Tag: malnutrition
Feeding Tube with Duodenal Switch
February 03, 2025 9:53 am
The surgical changes following the revision of the failed gastric bypass to the duodenal switch or a primary duodenal switch require an evident appreciation and understanding of the anatomy and physiology of placing a feeding tube and managing the nutritional status. There are different places where a feeding tube can be placed.
1-A feeding gastrostomy tube endoscopically cannot be placed because of the transected post-pyloric duodenum (The image viewed on a desktop or a laptop allows the scroller on the image to move)
2-An orogastric or nasogastric tube should only use an elemental feeding formula. This is because the food in the stomach is prevented from mixing with the biliopancreatic juices, which will not be adequately absorbed.
3-A feeding Jejunostomy can only be insured surgical post ligament of traits. This cannot be done endoscopically because duodenal switch transaction post pyloric small bowel to prevent mixing of the biliopancreatic secretion.
Additional informationVitamin Toxicity
December 17, 2024 1:36 pm
Patients are frequently asked to explain why they take high fat- or water-soluble vitamin doses. They are have often been scared by their well meaning healthcare providers that their higher levels of vitamin supplements will end up with vitamin toxicity.
Let’s clarify one point: there is such a thing as too much vitamin.
However, the point that is often overlooked in teaching within professional schools (medical, nursing, pharmacy, etc.) and drug manufacturers is that recommendations are based on “how much to take” and not how much is needed to keep a patient’s blood level in the normal range.

This table highlights how toxicity is described and what requirements are recommended. Vitamin toxicity is seen rarely in post-weight loss surgical patients who take them proactively in as many doses as needed to get their blood levels in the normal range. I see more patients in the office who suffer from low vitamin levels, such as vitamin D and A levels (duodenal switch and sleeve), than any patient with high or toxic levels of any vitamins.
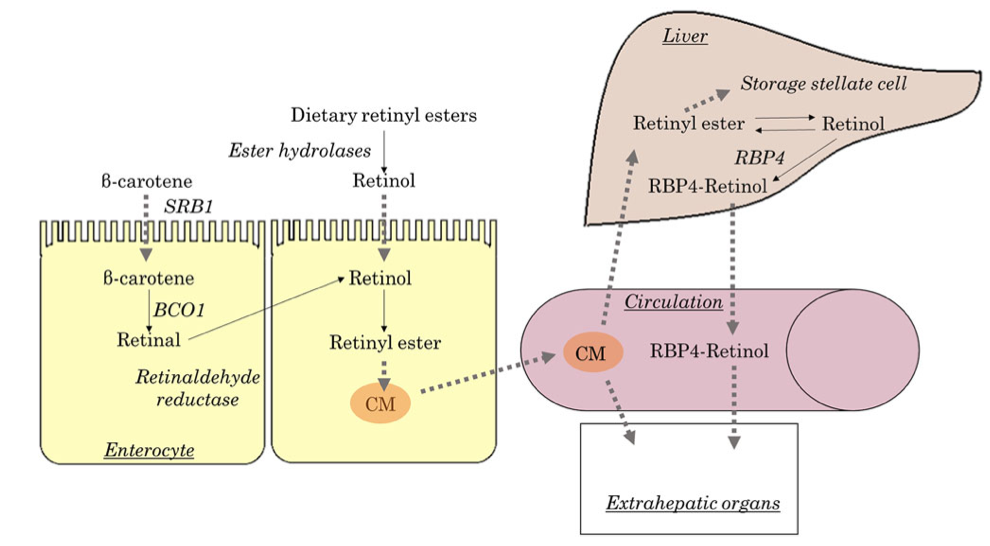
Here is an example of critical vitamin A deficiency and night blindness and how, with aggressive large-dose supplementation, her condition was corrected.
Too Much Protein & Protein Metabolism
December 17, 2024 12:40 pm

Digestive Juices
December 16, 2024 9:04 am
Covid 19:Anesthesia, Weight Loss Surgery and Malnutrition
October 30, 2021 8:52 am
As the COVID-19 pandemic is charting its course into 2022, as health care providers, we have had to adapt and adjust to the transient and shifting environment. Testing for COVID-19 has been in place, and is now part of the standard for preoperative work-up. In addition, covid testing will likely be part of screening any surgical procedure for the foreseeable future.
