Category: Anatomy
Surgery for Reflux
August 02, 2025 6:58 pm
Surgery for Reflux
Gastroesophageal reflux disease (GERD) is a common gastrointestinal problem in both the general population and post-weight-loss surgical patients.
The general population may have GERD symptoms with weight gain, pregnancy, hiatal hernia, Helicobacter pylori infection, gallstones, ulcers, motility issues of the esophagus or stomach, and other conditions. With proper workup, they all have their specific treatment plans. In a post-weight-loss surgical patient, some of the exact causes may be present in addition to those that may be specifically related to the type of surgery and its unique side effects and complications.
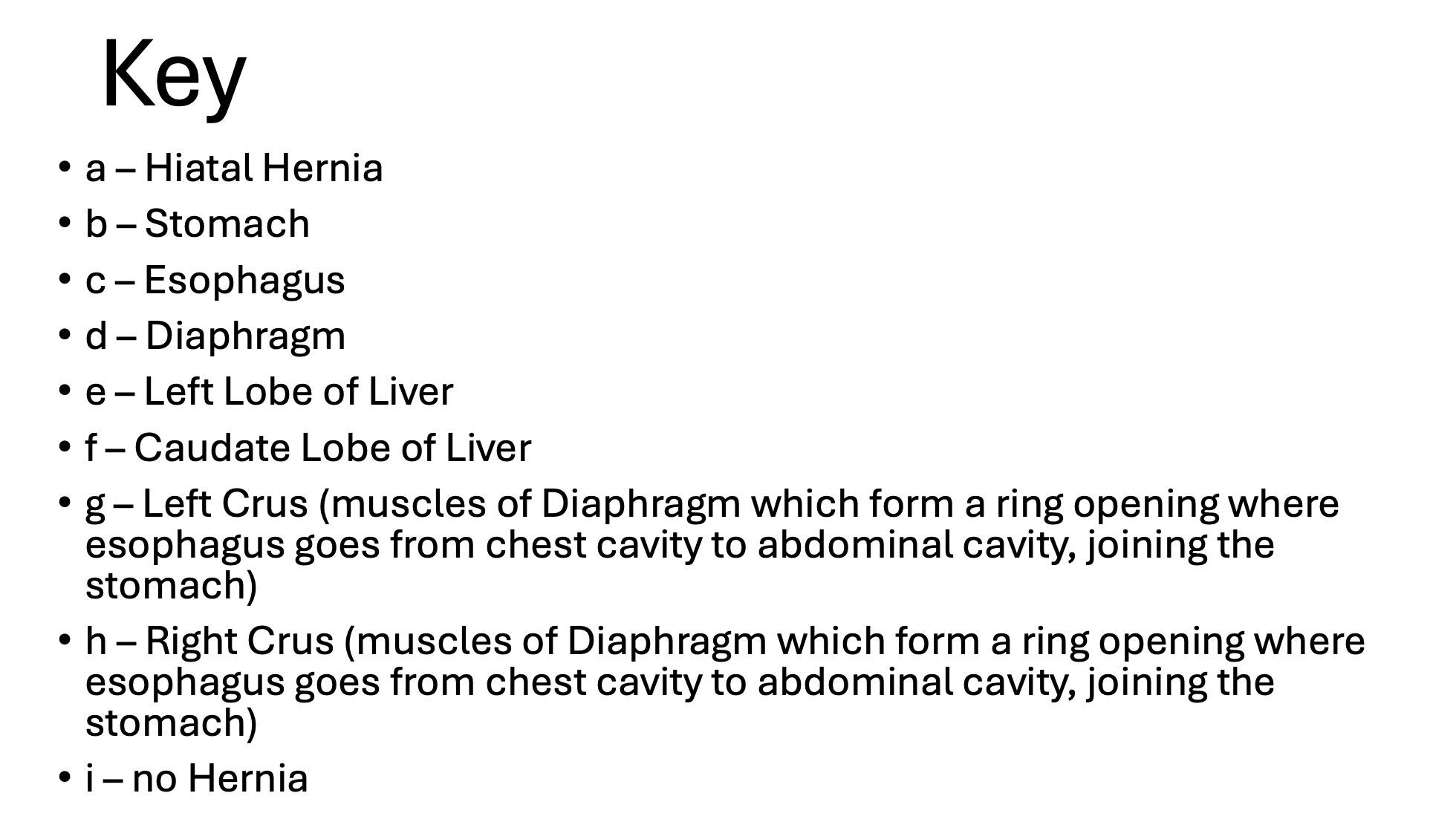
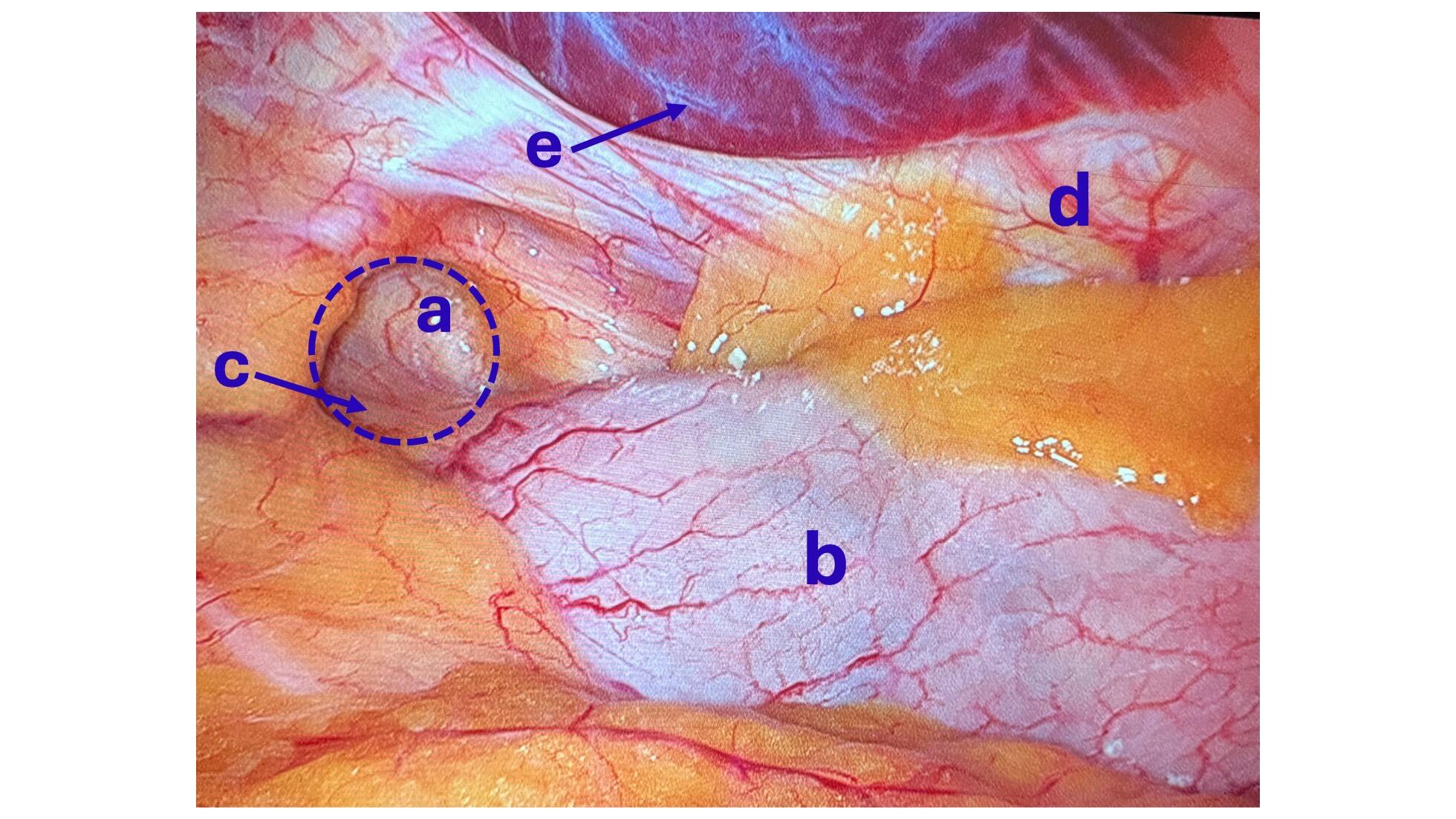
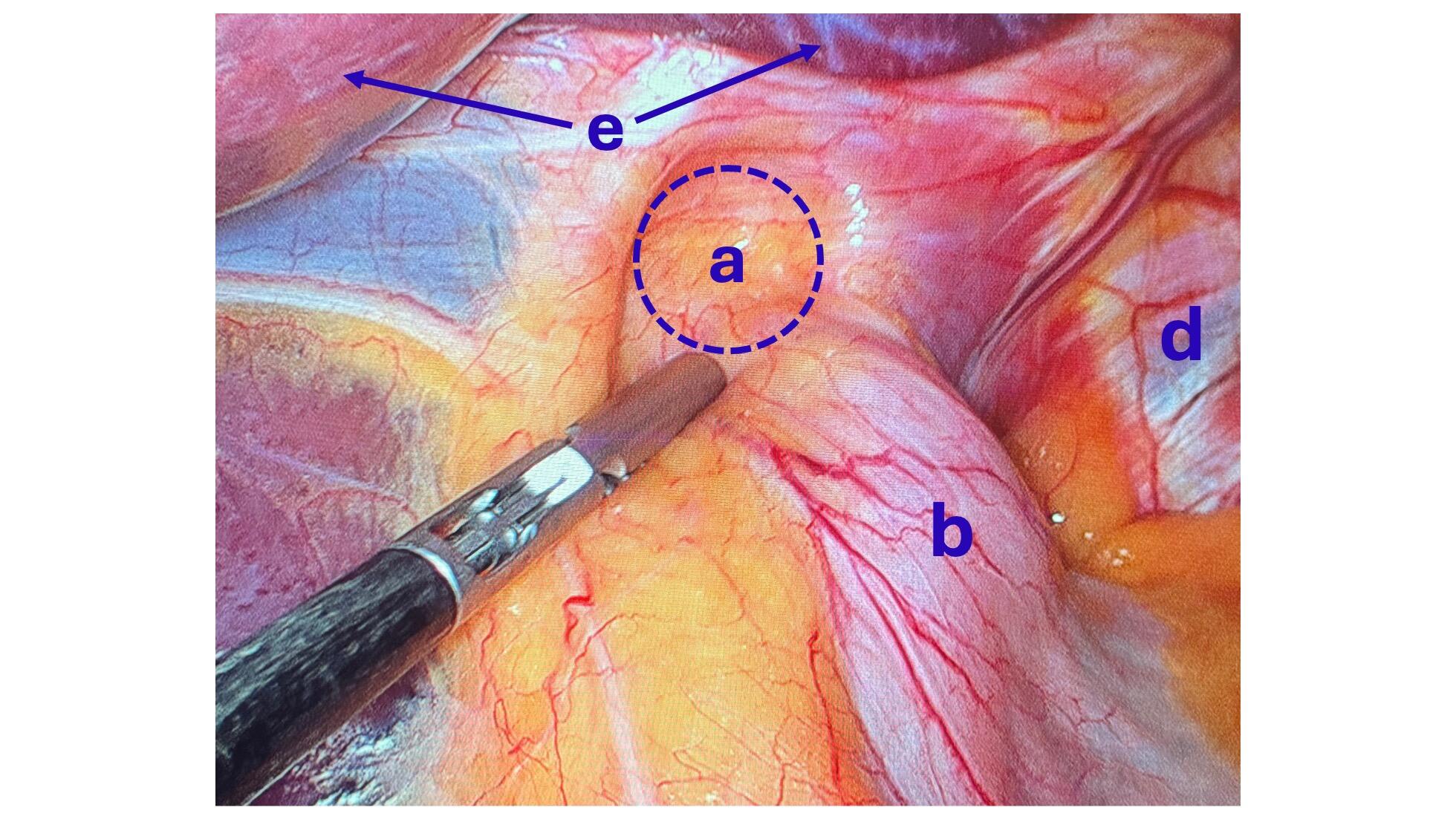
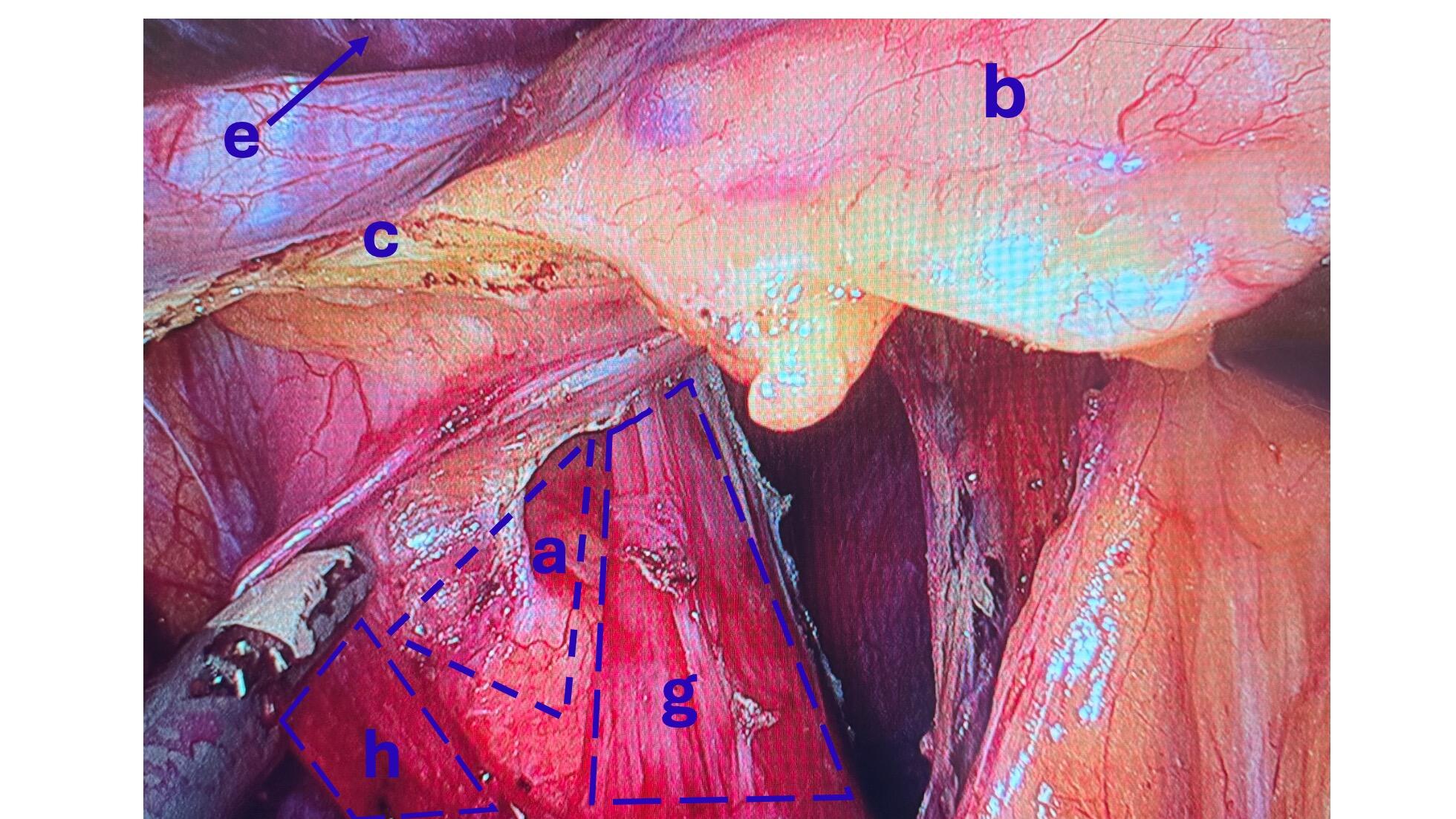
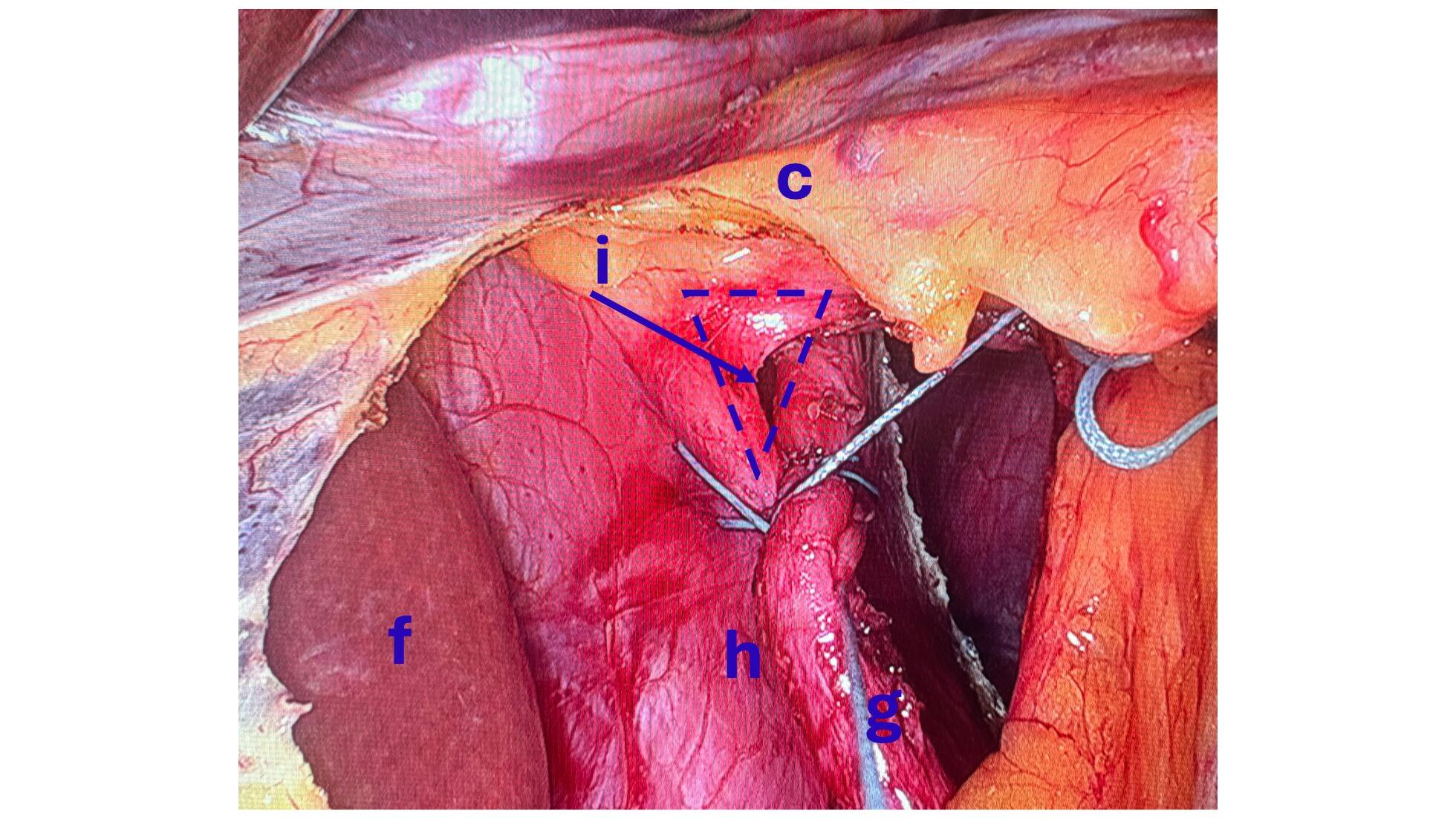
