Tag: BPD/DS
Medication Absorption After Weight Loss Surgery
March 30, 2020 8:01 am
Weight loss surgical procedures, in one form or another, achieve the desired effect of weight loss by altering absorption of fat, protein, and carbohydrates. This results in decreased total absorption of required calories.
An unintended consequence is the altered absorption of medications. Frequently I am asked about the specific medication. Usually the answer is vague since the information is limited on specific medications. If the desired effect is not achieved, then it is probably not being absorbed well. Specially, if the same dose of the same medication working well before surgery.
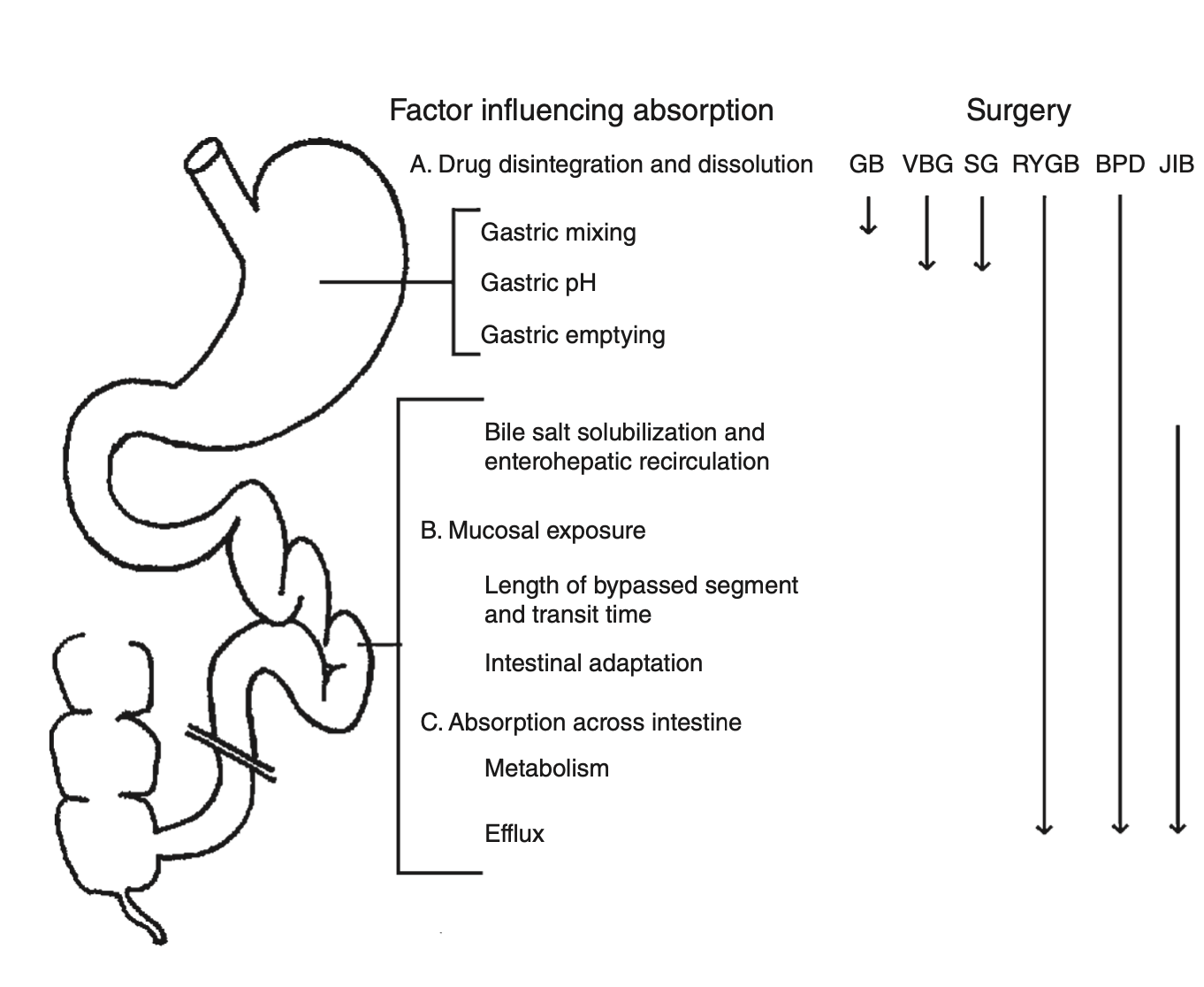
There is a summary article about the Theoretical absorption pattern of different weight loss surgical procedures.
