Category: Weight loss surgery. duodenal switch
Sleeve Gastrectomy Failure
May 07, 2019 12:53 pm
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
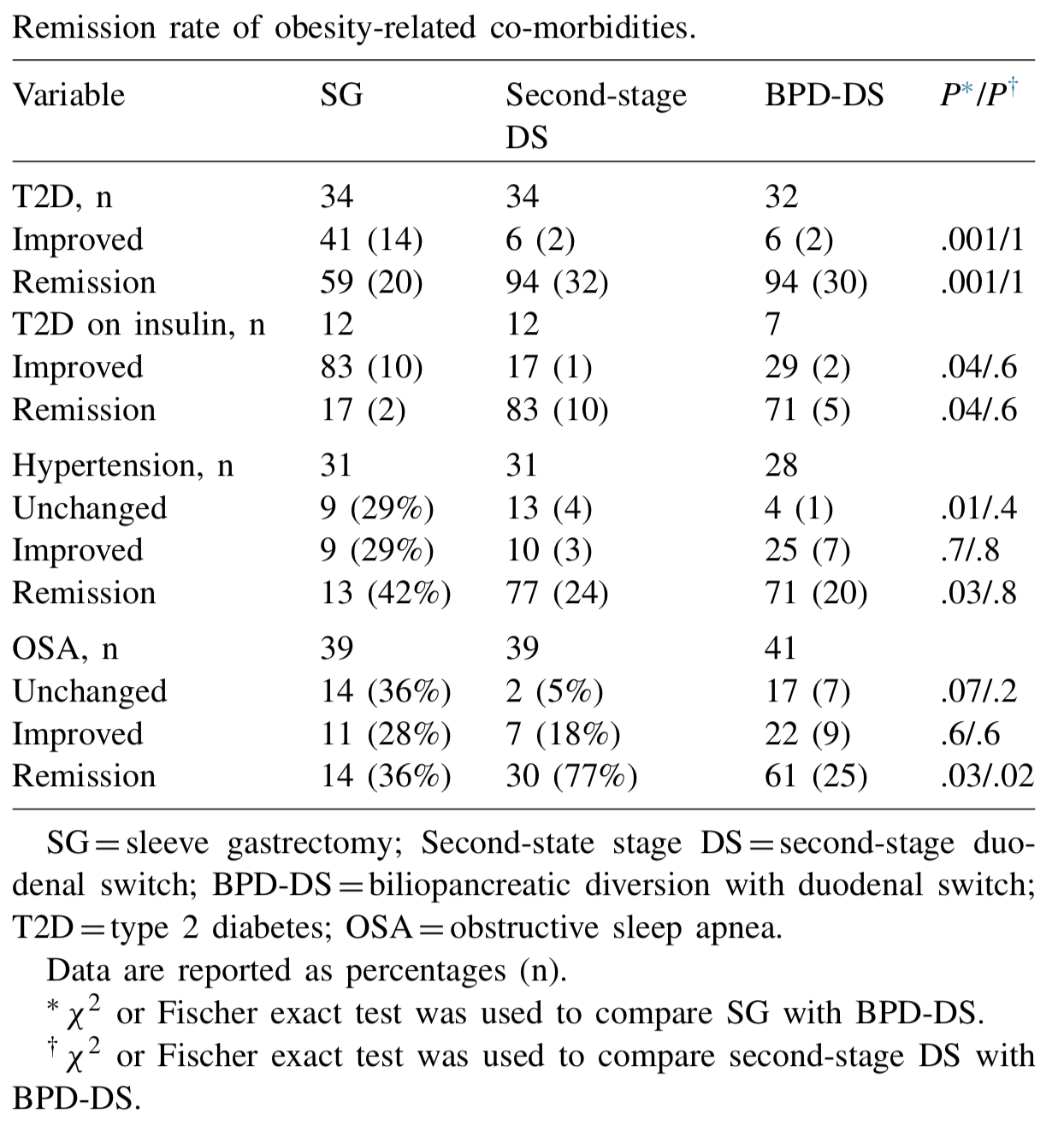
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss. 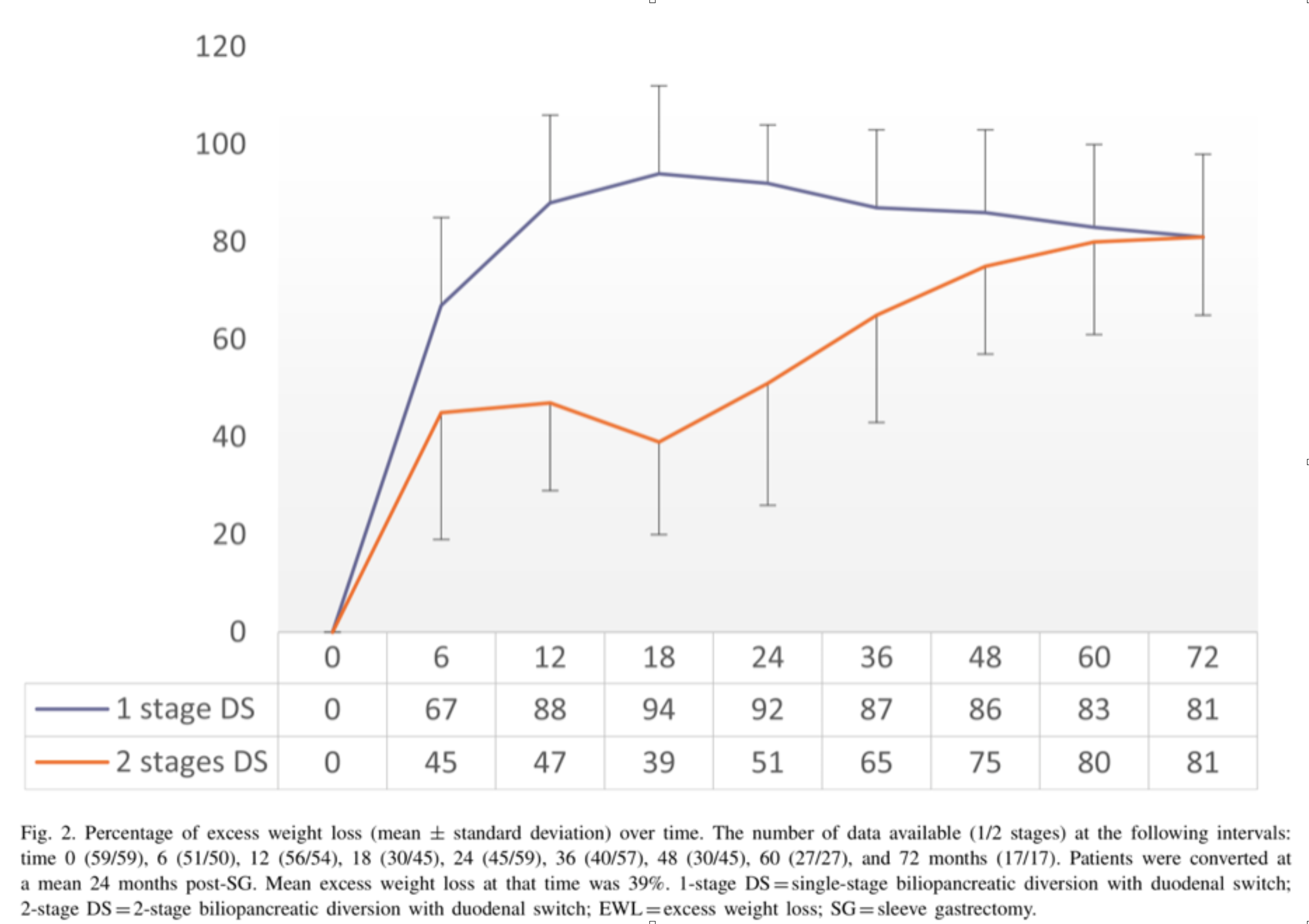
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.
Dr. Facebook
March 22, 2019 8:24 am
We have become reliant on the information that we obtain from the internet, specifically platforms such as Facebook. In our practice we have to continuously correct information that patients have obtained from other patients, unmonitored sites, blogs, and postings. Most of this information is based on individual experiences that has become gospel. “Fat is good for you” is one of them. To clarify, some health fat (olive oil, avocado, Omega 3) is healthy and needed for all patients. We do not recommend “fat bombs” as a part of ones daily dietary intake.
The following article was written on the accuracy of nutritional posts in support groups on Facebook.
