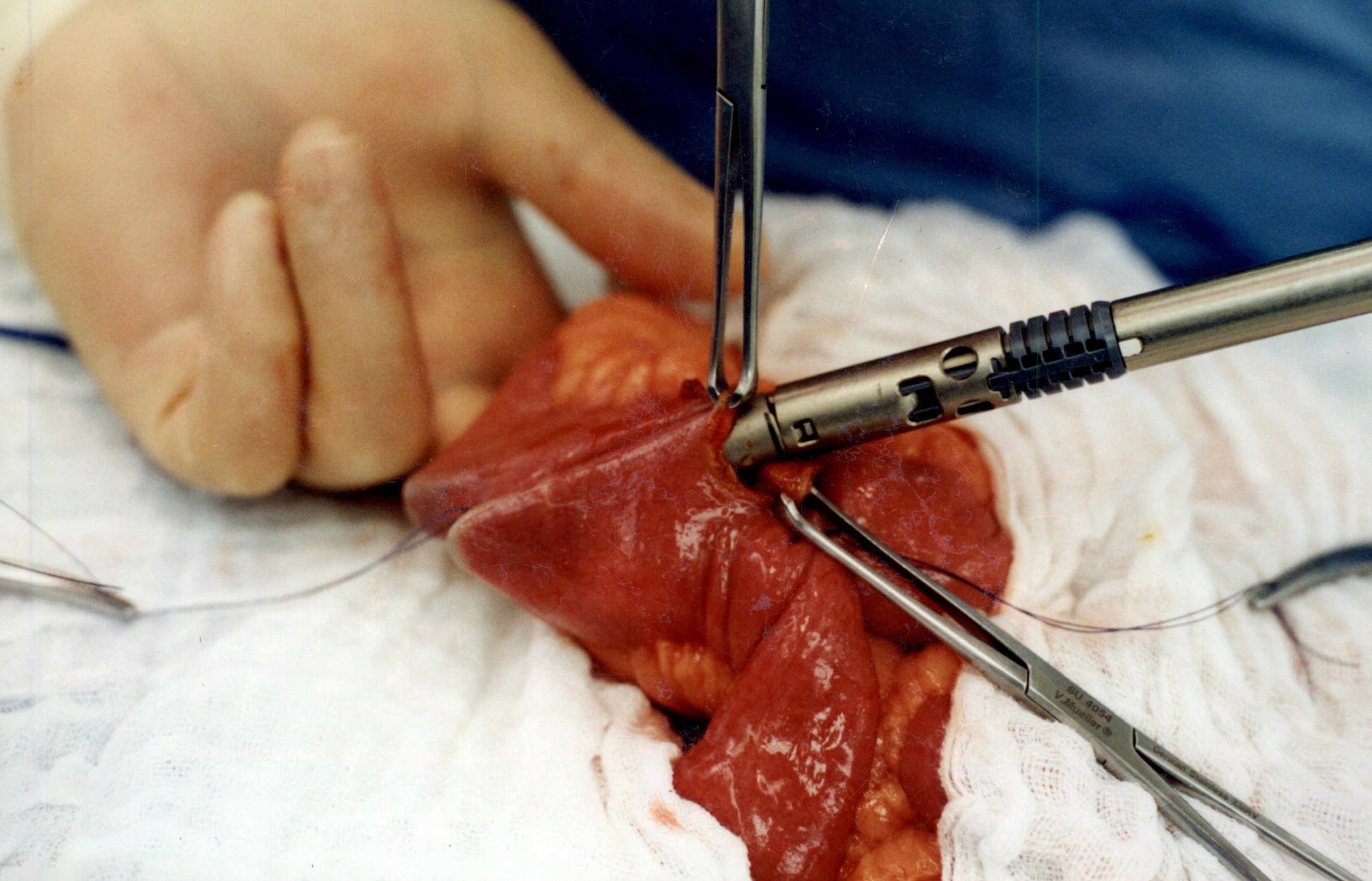
When the stapler is fired in opposite direction, a very wide anastomosis is created.