Vitamin D Metabolism and Deficiency file
March 28, 2020 8:17 am
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
In some cases, patients may need injectable Vitamin A or D to improve vitamin levels.
Click the links to view the information below and within the comments of this file:
Vitamin D3 50 by Biotech: Amazon
directly from BioTech:
Many DS surgeon’s do not recommend Children’s vitamins or chewable vitamins unless there is a specific reason or need for them.
DS Surgeon Blog on Vitamin D:
Webinar on Vitamin D metabolism:
Medications that effect Bone health:
This does not constitute medical advice, diagnosis or prescribing. It is simply a compiled list of gathered information. If you are in doubt or have questions please contact your medical healthcare professional.
Articles
March 22, 2020 6:57 pm
Length of Bowel : Hess or No Hess
March 22, 2020 5:58 pm
“…What is the length of my common channel” is probably one of the frequently asked questions about the duodenal switch operation in the office. This usually comes up at the initial consult when patients repost credible sources such as Dr. Google and Dr. Facebook for patient with different bowel length have done well or not so after duodenal switch operation. Dr. Hess described the Duodenal Switch by using total bowel length measurements and creating the common channel as a percentage of the total small bowel length. However, it seems that this is being done less and less.
This leads to my explanation that is on the website
Hess calculator : Bowel Length Calculator
How the actual measurements matters: Bowel length video link
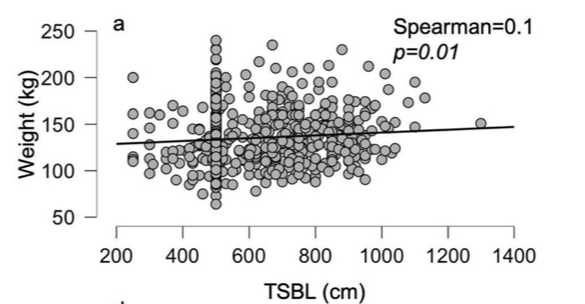
In 2019, Bekheit et.al published a very interesting study comparing total small bowel length (TSBL) to a number of variables such as height, weight, sex and BMI. They identified a few loose correlations. Male patient have longer TBSL than females. There was correlation between TSBL and height stronger in males than females but not statistically significant.
In Conclusion they reported ” Despite statistical significance of the correlation between the TSBL and the height and weight of the included participants, the correlation seems to have no clinical meaning since the effect size is negligible. ”
As I have previously discussed this Making the common and alimentary length standard for every duodenal switch patient will make some loose too much and other not enough weight.
Figure 1 shows TSBL on the horizontal axis, and height, weight, BMI and Age on the vertical axis. For the most part what they all show is that one can not predict how long a patients bowel is by any of the measures that we take in the office as a part of the routine exam.
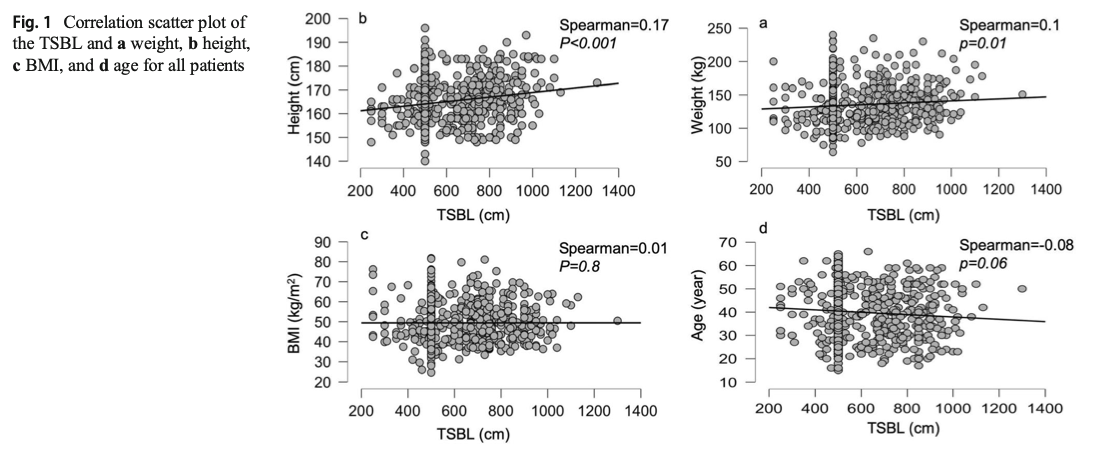
This raises, the concerns that I had raised previously. How could two similar patients who have the same weight, age, sex and BMI have the same surgery and expect the same result if one of them has TSBL of 400 cm and the other one 800cm?