Koalall et. all in SAORD, December 2018 Volume 14, Issue 12, Pages 1897–1902 published
“Content and accuracy of nutrition-related posts in bariatric surgery Facebook support groups”
The conclusion, as suspected, that “Over half of the posts contained inaccurate content or information that was too ambiguous to determine accuracy..:”

It is our recommendation before any dietary recommendations are taken from facebook and the like, the source of the information should be verified. As I have stated in the past, a frequent flier passenger is probably not qualified to fly a
commercial airplane, any more than a previous weight loss surgical patient providing medical and nutritional advice. We realize that there is significant value to the forum for exchange of information and sharing of experiences with other weight loss surgical patients as long as the information is well sourced and verified.

Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP
PolyCystic Ovarian Syndrome PCOS
September 04, 2018 9:58 am
PolyCystic Ovarian Syndrome PCOS is a complex condition. The exact cause of PCOS is unknown however, it involves hormones imbalance and multiple ovarian cysts, irregular menses, and infertility. In some cases, PCOS can be compounded by diabetes, hypertension and other metabolic conditions. PCOS has been shown to effect approximately 10% of women of childbearing age with symptoms of menstrual abnormalities, poly cystic ovaries, and excess androgen (male sex hormone). PCOS should be diagnosed by ensuring there are no other underlying endocrine issues. There are several associated disease processes that seem to be related to PCOS. These related disease processes are Type 2 Diabetes, higher depression and anxiety, increased cardiovascular risks, stroke, hyperlipidemia, sleep apnea, overall inflammation, and endometrial cancer.
Anatomically, numerous cysts are found on the ovaries. These are usually diagnosed by ultrasound, blood levels of hormones, and symptoms described above.

Bariatric Surgery and PolyCystic Ovarian Syndrome PCOS
Bariatric Surgery can improve PCOS in those individuals with Type 2 Diabetes Mellitus. Further information on weight loss surgery and its effect on PCOS here.
Health Insurances Working Against You
July 09, 2018 12:01 pm
Are Health Insurances working against you? Especially in people who have the disease of obesity? Insurance companies continue to lengthen the pre-operative period. The time that is required to lapse has now in some cases been extended between 6-12 months for some commercial health plans. There are yet again studies that have shown no benefit to the patient with this mandated waiting periods imposed on the patients. Unfortunately, the patients need to challenge the health care insurance companies by the means of all options that may be available to them. This may include internal appeal to external evaluation by some state agency. There are numerous studies that show pre-operative dieting does not equal better weight loss or compliance.


Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

Calcium Lab Results
June 05, 2018 3:26 pm
Calcium is measured to evaluate function and adequacy of a physiologic processes. Calcium plays a critical role in several body functions such as, coagulation pathways, bone health, nerve conduction, and other functions. It is important whenever you are evaluating laboratory results that you look at the whole picture of the person, including medications, other laboratory studies and health history. One value is not a stand alone result. There are many factors that effect calcium results.
Factors that effect calcium results: (not an all inclusive list)
pH
Albumin
Lactate
Heparin
Anticonvulsants
Renal Disease
Pancreatitis
The two most common issues following Weight loss Surgery or Duodenal Switch may be albumin level and Vitamin D level. Please see past blogs on Vitamin D. Magnesium may also play a role in a Duodenal Switch patient.
The most common calcium result drawn is the total calcium level. Laboratory results may not explicitly label it as such, however, it measures the calcium that is bound to protein. Ionized calcium is the free calcium that is representative of the true total calcium. Ionized Calcium can be measured by ordering specific lab. Alternatively, the Ionized calcium can be calculated by the following formula: Corrected calcium mg/dL = (0.8 * (Normal Albumin – Pt’s Albumin)) + Serum Ca ) or use the calculator at the bottom of this post.


The low Albumin level accounts for the low calcium level. This may be the reason for a patient with a low albumin/protein level, also having their calcium level reported as low. However, when adjusted for the protein deficiency the corrected calcium comes into normal range. Video of Trouseau’s sign of a patient with calcium deficiency.
The first step in a patient who has low calcium reported, is to make sure their protein and albumin levels are normal, along with Vitamin D.
Calcium levels are managed by two processes major regularly hormones and influencing hormones. Controlling or major regulatory hormones include PTH, calcitonin, and vitamin D. In the kidney, vitamin D and PTH stimulate the activity of the epithelial calcium channel and the calcium-binding protein (ie, calbindin) to increase calcium absorption. Influencing hormones include thyroid hormones, growth hormone, and adrenal and gonadal steroids.
Further information on protein.
Further information on calcium.
Videos/Webinars on several of the above topics.