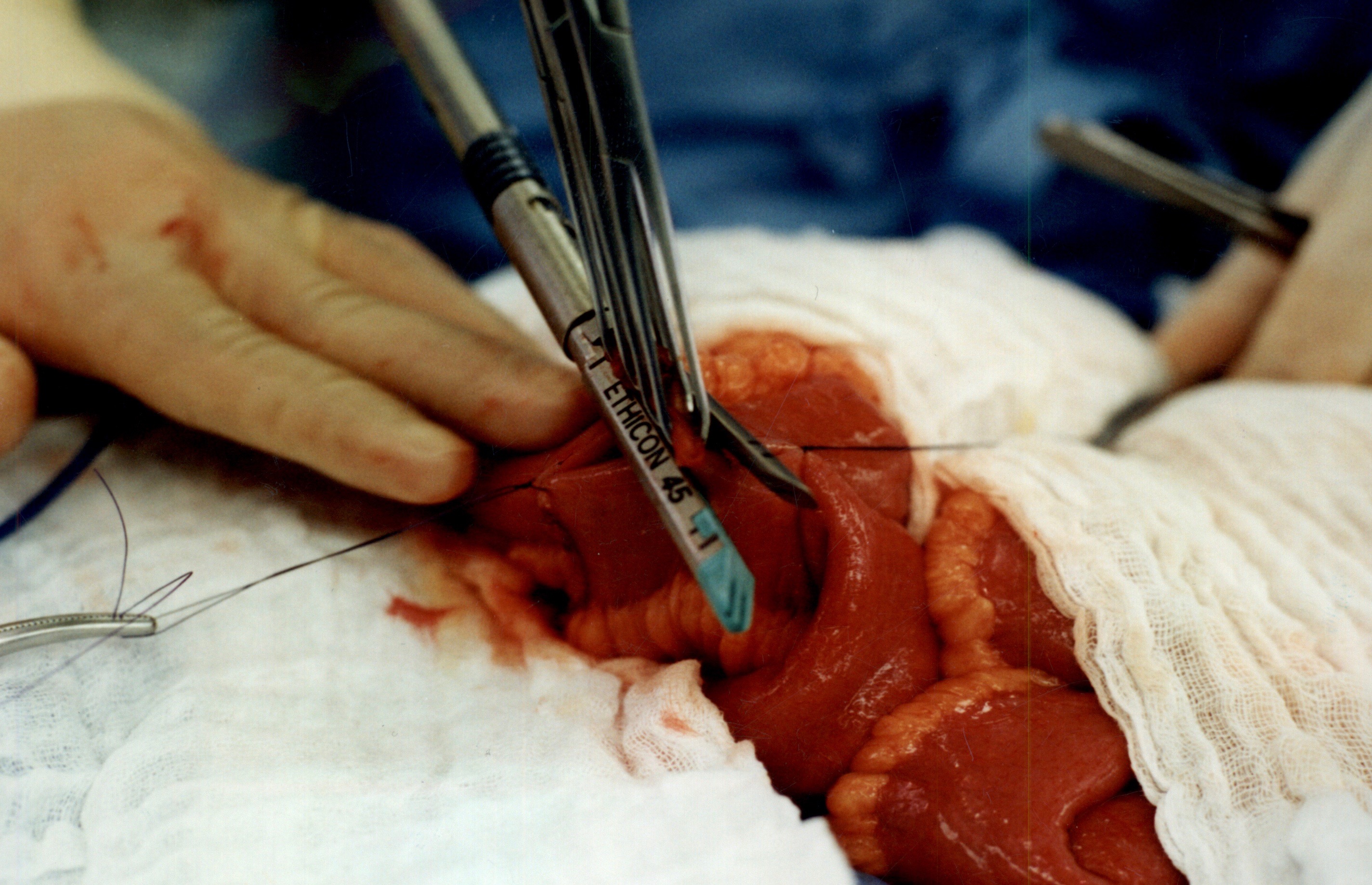
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Dual Testimonial: Cameron’s Gastroparesis surgery & Scott’s Revision of a Duodenal Switch
February 01, 2016 8:04 am
In 2015, I came into contact with the most unique, passionate, urgently responsive; talented beyond belief and caring surgeon I have ever met. Our oldest son who is a 21-year-old cancer survivor, has had nearly five years of medical nightmare as diagnosed with severe gastroparesis resultant from his vagal nerve being severed during a previous Nissen Fundoplication surgery. We didn’t find out that this had happened until nearly two years later and only after a 4 hour gastric emptying test showed that Cameron’s stomach was only about 30% emptied after four hours (should be empty after an hour) due to gastroparesis.
I had heard about Dr. Keshishian on a Bariatric support group page on which I post and get great advice. The surgeon back in Central, IL where we live told us that Cameron needed a subtotal gastrectomy to remove 80% of his stomach! This sounded radical and no way in the world was that going to happen. I was given Dr. Keshishian’s email address so I could consult with him for his advice. It was a Saturday morning around 7 AM Central time when I sent off an email to Dr. Keshishian detailing Cameron’s medical history and current issues. I was in hoping that his office would get the email on Monday and hopefully get back to me within a week. I went out to my kitchen to get a cup of coffee and when I returned I had a missed call with a California area code. Yep, it was Dr. Keshishian. I called back and we talked for 45 minutes. He suggested several things and told me that any good general surgeon in my area could do surgery on Cameron and fix him, well that was the only time he was wrong. We couldn’t find anyone in our area who would do the surgery.