Stapled Anastomosis
December 30, 2019 11:23 am
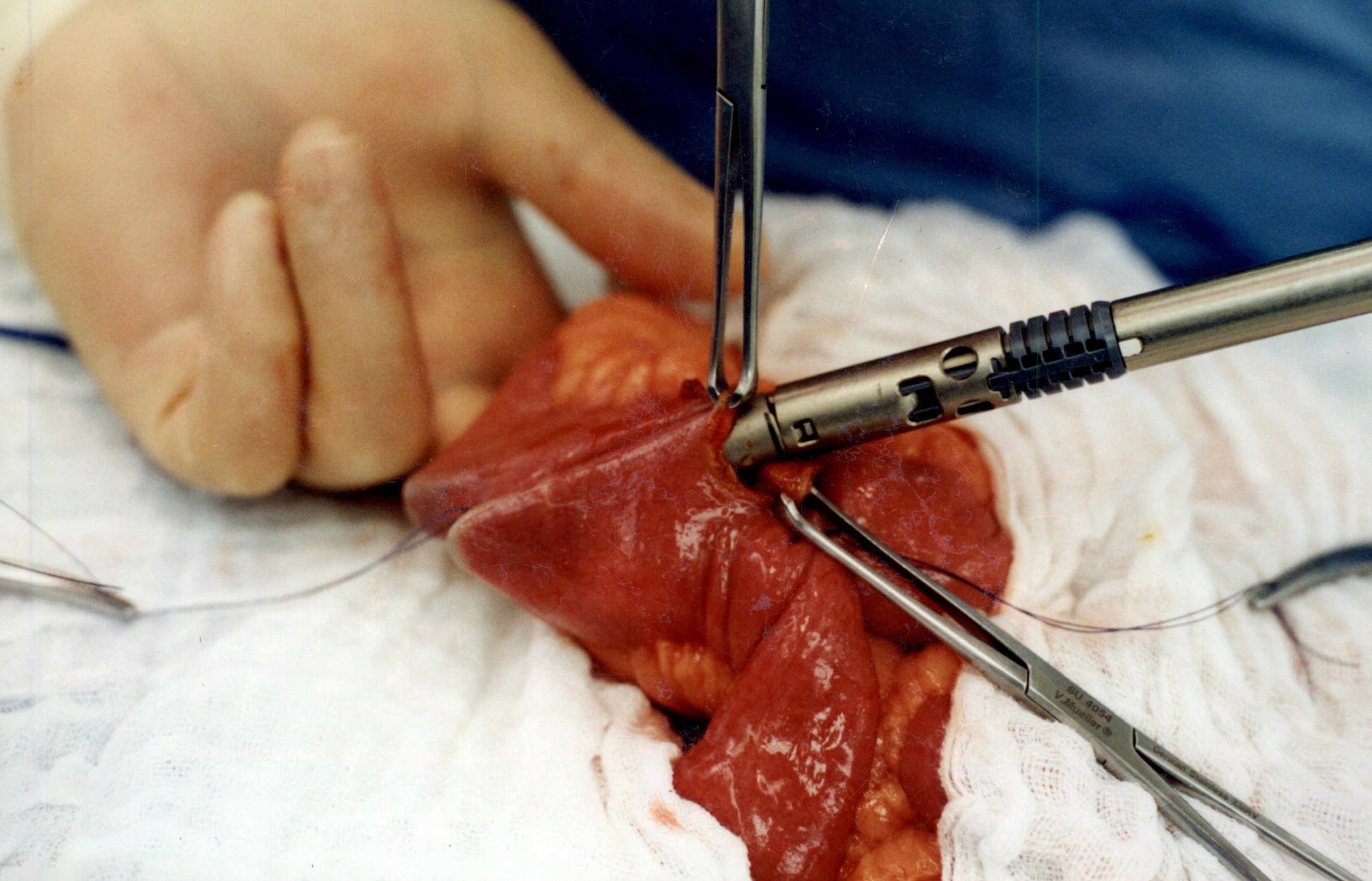
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