The challenge of pandemic control is the large pockets of populations in the US and worldwide that do not have protection against the virus and are not vaccinated. Vaccination provides the only proven long-term protection against COVID-19 infection and its long-term persistent health effect. In addition, the complication rate reported in scientific journals is negligible compared to the complication and death rate from the COVID-19 infection.
There are implications of covid infection and general anesthesia published in peer-reviewed journals. The increased risk of general anesthesia after covid infection is related to the severity of the initial infection and the extent of the treatment required, and the persistence of the post covid symptoms, including shortness of breath, fatigue, and laboratory finding elevated inflammatory markers. Long after resolution of the acute COVID-19 symptoms, the most common persistent complaints are fatigue, shortness of breath, Joint and chest pain; and all these increase the risk of post-operative complications (Carfì et al., 2020)
The required delay for surgery may be as short as 2-4 weeks to as long as six months or longer if the persistent symptoms are present. Surgery may not be avoidable in a critical life-threatening situation and may be necessary even with a much-increased risk of complication (Collaborative, 2020). Recovery post-COVID-19 may not be complete with the resolution of the initial symptoms (Dexter et al., 2020)
Recent publications and scientific presentations have also shown the protection that weight loss surgery and maintained weight loss provide in those who come down with the COVID-19 infection (Aminian et al., 2021). However, the rate of weight gain, lack of weight loss is worse for weight loss surgical patients post COVID-19 disorder (Bullard et al., 2021; Conceição et al., 2021). Furthermore, patients with COVID-19 infection post weight loss are at a higher risk of malnutrition (di Filippo et al., 2021; Kikutani et al., 2021). Up to 40% of patients have malnutrition if hospitalized with COVID (Anker et al., 2021).
To summarize, Weight loss and weight loss surgery reduce the severity of the initial COVID-19 infection. However, it increases malnutrition risk, requiring nutritional support and surgical interventions in non-responsive cases.
REFERENCES:
Aminian, A., Fathalizadeh, A., Tu, C., Butsch, W. S., Pantalone, K. M., Griebeler, M. L., Kashyap, S. R., Rosenthal, R. J., Burguera, B., & Nissen, S. E. (2021). Association of prior metabolic and bariatric surgery with severity of coronavirus disease 2019 (COVID-19) in patients with obesity. Surgery for Obesity and Related Diseases, 17(1). https://doi.org/10.1016/j.soard.2020.10.026
Bullard, T., Medcalf, A., Rethorst, C., & Foster, G. D. (2021). Impact of the COVID-19 pandemic on initial weight loss in a digital weight management program: A natural experiment. Obesity, 29(9). https://doi.org/10.1002/oby.23233
Conceição, E., de Lourdes, M., Ramalho, S., Félix, S., Pinto-Bastos, A., & Vaz, A. R. (2021). Eating behaviors and weight outcomes in bariatric surgery patients amidst COVID-19. Surgery for Obesity and Related Diseases, 17(6).
Di Filippo, L., De Lorenzo, R., D’Amico, M., Sofia, V., Roveri, L., Mele, R., Saibene, A., Rovere-Querini, P., & Conte, C. (2021). COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clinical Nutrition, 40(4). https://doi.org/10.1016/j.clnu.2020.10.043
Kikutani, T., Ichikawa, Y., Kitazume, E., Mizukoshi, A., Tohara, T., Takahashi, N., Tamura, F., Matsutani, M., Onishi, J., & Makino, E. (2021). COVID-19 infection-related weight loss decreases eating/swallowing function in schizophrenic patients. Nutrients, 13(4). https://doi.org/10.3390/nu13041113
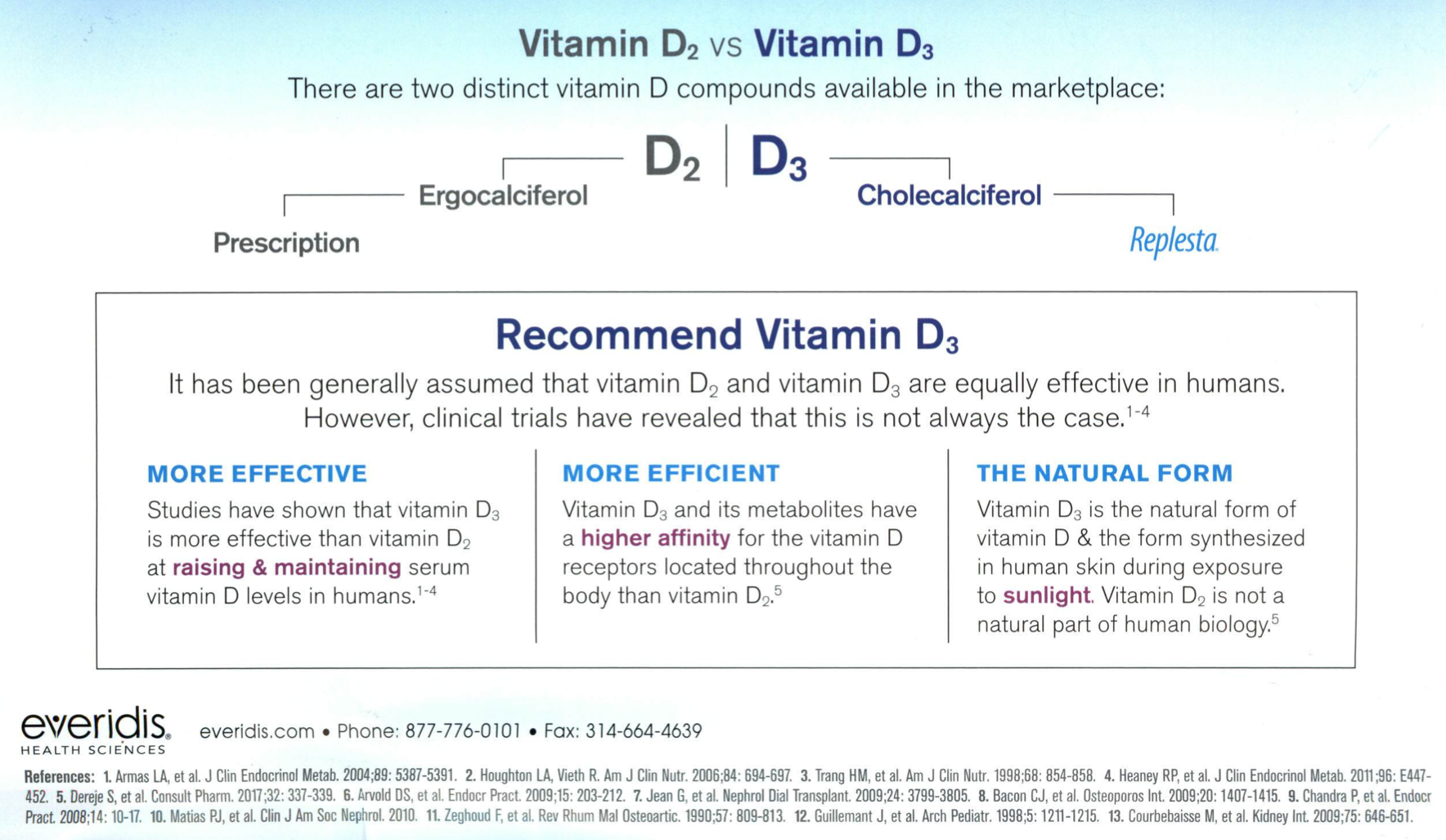
Over the Counter Vitmain D3 better than the Prescription Vitamin D2
August 30, 2021 10:41 am
Vitamin A and Wound healing
December 21, 2020 9:37 am
Night Blindness – Vitamin A Deficiency
Nyctalopia (Night Blindness) An Early Sign of Vitamin A Deficiency with VideoA recent article discusses the types and function of vitamin A. As with the pandemic of COVID-19 continuous to stress our body and mind, we must stay vigilant with our nutritional status. Therefore, Vitamin supplements are critical in maintaining a robust immune system. For some, oral supplements are adequate; others may require injectable forms. If the oral supplements do not correct the vitamin A levels, please contact your primary care or our office to available vitamin A injections.
Copper Metabolims And Weight Loss Surgery
May 01, 2020 12:31 am
Written By: Osheen Abnous, Maria Vardapetyan, Eric Baghdasaryan
Copper is an essential element to all organisms, and it is a contributor in several enzymes vital to the function of hematopoietic, vascular, and skeletal tissues, as well as the structure and function of the nervous system.