Corrected calcium = 0.8 * (4.0 – serum albumin) + serum calcium
Shared Success Story- Theresa & Rodney (Duodenal Switch)
August 05, 2017 8:41 am
Life before surgery seems like a lifetime ago for both my wife and I. Being extremely overweight is not only a burden on your general health but a burden on your lifestyle in general. You have the awful label of being called obese, or morbidly obese. This is such a wonderful word that makes you feel as if you have been judged a misfit in society. We were both overweight all of our lives and had done all of the diets known on the planet throughout the years. Some worked a little some not at all and we always found ourselves back to where we were before and usually larger than that. The main focus though as we were getting older was our health. For Theresa it was very difficult. Along with being over 400 pounds she had a severe case of asthma which caused her episodes where she felt she was going to suffocate. She also had very little muscle mass which made it very difficult to get up and down from seating or lying positions. Theresa had her surgery in February of 2014 and not a moment too soon. If she had done nothing it is a good chance that she was facing a horribly short future. She also has a slight heart murmur which did not bode well for a person with her weight. She did not have diabetes thank goodness but her A1C was on the rise as was her BP. She did have sleep apnea as well and had to have a CPAP machine.
I was also severely overweight, my highest weight was nearly 400 pounds and on surgery day I was 355 pounds. I was also under the illusion that I had more control over my weight and that once Theresa had her surgery I would just be able to diet and exercise my way to a healthy weight. I was able to do this in my younger years to a certain extent and I was naive enough to think I could continue to do so. How wrong I was. I had found that no matter how much diet and exercise I did my weight would drop a bit at first but then stall and I would have to essentially starve to lose any more and of course that just makes for a bad outcome. My A1C shot up to 7.6 and this was with 1000mg of metformin a day! My BP was very high with both numbers over 100, well over. This is with a high dose of BP meds. I had a severe case of sleep apnea and could not even consider sleeping without a CPAP machine with a high pressure. I have an artificial hip that was being burdened by my 350 pound plus frame and would probably need to be replaced sooner rather than later. My future was not looking good. Dying before I was 60 seemed like a reality for me and that is not the future I was hoping for. The decision to have weight loss surgery for the both of us was tough. You of course hear the nay sayers spout what a cop out it is and it’s the easy way out! You are just weak and just simply need to not eat hamburgers, French fries and donuts. Just stick with non-fat and low calories and you will reach the promised land. What a load of BS.


Once you wrap your head around the fact that your body is wired in such a way that it will always seek a higher weight every time you lose weight, it’s time to consider the type of surgery. Everyone has heard of the Gastric bypass and that seemed to be the path at the time of Theresa’s surgery. The thing about Theresa and what I admire very much is her persistence and her ability to research to the point where a decision is spot on. She looked at all of the four possible surgeries and quickly realized that the Duodenal Switch was a no brainer. It had the greatest measure of success in the long term as well as short term. Reading about the process and talking to others who have had the surgery it became clear that it was the right choice. Finding out where to go and have the surgery was a real challenge. We were lucky to find Dr. Ara Keshishian and have the ability to travel to his location to have the surgery.
Theresa’s Stats Rodney’s Stats
Surgery Weight: 410 Surgery Weight: 355 Pounds
Total Weight Loss: 215 pounds Total Weight Loss: 170 Pounds
Surgery Type: Duodenal Switch Surgery Type: Duodenal Switch
Surgery Date: February 2014 Surgery Data: May 2016
Surgeon: Dr. Ara Keshishian Surgeon: Dr. Ara Keshishian
Life after surgery is an amazing series of challenges, changes, and a journey that transforms your life in a huge way. For Theresa, it was freedom. Freedom from the overbearing weight she was carrying that kept her from essentially moving or doing anything but staying at home. We did very little outside of the house before surgery. Only the necessities of shopping and keeping up the house on the inside and out. Even that was difficult and went by the wayside all too often. Of course eating out was easier than going to the grocery store and that made the scale just go higher. After surgery, Theresa began to lose weight and you could see day by day the changes. After the first month, you could see a dramatic change not only in her look but the fact that she was moving again! She had dropped 35 pounds in that first month and it made a huge difference. As the weight kept coming off over the next few months we began doing things we have not done before. We started to do a lot of walking and a lot more things around the house that needed to be done. Shopping became a breeze and we ate out a lot less. The dramatic change was in her health. A number of changes for the better were happening on that front. The main one and a huge relief was the asthma. It simply was no longer there. She was no longer short on breath and was simply out moving me! I could barely keep up with her. She also had a bad case of psoriasis which before surgery she could do nothing about. Since the surgery it has disappeared. It might be due to the increased in vitamins, particularly the D vitamin. Her sleep apnea went away and now she is healthy and happy. It is almost difficult to describe the changes until you see them for yourself. For Theresa it has been a life changing experience that has transformed the both of us in ways we never imagined. Theresa eats a normal diet and after 3 ½ years post op she fluctuates about 5 pounds either way. It is amazing.