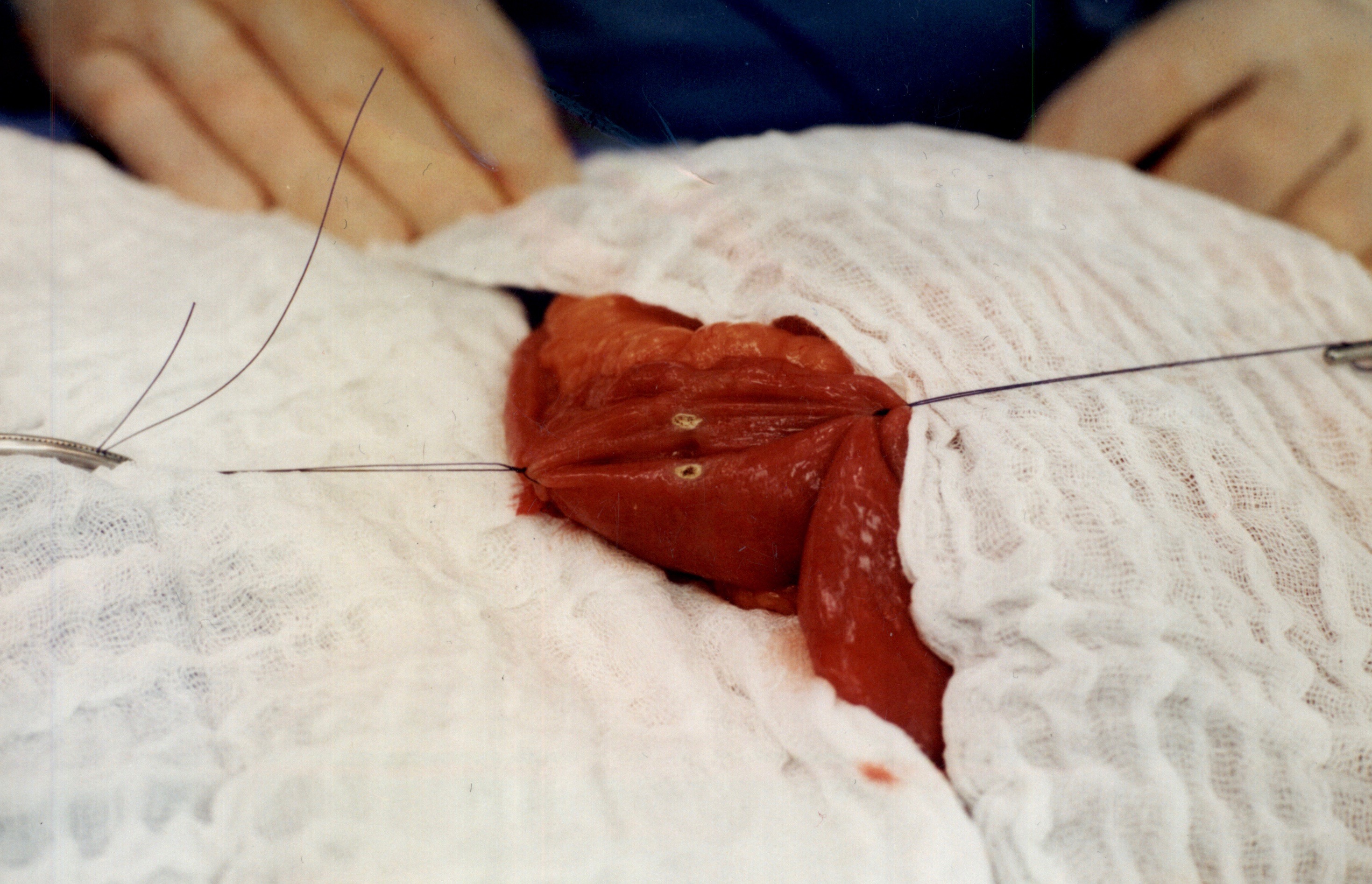
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
When the stapler is fired in opposite direction, a very wide anastomosis is created.
