Category: Uncategorized
Protein Intake
October 14, 2019 7:08 am
Protein intake requirements change over time following weight loss surgery. This is based on the requirements imposed on our body by a number of variables. These include, activity level, muscle mass, over all health condition to name a few.
A very young muscular athletic male with a BMI or 30 will require much higher protein intake (and absorption) that an inactive older Female with the same BMI. The same young athletic male will require much higher protein intake is he is recovering from a surgery than his baseline.
As we have stated in the past, the protein intake, should be adequate and not excessive. High level of protein intake that are not accounted for based on muscle mass and activity level, will eventually result in weight gain. The best measure of protein intake in a stable weight patient over 3-4 years post op is their albumin and protein level. Following your yearly laboratory values at a minimum is an important part of weight loss surgery follow up care.
You also need to adjust protein intake when necessary. Protein needs increase depending on physical needs, infection, healing, pregnancy, surgery, age, injury, etc. Plastic surgery requires higher protein needs for appropriate healing.
Information on protein sources and quality here.
The basic formula for protein intake is 1gm/kg of ideal body weight. The calculator below will provide a guide for the protein into based on your stable weight in lbs.
Overfed But Undernourished
October 01, 2019 11:27 am
Obesity is related to as many as 400,000 deaths each year in the US and it has increasingly been recognized as a risk factor for several nutrient deficiencies. This may seem surprising given the likelihood of over consumption of calories, however these additional calories are not from nutritious sources. One of the main reason for these nutritional deficits is the greater availability of inexpensive foods that are rich in calories and are nutrient deficient. This has led some medical professional to conclude that there is a certain group of people who are overfed but undernourished. Even with the epidemic of the obesity, there is significant nutritional deficiencies noted.
Obese subjects have increased blood volume, cardiac output, adiposity, lean mass and organ size all of which can influence volume of distribution, in addition, treatment for severe obesity involving surgical procedures can worsen these nutrient deficiencies and in some cases may cause new ones to develop.
This table shows the percentage of population below the estimated average requirement (EAR) by body weight status in adults more tan 19 years old, showing that almost 90 to 100 percent of people including normal weight (NW) are below the EAR of vitamin D and Vitamin E.

We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
Flagyl
September 25, 2019 9:07 am
Flagyl is sometimes prescribed for excessive gas and diarrhea. It is an antibiotics that works well on certain bacteria that accumulates in the GI tract and contributes to the gas and the bloating.
These bad bacteria flourish when patients consume significant and excessive fiber and carbohydrates (sugars, salad, pasta etc.) The FIRST line of defense against flatulence, bloating, and diarrhea should be eleminating the culprits in the diet. This point can not be stressed enough. Adding a daily dose of yogurt may improve symptoms due to yogurts probiotic benefits. To be beneficial, Yogurt should contain live bacteria cultures, not contain artificial sweeteners or have a high sugar content.
Artificial sweetness also area source of the excessive gas and should be avoided.
The Flagyl eliminates and reduces the bad bacteria. Along with a Probiotic and healthy dietary choices Flagyl can help to significantly improved or eliminate those symptoms of gas and diarrhea.
Before Flagyl is prescribed, it is important that the diet is critically examined to make sure that the carbohydrates and the fiber as source of gas and bloating is minimized or eliminated. Excessive use of medications that may be needed for other infections should be avoided.
Chronic diarrhea should be evaluated to rule out GI infection with C. diff bacteria or other bacteria or parasite.
Additional Information on C. Diff (Clostridium Difficile) and probiotics.
Vitamin A, Absorption, and Wound Healing
September 25, 2019 8:39 am
Vitamin A is one of the 4 fat soluble vitamins along with vitamin D, Vitamin E and Vitamin K. It is multifunctional and essential which means that it is not produced by the body. In this article we will touch on aspects of Vitamin A absorption and it’s effect on wound healing as well as its metabolism.
We often think of Vitamin A as the critical vitamin for vision, however it has several other roles that related to immune function, protein synthesis, and cellular communication. Vitamin A deficiency is a concern world wide because of the natural of the side effects. Vitamin A deficiency is the leading cause of preventable childhood blindness in the world according to UNICEF and sometimes it may be undetected until there is irreversible damage.
There are 2 chemical forms of vitamin A in diet:
Retinoids (Preformed vitamin A) This group include retinol, retinyl esters, and retinal they are mostly found in animal sources like liver, egg yolk or fish oils.
Carotenoids (Provitamin A) This group includes beta-carotene, alpha-carotene and lycopene, mainly found in plant sources like leafy vegetables or yellow/orange vegetables and fruits.