There is a subset of patients with hiatal hernia who should undergo surgical repair, but do not. There has been a series of publications from over 15 years ago that have been embraced by the gastroenterologist who frequently, incorrectly, dismisses Nissen fundoplication as an effective surgical tool for the treatment of GERD and hiatal hernia.
The treatment for GERD with a hiatal hernia, regardless of size, is Nissen Fundoplication and not lifelong use of proton pump inhibitors (omeprazole, pantoprazole) and other classes of medication. It should be noted that these medications were never approved for long-term use and can cause significant metabolic and gastrointestinal side effects.
Recent publications have shown that not only the old data that gastroenterologists frequently rely on was not reliable, but also that surgery is very safe and effective with a very low rate of short and long-term complications.
Feeding Tube with Duodenal Switch
February 03, 2025 9:53 am
The surgical changes following the revision of the failed gastric bypass to the duodenal switch or a primary duodenal switch require an evident appreciation and understanding of the anatomy and physiology of placing a feeding tube and managing the nutritional status. There are different places where a feeding tube can be placed.
1-A feeding gastrostomy tube endoscopically cannot be placed because of the transected post-pyloric duodenum (The image viewed on a desktop or a laptop allows the scroller on the image to move)
2-An orogastric or nasogastric tube should only use an elemental feeding formula. This is because the food in the stomach is prevented from mixing with the biliopancreatic juices, which will not be adequately absorbed.
3-A feeding Jejunostomy can only be insured surgical post ligament of traits. This cannot be done endoscopically because duodenal switch transaction post pyloric small bowel to prevent mixing of the biliopancreatic secretion.