So we talked and agreed that Cameron needed a Roux-en Y drain put in place to physically drain his stomach by way of gravity (not for any weight loss as very little small bowel was bypassed). Dr. Keshishian got us in the next week and we flew out to Glendale where he met with Cameron for an examination on that Monday. On Tuesday, Dr. Keshishian performed surgery to fix Cameron’s herniated diaphragm, loose Nissen wrap, performed the Roux-n Y limb and anastomosis to the stomach. Dr. Keshishian also found a Meckel’s diverticulum (a congenital small bowel defect that can cause internal bleeding and serious issues). The following Sunday, Cameron developed severe pain due to chronic pain from his Cancer treatment and 12 subsequent surgeries, many on his abdomen. Dr. Keshishian saw Cameron in the ER and spent 3 hours fixing Cameron’s pain issue and making sure he was medically sound so we could fly home the next day.
Today, Cameron has very little to no issues which you wouldn’t have believed possible six months earlier. In the past, he had violent retching, dry heaving and bad nausea daily which had him severely incapacitated and very depressed due to a feeling of hopelessness and pain from the Gastroparesis. He didn’t believe he had a chance at a normal life but Dr. Keshishian gave Cameron his life back. We are eternally grateful for your huge heart and talent Dr. Keshishian. Thank you!
During our time in Glendale in 2015 for Cameron’s surgery Dr. Keshishian and I began discussing my situation. I had been given a virgin Duodenal Switch performed by a surgeon in Illinois in September of 2013. A year later in 2014 and 180 lbs lighter, I ended up in the hospital as I was passing out. I had a resting heart rate of 35 BPM, a blood pressure in the 75/40 range and incredibly bad labs including anemia, low copper, low zinc, and dangerously low albumin and total protein. A full cardiac work up was completed and I spent a week in intermediate care. Why? I was extremely malnourished even though I was consuming 200-250 grams of protein daily! Why was I malnourished? Because my original surgeon performed a “cookie cutter DS” on me where he didn’t measure my small bowel and arbitrarily gave this 6’2 man a 100 cm common channel and a 150 cm Alimentary limb. Way too short on the AL! Had the Hess method been followed (the only way the DS should be allowed to be completed) my CC would have been 100 cm (that was okay) but my Alimentary channel should have been 275 cm! Simply put, my absorbing portion of small bowel was 34% and the Biliopancreatic limb (non-absorbing) was 66%. It should have been a 50/50 ratio with 100 cm CC, 275 cm AL and a 375 cm BPL. In order to combat my severe malnutrition that September of 2014 I went on a pancreatic enzyme (CREON) to assist my nutrient absorption. I was taking with meals right around 400,000 IU’s of CREON (a boat load) and this was barely keeping my nutrients in range and lab values barely in range. After speaking with Dr. Keshishian, he recommended that I give it until around September of 2015 to see if my absorption increased enough to where a revision wouldn’t be required. Towards the end of July, I all of the sudden lost nearly 20 pounds in two weeks from my already frail and scrawny body. I saw my surgeon in Peoria as I was very alarmed; and I had been having bad cramping and other issues point to a possible bowel obstruction His exact words to me were “see me in 30 days, you are like the DS poster boy of good nutrition”. As you can imagine I found that completely unacceptable and soon as I was out of that appointment I emailed Dr. Keshishian. He told me that if I couldn’t get a revision ASAP I would need to immediately go on TPN. Two weeks later my wife and I landed at LAX and were in Glendale on Monday morning for an exam with Dr. Keshishian.
The job Dr. Keshishian did describing what he was going to do, and of course this was a visual presentation with Dr. Keshishian drawing (you know Dr K’s love of drawing) out for us what he was going to do. He thoroughly explained for my wife and I so she was comfortable with what was going to happen and we fully understood what he was going to do. Doc also found an umbilical hernia that he was going to repair and I had an anal fissure as well that wouldn’t heal so we discussed what he would do to examine and possibly fix during my revision surgery. The next day Dr. Keshishian performed surgery where he fixed the umbilical hernia, measured my total small bowel length to determine appropriate channel lengths and found an repaired a huge mesenteric defect (intestinal hernia and Dr K has a picture of my guts with the huge hole in the mesentery that he has posted on his blog discussing intestinal hernias and blockages), fixed my fissure (Thank you!) and put in a side by side anastomosis that effectively lengthened my AL by 125 cm and my CC by 25 cm worth of absorption. This put my absorbing intestine to BPL ratio where it should have been in the first place (50/50 ratio).
I am pleased to say that I immediately went off the CREON and my absorption and subsequently my lab values improved tremendously. At surgery on August 18, 2015 I weighed a whopping 170 lbs. Today I am weighing in at 183 pounds and well on my way to Dr. Keshishian’s suggested optimal weight target of 205.