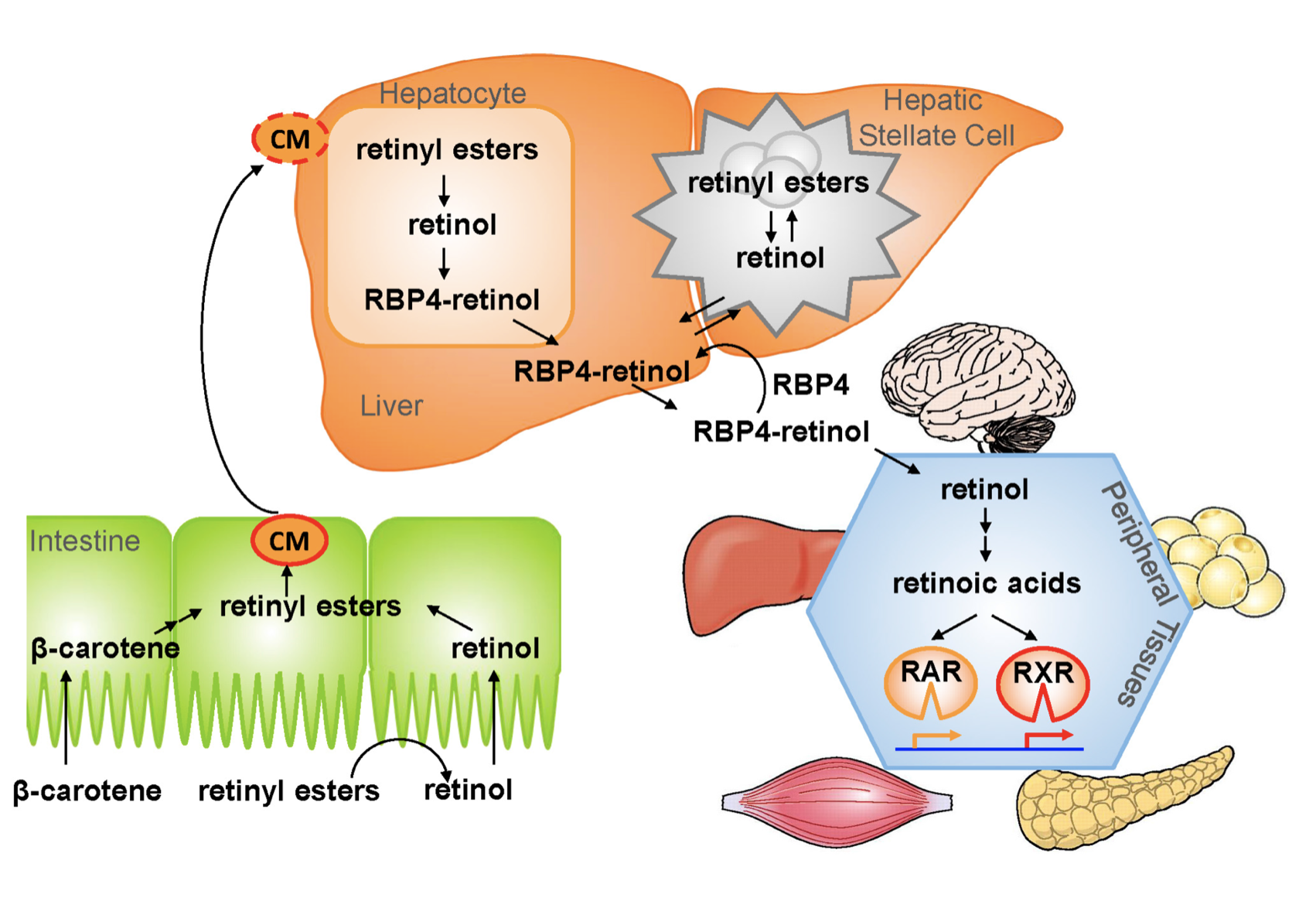
The Physiology of the Vitamin A is as follows:
1.- Ingested food is digested in the stomach where retinyl palmitates (esters) are released from proteins. Retinol and beta-carotene are absorbed directly into the small intestine where retinyl esters and betacarotene are transformed into retinol . Retinol is the most easily absorbed form of vitamin A.
2.-That retinol absorbed by the enterocytes in the ileum (small intestine) along with bile is then transported to the liver with the help of chylomicrons a protein that transports fat.
3.-Fifty to 80% of the vitamin A is stored in the liver and the remaining is deposited into adipose tissue, lungs and kidneys.
4.-When stored retinol is released from the liver into the circulation to target organs, it is bound to plasma retinol-binding protein (RBP4) a transporting protein produced by the liver that requires ZINC, which is synthesized by the liver; This complex is stabilized by transthyretin (TTR), which reduces renal excretion.
Retinol is a crucial component for reproduction, embryological development, cellular differentiation, growth, protein synthesis, and immunity in the form of retinoic acid and vision in the form of retinal.