For me it was not what I expected. What I mean by that is, learning to eat is a challenge. With the Duodenal Switch you are not only eating less, but what you eat is tremendously important to the success of the transformation. With the other surgeries, Lap Band, Bypass and Sleeve you do not have the degree of malabsorption. You simply eat less and you lose weight, but you are still essentially “on a diet”. With the Duodenal Switch you have to consider the malabsorption and think protein first and for most. Once you get past the first month of eating small amounts and what you can while your innards heal you need to learn what to eat and is it enough protein. You may also have to contending with the fact that you have an aversion to foods you ate before. I, for one, could not even eat cheese, and chicken. I pretty much lived on scallops, crab, shrimp and protein drinks for the first three months. Nuts were also a good source of the protein when you get to that stage. This does change and things do go back to normal as far as the taste changes, but it takes a few months. The weight in that first month pretty much peeled off. I was dropping like a pound a day. It was incredible. You think that this is going to be a breeze and you will drop it all in no time! Then that 4 week somewhat of a stall occurs. From what I can tell, everyone experiences it in one form or another. It freaks you out because you start to think about the past where you would work your butt off and either gain or drop and ounce or two. But I was lucky, my wife had gone though it two years before me so she was there to explain that it was normal. The whole “this is a journey thing”, and she was right! At the time though I was listening to the negative voice in my head from the past. That is where the support from the many groups come in. You see that pretty much everyone has the same ups and downs and then your body gives up the farm and you drop a bunch of weight in a weeks’ time. There is really a lot of science behind it. Researching and reading about this particular surgery and how it works will benefit you while you go through the process. Another important thing we face with this surgery is the necessity of Vitamins. Thank goodness for my wife and the DS groups and of course my surgeon. You will not be without knowledge if you actively join the different groups and do your research on the vitamins. I am still learning about what my body needs and am looking forward to my labs in the next month to see where I may be deficient. I have also come to realize the importance of drinking water and avoiding dehydration. I never used to drink it much before the Duodenal Switch, but since the surgery I find it aids heavily in the success if you drink it and drink a lot of it.
To conclude this has been a journey and one I wish I could have done a lot sooner in life, but it is never too late. Today Theresa and I are at weights that we are happy with and our bodies are happy with. We are more active then we have ever been before together. No more days idle in front of the television with large amounts of fast food and drinks. That is what we used to look forward too. Now we cannot wait until we go out and do something. We are not running marathons or anything but we are active and enjoy being so. We no longer have the ailments we had before surgery. Theresa’s asthma is practically nonexistent, living in the northwest with fires in the summer she may have a bout or two. Nothing even close to what she has before and a simple inhale and its gone. Both of us no longer need a CPAP! The freedom to simply lay your head on the pillow and sleep is amazing and wonderful. All of the medication we had prescribed for us are gone as well. My A1C was 5 on my last set of labs and 5.3 on the one before that. Theresa’s is the same and has been for three years. BP is normal and my hip is holding steady. Oh, and another cool thing about it is you can actually shop for clothes anywhere! Your sizes will shrink but we have found we have become quite the clothes horses since losing all this weight. It makes it fun to be able to fit into a size you haven’t seen since who knows when.
Life is always a challenge for many reasons but to remove the burden of the weight simplifies things just a bit. It is a decision we will never regret and wished we had made a long time ago. We both owe our lives firstly, to having Duodenal Switch surgery. Secondly, and most important – was in seeking out the best surgeon we could find, and that was without a doubt, Dr. Ara Keshishian. As a surgeon he is thorough, meticulous, constantly learning and keeping up on the latest research;as a person he is easy to talk to, very approachable, and genuinely cares about his patients before, during and after the surgery process. We could not imagine choosing anyone else.