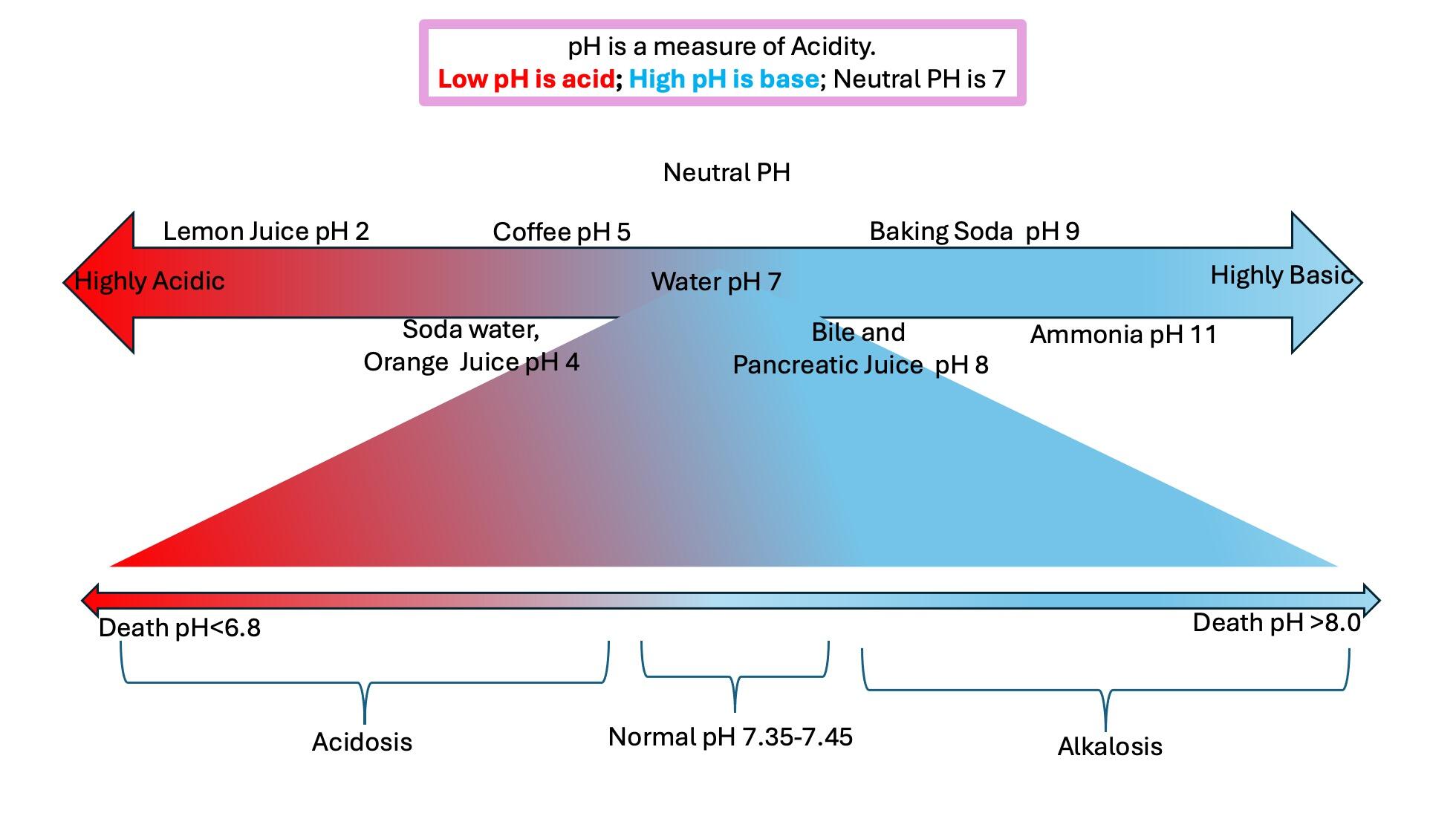
As a crucial metal, copper plays an important role in chemical reactions throughout the human body; this includes the central nervous system. Enzymes are substances that facilitate chemical reactions. There are many copper-dependent reactions in the human body. In humans, the major site of absorption of dietary copper is still unclear. Copper in humans is absorbed in the proximal small bowel, duodenum, and ileum. This is after it has passed the acidic environment of the stomach.