Additional informationWhy Oxygenation in Covid-19 is a major problem
April 21, 2020 7:27 am
Covid-19 is a respiratory virus. The majority of patient may experience no or minimal symptoms. But small subset of those infected will unfortunately progress to have significant pulmonary dysfunction. Some will even require mechanical ventilation. Oxygenation in COVID 19 patients with severe symptoms is altered. This is the due to the changes caused by the virus.
Normal Physiology
Oxygen (O2) is exchanged with Carbon Dioxide(CO2) in the lungs. The CO2 is exhaled and the O2 is taken up by the blood. This high O2 continuing blood is then pumped to every single organ. With complete distribution network of capillary vessels, every cell then gets access to the O2 rich blood. Hemoglobin is the carrier that transports the O2.
The O2 is removed and dissociated from the Hgb depends on a number of variables. Each red cell Hgb has four binding site for the oxygen. The affinity and strength of each one of those four units for oxygen changes based on a number variables. These are CO2, Acidity (PH), DPG and temperature.
Oxygen Dissociation Curve
The oxygen dissociation curve has a long “S” shape. On the low end of oxygen in the blood most of the Hgb site are occupied. As the oxygent level increase there is little change to the saturation.

Normally the relationship of the blood in the lungs (horizontal axis) and the amount of the O2 in the red cell (vertical axis) is following the red line. When the amout of oxygen insired is 25mmhg the blood saturation is at 50% (A). The blood saturation is nearly 100% when room air is inhaled (C). Room air has PO2 of 75mmHg. Note that there is very little change in blood saturation (SaO2) by increasing the PO2 from 75 to 100 mmHg (the red line is horizontal between 75-100).