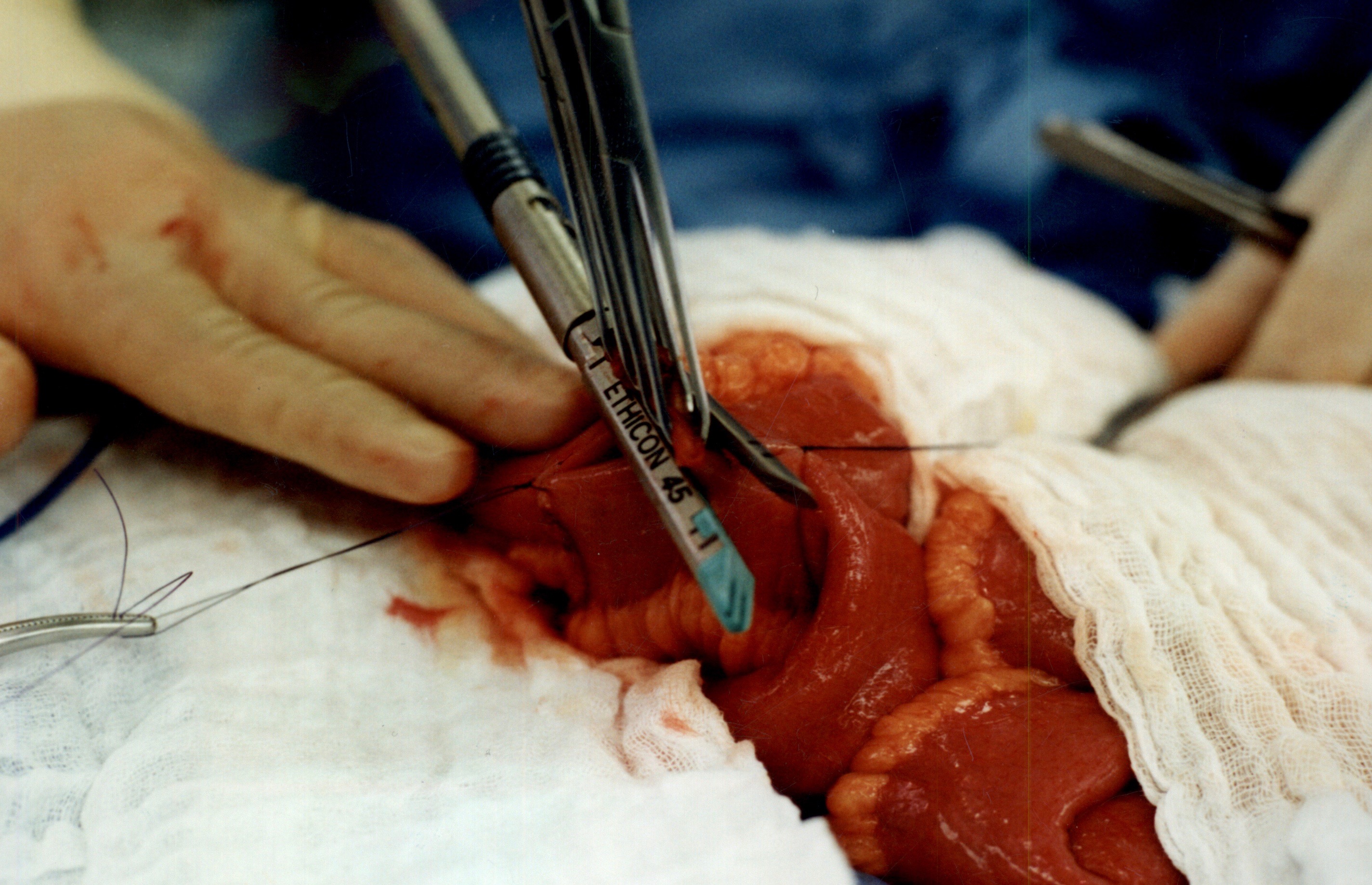
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Copper Deficiency Intravenous SupplementationExclusive Member Content
November 17, 2019 9:23 pm
Protein Intake
October 14, 2019 7:08 am
Protein intake requirements change over time following weight loss surgery. This is based on the requirements imposed on our body by a number of variables. These include, activity level, muscle mass, over all health condition to name a few.