Copper deficiency can be caused by malnutrition, prematurity, parenteral or enteral feeding without copper supplementation, gastrectomy, and excessive zinc therapy. The common causes of copper deficiency have been zinc supplementation, and changes to the PH (acidity) of the stomach. This can be the result of the alteration of the stomach anatomy, and by chronic acid suppression by proton pump inhibitors (antacids), and similar medications. Physicians need to be alert with patients who show signs of copper deficiency or are at a high risk of developing a copper deficiency.
It is important to raise greater awareness about copper deficiency because there is a growing number of patients undergoing surgeries for obesity, as the occurrence of copper deficiency will increase in the future.
Studies of patients who have had weight loss surgery in the past experience common symptoms such as pain involving the feet, gait abnormality (unusual walking), lower limb weakness, and recurrent falls. Common lab results include unusually low serum copper and serum ceruloplasmin levels. In some cases, elevated zinc levels are also present. Treatment includes cupric sulfate infusion until normal copper levels are reached, which then need to be maintained for the future. Vitamin B-12 deficiency has also been reported as a possible cause of myelopathy, which is a nervous system disorder that affects the spinal cord. As stated earlier, neurological damages are often irreversible and cause permanent damage to patients. Early diagnosis from physicians is crucial for patients who have undergone gastric bypass surgery, and the sooner they are diagnosed, the less permanent damage the patient will endure.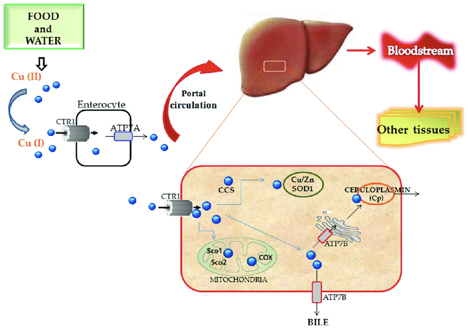
Case Discussions:
A 49-year-old woman had gastric bypass surgery for obesity 24 years age. She presetend with increasing lower limb stiffness and numbness. Additionally she reported tingling of the feet. As her pain continued to increase, she began using a walker, and her symptoms continued to worsen. After undergoing a neurological examination, results showed that the patient had increased lower limb tone and an absent perception of vibration at the toes and ankles. Laboratory results showed that the patient had copper levels barely detectable. This included serum copper and serum ceruloplasmin levels. In addition, the patient had reduced serum carotene (vitamin A) levels.
The patient received cupric sulfate intravenously daily through an 8-week period. After each daily infusion of cupric sulfate, the patient reported to have slight decreases in numbness and an increased tingling sensation. After the 8-week period, lab results showed that serum copper levels were normal and are needed to be maintained. Her night blindness was corrected by vitamin A injections.

In another case, a 53-year-old woman had symptoms of abnormal gait (abnormal walking) and anemia (lack of healthy red blood cells), and was seen for evaluation. The patient complained of pain in the lower legs, which would worsen over time and move up towards her thighs. As her ability to walk continued to worsen, the patient resorted to using a wheelchair. Her medical history consisted of an RYGB surgery for obesity. The only significant supplementation she received was 1000 μg vitamin B12 subcutaneously for several years. She had absent positional and vibratory sensation in the lower extremities to the knee. In addition, touch sensation was decreased. Laboratory examination revealed an elevated serum zinc level, and extremely low serum copper and ceruloplasmin levels.
For treatment, the patient received intravenous copper over a 6-day period, was discharged home, and then received weekly intravenous copper infusions thereafter. After a month of receiving intravenous copper, serum copper levels returned to normal. In addition, the patient’s pain in the lower leg improved, but vibratory sensation remained absent in the same area. Four months after being discharged from the hospital, the patient began walking with a cane.
Medication Absorption After Weight Loss Surgery
March 30, 2020 8:01 am
Weight loss surgical procedures, in one form or another, achieve the desired effect of weight loss by altering absorption of fat, protein, and carbohydrates. This results in decreased total absorption of required calories.