{kind=link}
Another way to look at this: If you increase the PO2 from 25 to 50 (doubling) the Saturation goes from 50 (A) to nearly 85(B). Whereas increaseing the PO2 from 50 to 100 (doubling) only mober the Saturation from 85(B) to 100(C). This shows the efficiancy of system to be able to deliver the most amout of oxygen to the tissue even with the low level of oxygen present in the lungs.
As the Green and the Blue lines demosntrate the balance can change by changes in CO2, Acidity (PH), DPG and temperature.
COVID-19
When it comes to COVID-19 illness there may be a number of factors in play. Most patients with pre-existing conditions already have changes that may shift the curve to the right (high fever and high Co2). Furthermore, obesity, asthma and other conditions may decrease the ability to clear the lungs of secretions and mucus may contribute to decreased oxygenation. Additionally, there is significant inflammation associated with the chemicals released in COVID-19 (cytokines). These can cause devastating changes to the ability to exchange oxygen in the lungs.
Oxygenation in COVID-19 severely symptomatic patient can deprive oxygen from organ. This can progress to organ failure. One of the most common organ systems to fail is the kidneys which may require dialysis.
Stapled Anastomosis
December 30, 2019 11:23 am
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
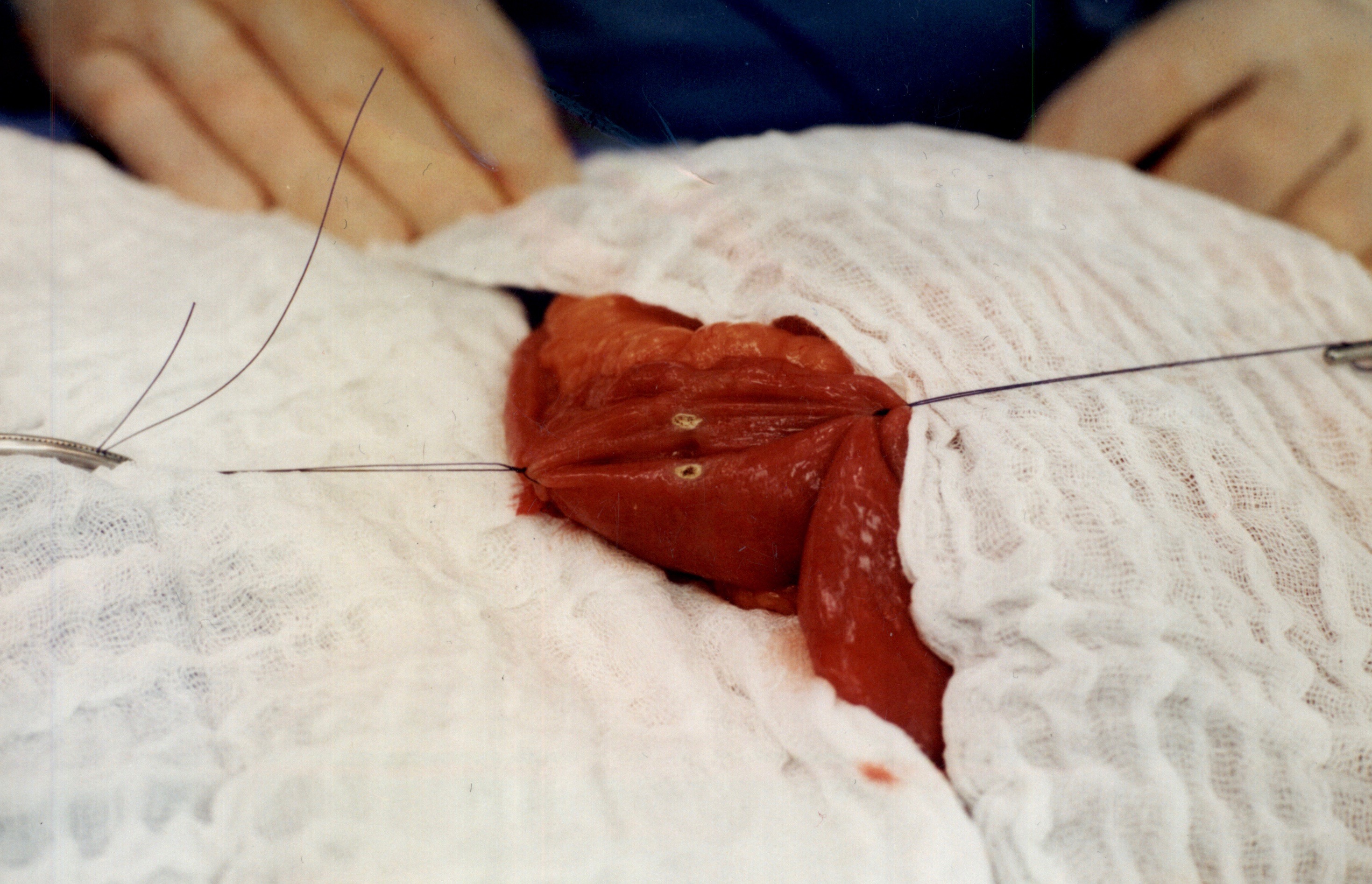
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
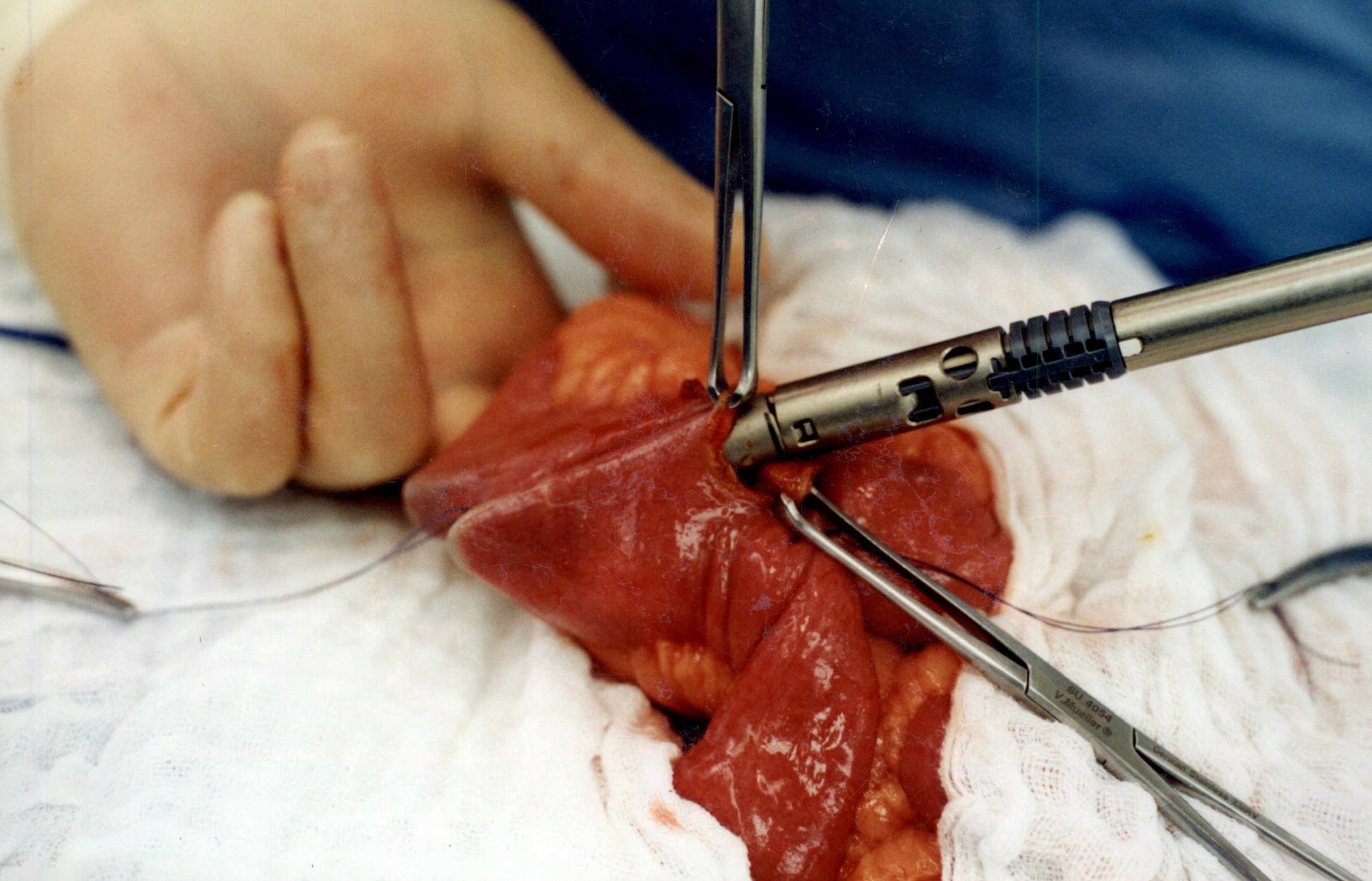
When the stapler is fired in opposite direction, a very wide anastomosis is created.