A very young muscular athletic male with a BMI or 30 will require much higher protein intake (and absorption) that an inactive older Female with the same BMI. The same young athletic male will require much higher protein intake is he is recovering from a surgery than his baseline.
As we have stated in the past, the protein intake, should be adequate and not excessive. High level of protein intake that are not accounted for based on muscle mass and activity level, will eventually result in weight gain. The best measure of protein intake in a stable weight patient over 3-4 years post op is their albumin and protein level. Following your yearly laboratory values at a minimum is an important part of weight loss surgery follow up care.
You also need to adjust protein intake when necessary. Protein needs increase depending on physical needs, infection, healing, pregnancy, surgery, age, injury, etc. Plastic surgery requires higher protein needs for appropriate healing.
Information on protein sources and quality here.
The basic formula for protein intake is 1gm/kg of ideal body weight. The calculator below will provide a guide for the protein into based on your stable weight in lbs.
Vitamin A, Absorption, and Wound Healing
September 25, 2019 8:39 am
Vitamin A is one of the 4 fat soluble vitamins along with vitamin D, Vitamin E and Vitamin K. It is multifunctional and essential which means that it is not produced by the body. In this article we will touch on aspects of Vitamin A absorption and it’s effect on wound healing as well as its metabolism.
We often think of Vitamin A as the critical vitamin for vision, however it has several other roles that related to immune function, protein synthesis, and cellular communication. Vitamin A deficiency is a concern world wide because of the natural of the side effects. Vitamin A deficiency is the leading cause of preventable childhood blindness in the world according to UNICEF and sometimes it may be undetected until there is irreversible damage.
There are 2 chemical forms of vitamin A in diet:
Retinoids (Preformed vitamin A) This group include retinol, retinyl esters, and retinal they are mostly found in animal sources like liver, egg yolk or fish oils.
Carotenoids (Provitamin A) This group includes beta-carotene, alpha-carotene and lycopene, mainly found in plant sources like leafy vegetables or yellow/orange vegetables and fruits.