Dr. Keshishian is absolutely amazing and the best in the world when it comes to performing the Duodenal Switch and revision to DS Surgery (Band to DS, RnY to DS, Channel extending revision to DS). I would recommend Dr. Keshishian to any patient who needs a virgin Duodenal Switch to get their health back and especially to those who were sold a garbage RnY or Crapband procedure that ultimately failed you (it failed you, you did not fail). In fact, I am trying very hard to convince my brother and Step Mother to fly to Glendale and have Dr. Keshishian perform a Duodenal Switch on them. They very much need it for their health and Dr. Keshishian is the best in the world having performed over 2,000 DS procedures.
I don’t say this lightly. Ara, you are one of the finest human beings I have ever had the good fortune of knowing and your surgical skills are second to none. I really do admire and love this gentleman like a brother and consider him to be a friend. Thank you for using your incredible skill to fix my health issues resultant from the failed cookie cutter Duodenal Switch I was given two years earlier by another surgeon. Had I met you back then and knew what I know now, you would have performed my virgin DS and I would not have suffered for two plus years. Thank you from the bottom of my heart, Dr. K!
Hypertrophy of Small Bowel and Weight Gain Years After Duodenal Switch
August 21, 2015 7:53 pm
Duodenal switch (DS) operation results in the highest success rate of all weight loss surgical procedures. Patients, over time, will experience some weight gain many years after DS procedure. There are a number of suspected mechanisms that may be responsible for the weight gain:
1-Ageing may slow the metabolism and the activity down.
2-Over time patients may not be as adherent to healthy dietary and lifestyle changes as they may have been immediately after surgery.
3- Hypertrophy of the alimentary and common channels over time increases in surface area f allowing greater caloric absorption leading to increased weight gain.
It has been demonstrated in bowel resection studies, as well as rat studies, that the nutrient stimulated regions of small intestine increase villus height and total weight, crypt depth and proliferation as well as wall thickness, as an adaptation to compensate for the loss of absorptive capacity in the resected bowel. This observation may be applied to DS procedure as seen in histological slides from a patient who had to have an operation done requiring bowel resection. The segment of the bowel resected included the junction of the biliopancreatic, common and alimentary limbs.

Duodenal Switch and Fat in The Diet
May 21, 2015 12:35 pm
When I perform the duodenal switch operation, the common channel is a percentage of the total small bowel length and I also account for the patient’s metabolic rate. Two individuals with a BMI of 50, should not have the same common channel. If we compare two patients, one of them is a 20 years old male who is 6’2″ and the second patient is a 60 year old female who is 5’4″, we can see how this applies. These two patients have very different metabolic needs and requirements. When the Duodenal Switch is performed in this fashion, the common channel based on a percentage of total small bowel length and metabolic needs, the patients post op diet works best when it is a well balanced, protein based diet. The basic principals are : Hydration (water), Protein and Everything else, low carb, avoid artificial sweeteners, avoid carbonated drinks, have frequent smaller meals and avoid processed food. Listen to you body as to what it tolerates and what it doesn’t. This is what I recommend for my patients.
I am not aware of any scientific evidence that proves any benefit to excessive amounts of fat for DS patients who have had their length of the common and alimentary bowels based as a percentage of the total length.
My recommendation are to have a well balanced high protein diet. I do not recommend a low fat diet, except in the healing phase after surgery. However, there is no reason to consume excessive amounts of fat long term.
High fat diet is used to facilitate bowel movements for some patients who have constipation. It may be prudent to try and identify what may be causing the constipation and correct or eliminate them before one resorts to a very high fat diet as a “treatment” for constipation after Duodenal Switch. The possible causes for constipation after duodenal switch may be metabolic-organic (where some patients have infrequent bowel movements before DS, hypothyroidism), length of the common and the Alimentary channels and medications (pain meds, narcotics, antidepressants).
In addition, Medium Chain Fatty Acids do not require bile salts to be absorbed and are directly absorbed into the Portal Vein in the liver. Medium Chain Fatty Acids are not malabsorbed post Duodenal Switch. Medium Chain Fatty Acids included Caproic acid, Caprylic acid, Capric acid, and Lauric acid. Commonly found in varying amounts within coconut oil and palm oil. MCT supplement is made with Medium Chain Fatty Acids.
In summary, I recommend that Duodenal Switch patients who have had surgery with our practice have a high protein balanced diet. I do not recommend avoiding fat, or going on a low fat diet. I am not sure if there a reason to consume excessive amount of fat, which may in fact have unexpected metabolic and nutrient consequences.
Every patient, as their weight stabilizes, will find what works and what does not work for them. Some patients will tolerate a higher fat intake and other will not be able to tolerate higher fat intake.