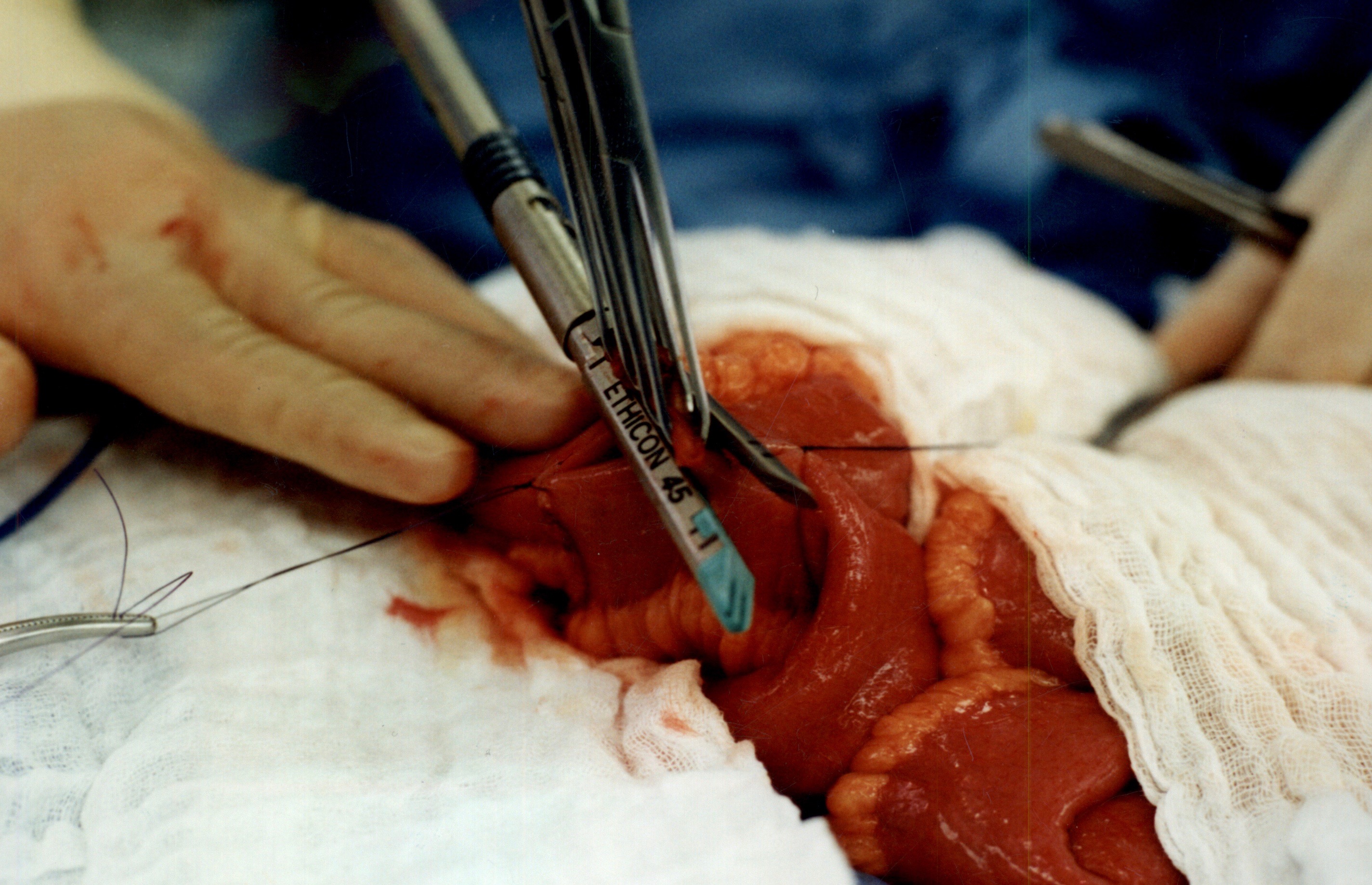
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Intestinal Peristalsis
June 24, 2016 6:32 pm
The following video is an example of intestinal peristalsis, the rthymic contraction and relaxation of the intestinal muscles to propel digested food through the intestinal tract. This process starts after food product is swallowed into the esophagus. It continues once the food is emptied through the pyloric valve into the small intestine. This motion allows for absorption of nutrients from the food product. Peristalsis continues throughout the small intestine and into the colon (large intestine) until defecation.
Click the following to view the Video of Intestinal Peristalsis
Peristalsis also happens within the tubes connecting the kidneys and bladder and also the tubes between the gallbladder and duodenum