An unintended consequence is the altered absorption of medications. Frequently I am asked about the specific medication. Usually the answer is vague since the information is limited on specific medications. If the desired effect is not achieved, then it is probably not being absorbed well. Specially, if the same dose of the same medication working well before surgery.
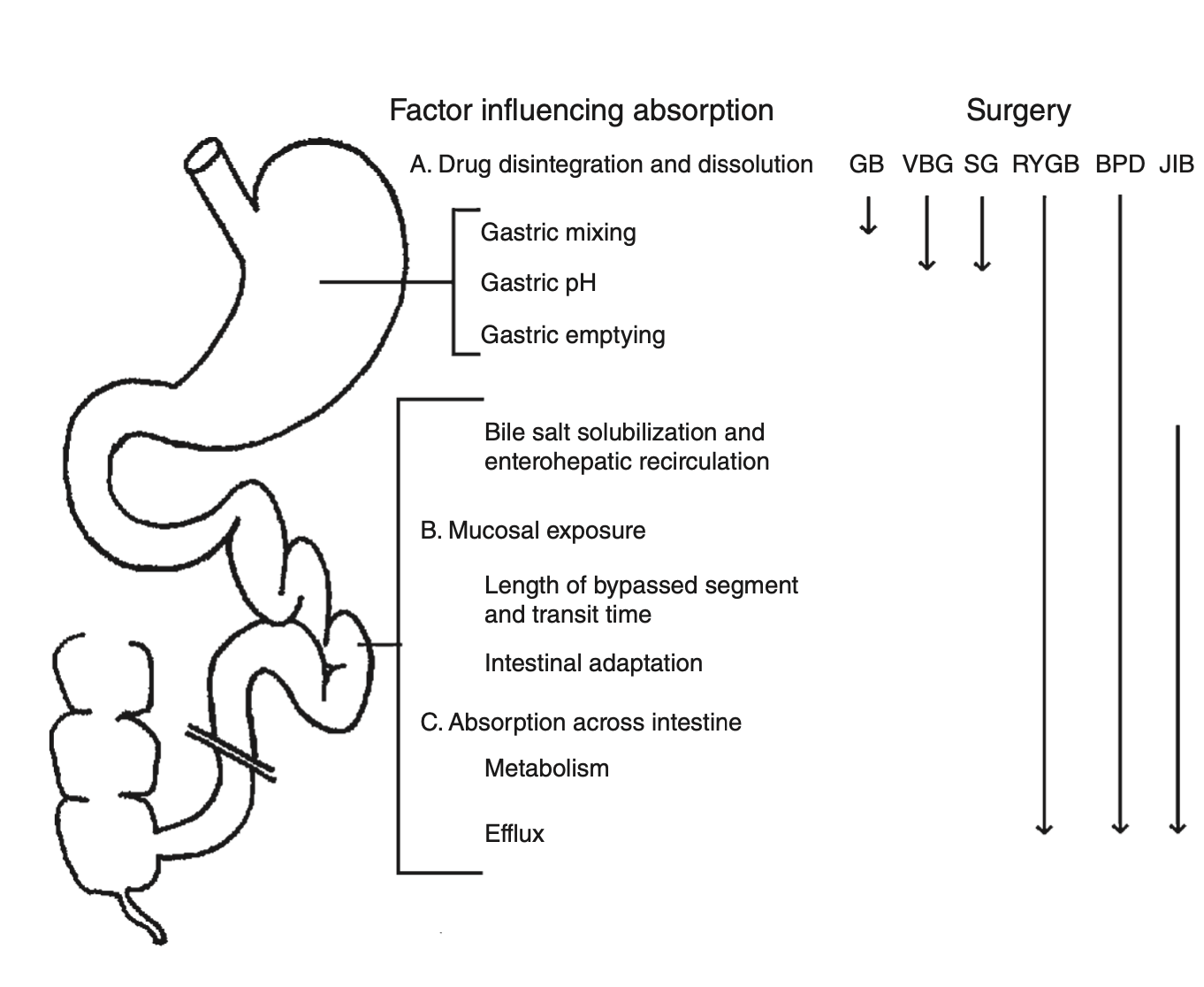
There is a summary article about the Theoretical absorption pattern of different weight loss surgical procedures.
Copper Deficiency Intravenous SupplementationExclusive Member Content
November 17, 2019 9:23 pm