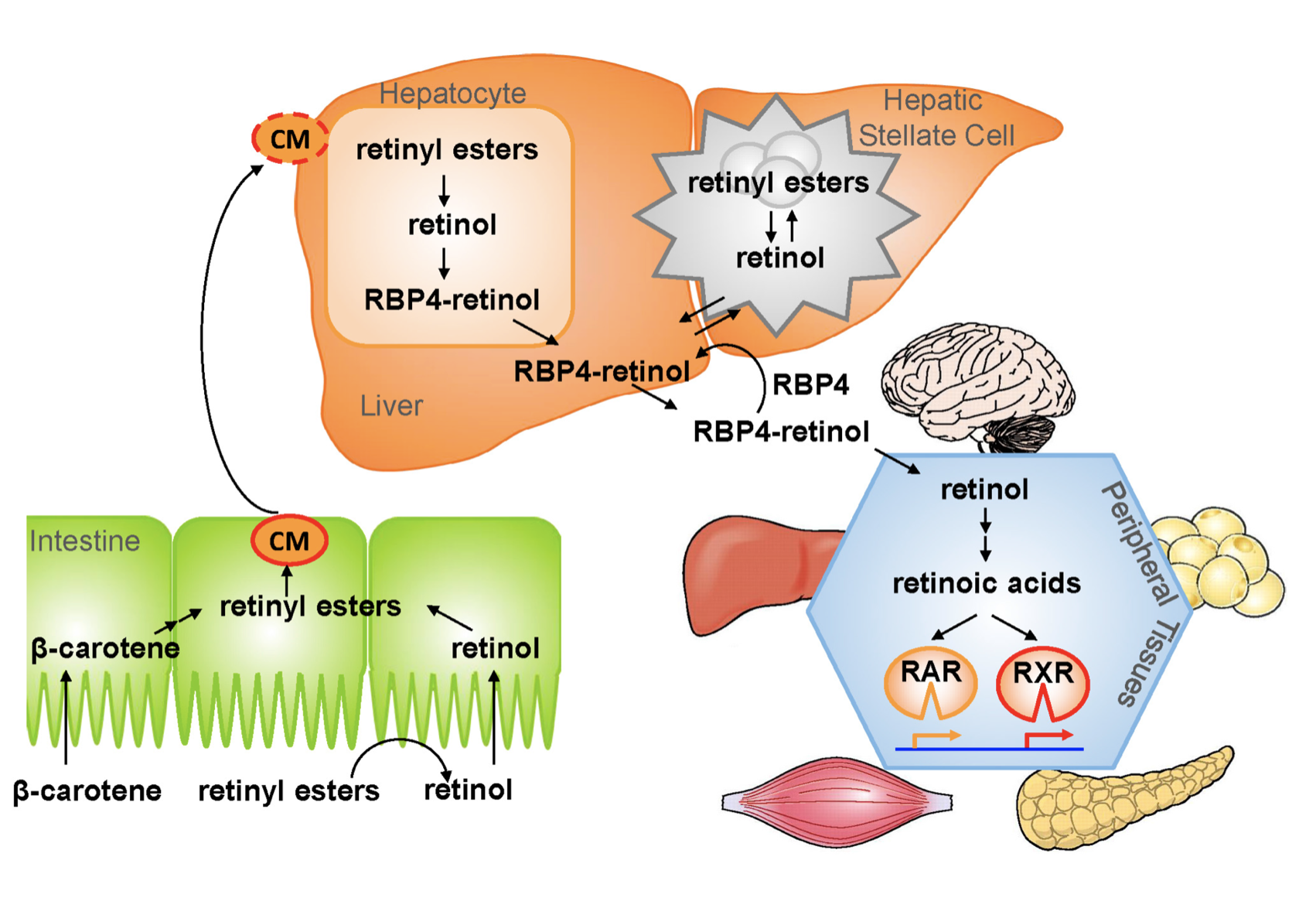
The Physiology of the Vitamin A is as follows:
1.- Ingested food is digested in the stomach where retinyl palmitates (esters) are released from proteins. Retinol and beta-carotene are absorbed directly into the small intestine where retinyl esters and betacarotene are transformed into retinol . Retinol is the most easily absorbed form of vitamin A.
2.-That retinol absorbed by the enterocytes in the ileum (small intestine) along with bile is then transported to the liver with the help of chylomicrons a protein that transports fat.
3.-Fifty to 80% of the vitamin A is stored in the liver and the remaining is deposited into adipose tissue, lungs and kidneys.
4.-When stored retinol is released from the liver into the circulation to target organs, it is bound to plasma retinol-binding protein (RBP4) a transporting protein produced by the liver that requires ZINC, which is synthesized by the liver; This complex is stabilized by transthyretin (TTR), which reduces renal excretion.
Retinol is a crucial component for reproduction, embryological development, cellular differentiation, growth, protein synthesis, and immunity in the form of retinoic acid and vision in the form of retinal.
One of Vitamin A additional roles is in epithelial health of skin and mucous membranes. It increases epithelial turnover which is crucial during would healing. It also has anti-oxidative effects which prevent cell damage and can prevent or reverse the effects of other damaging agents. In addition to these benefits it has also been associated with increasing collagen, fibronectin, keratinocytes and fibroblast, all important in wound tissue structure. There have been some studies that suggest giving higher doses of Vitamin A in patients with non or slow healing wounds.
It is important to remember that we have documents delayed diagnosis of adult vitamin A deficiency leading to significant night blindness in adults. It is critical that the patients and their primary care physicians are acutely aware of this possibility. In majority of the patients with low vitamin A, post weight loss surgery, aggressive supplementations, including injections need to be considered as a part of the treatment regimen.