First Duodenal Switch Patient- Dr. Hess
April 05, 2015 3:35 pm
I had the opportunity to be in a meeting with Dr. Hess in November of 2004. He presented a lecture about the history of the Duodenal Switch and his collaborative work with Dr. Scopinaro, the pioneer surgeon of the Biliopancreatic Diversion. The BPD was the the foundation of the Duodenal Switch operation. The first patient ever to have had the Duodenal Switch was a revision from a failed vertical banded March of 1988 by Dr. Douglas Hess. At the time of this particular meeting (in 2004), the patient was 17.5 years post op.

This is a copy of the slide that he shared with the surgeons present at the Duodenal Switch meeting on November 21, 2004.
Sunshine, Water, Rest, Air, Exercise and Diet
May 23, 2014 4:10 pm

{kind=link}
Sunshine, Water, Rest, Air, Exercise and Diet
Of course this is over simplified, but we can’t forget the importance of the basics in our general well being. Weight loss surgery and especially Duodenal Switch have distinctive supplement requirements that need to be individualized based on your individual needs.
Sunshine is essential to life. It provides the light that wakes us and helps to regulate wake/sleep cycles and provides us with a feeling of well being. Sunlight is not only the basis of all living things but crucial in boosting the bodies Vitamin D supply. Most Vitamin D deficiencies in the general public are caused by lack of sun exposure. It is important to note that our bodies can not accomplish Vitamin D metabolism if we are wearing sunscreen. Without adequate Vitamin D stores bones will not form properly, muscle strength is impaired and osteoporosis. Vitamin D 1,25(OH) accumulates in cell nuclei of the intestine, where it enhances calcium and phosphorus absorption, controlling the flow of calcium into and out of bones to regulate bone-calcium metabolism. However, after weight loss surgery this mechanism can be impaired. Addition supplementation of Vitamin D is usually required based on laboratory studies following weight loss surgery. Duodenal Switch patients should take a dry “water miscible” type of Vitamin D3 daily.
Water comprises 50-60% of our adult bodies. Water is essential in cell life. It aids in transporting vitamins, nutrients and minerals to our cells. Chemical and Metabolic reactions rely on water to remove waste products including toxins that the organs’ cells reject and removes them through urine and feces. Our body temperature is regulated by sweating and the evaporation of water on the skin. Also, effectively Lubricating our joints and acting as a shock absorber for our brain, eyes, and spinal cord. Decreased stomach size, after weight loss surgery, limits the amount of water a person can drink at one time. It is imperative that patients ingest enough waters and fluids after surgery. We like to see our patients consume a minimum of 64 ounces of fluids a day, more on warmer days.
Rest is something we can all use more of. Lack of sleep can cause a whole host of health issues ranging from altered levels of hormones involved in metabolism, appetite regulation, stress response to cardiovascular health, insulin resistance, immune function and most importantly post-operatively tissue repair, muscle growth and protein synthesis. It’s easy to take rest for granted but do not underestimate the power of sleep.
Air is an obvious essential of life. It is important in about every function of our cells. After surgery it is important to lung health and tissue repair. Be aware of the type of air you are breathing. Pollution and contaminants in the air can impair lung function. After surgery your breathing and breathing exercises will prevent complications such as pneumonia and atelectasis. Long term air contaminants can cause asthma and long term lung health. In addition, post surgical patients will need to use their incentive spirometers to combat lung complications.
Exercise’s health benefits can not be denied. Exercise combat health conditions and disease such as stroke, metabolic syndrome, diabetes and cardiovascular disease. It also improves emotional outlook and mood. Physical activity stimulates the brain to release chemicals that involve increasing memory function. Exercise helps maintain healthy weight, improves energy, promotes better sleep, lowers stress and anxiety. Needless, to say after surgery exercise is extremely important for all the above reasons but also to ward off complications such as pulmonary embolism and deep vein thrombosis.
Diet is last but definitely not least. Balance along with moderation and eating whole unprocessed foods are best ways to ensure your health. We derive most our building blocks for cell growth from the nutrients we consume. The quality of the food we put into our bodies is important in lowering health risks such as cardiovascular disease, cancer, and weight control. Protein is crucial in muscle growth, hemoglobin, cell structure and enzymes formation. It is extremely important after weight loss surgery to remain diligent about protein intake throughout your lifetime.
It is interesting to see how all these elements are so intertwined in their synergy to maintain health. Most are easily found or done in nature. When engaging in one of these elements, many of the others are needed or benefited by the doing the first. Exercise requires that you stay hydrated, deep breath, possibly out in the sunlight and therefore you will rest better. Always follow your surgeon’s orders and recommendations based on your individual health status and laboratory studies.