We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
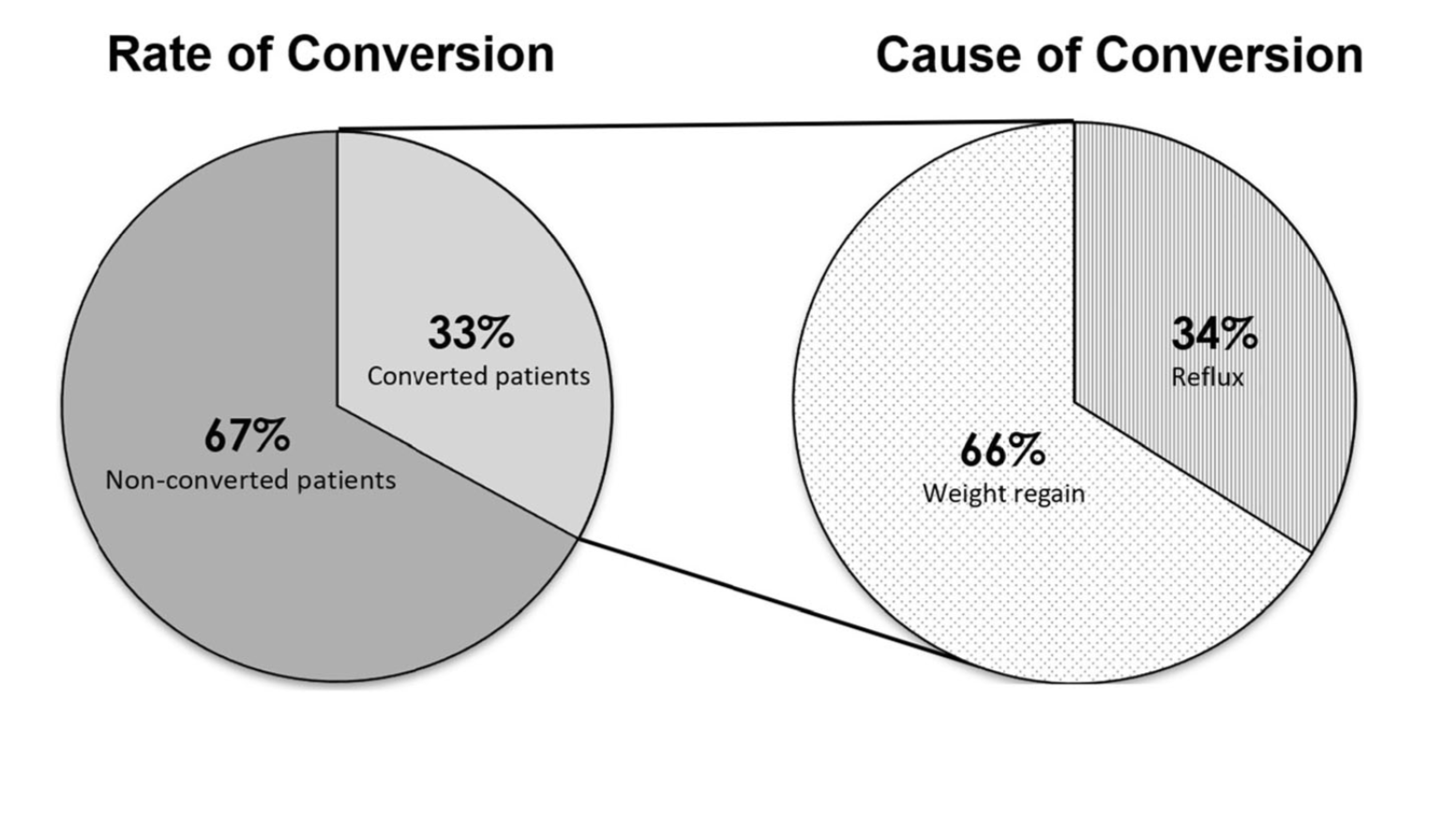
Sleeve And Weight Regain
July 22, 2019 9:50 am
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here