One of Vitamin A additional roles is in epithelial health of skin and mucous membranes. It increases epithelial turnover which is crucial during would healing. It also has anti-oxidative effects which prevent cell damage and can prevent or reverse the effects of other damaging agents. In addition to these benefits it has also been associated with increasing collagen, fibronectin, keratinocytes and fibroblast, all important in wound tissue structure. There have been some studies that suggest giving higher doses of Vitamin A in patients with non or slow healing wounds.
It is important to remember that we have documents delayed diagnosis of adult vitamin A deficiency leading to significant night blindness in adults. It is critical that the patients and their primary care physicians are acutely aware of this possibility. In majority of the patients with low vitamin A, post weight loss surgery, aggressive supplementations, including injections need to be considered as a part of the treatment regimen.
We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
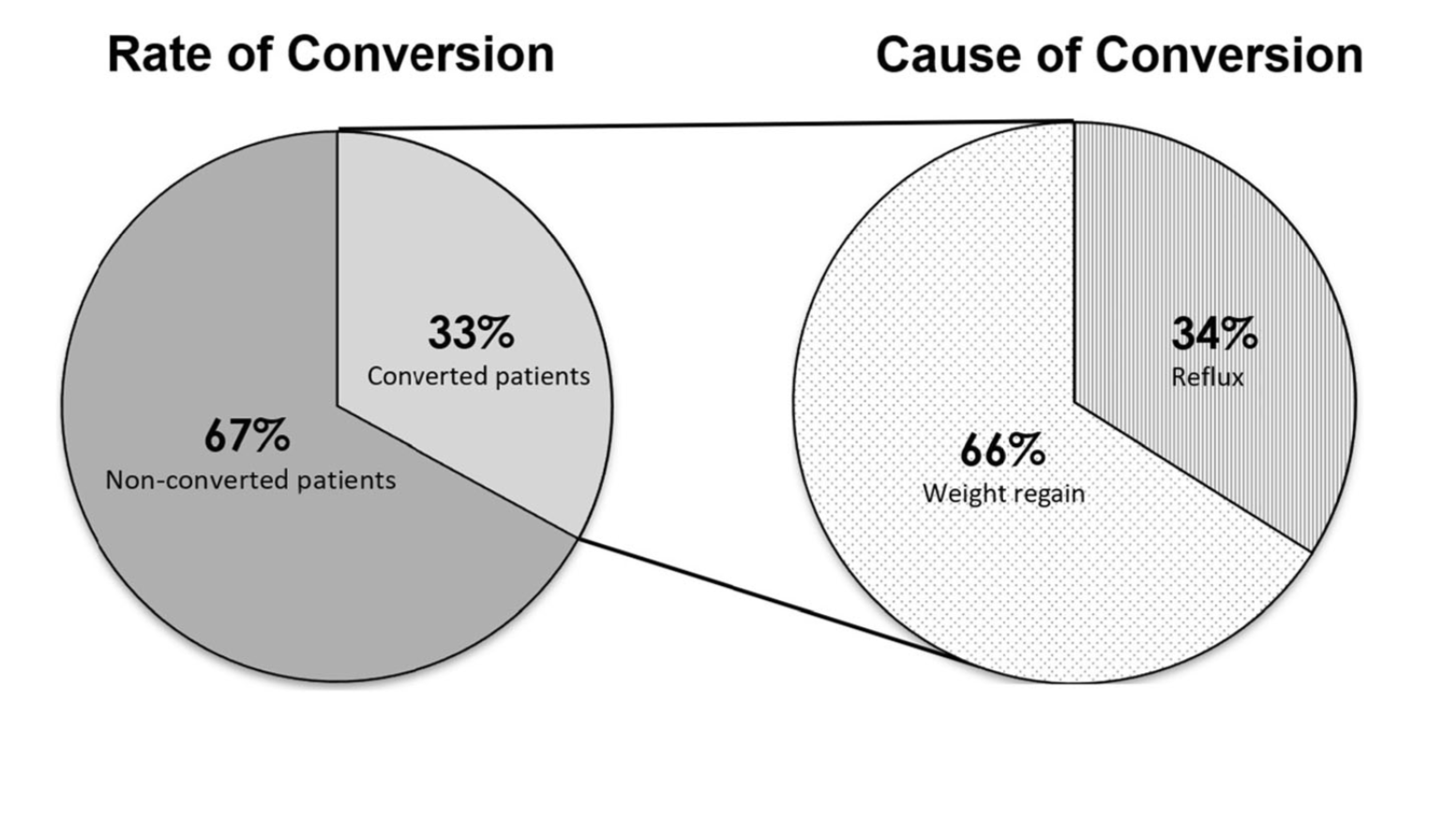
Sleeve And Weight Regain
July 22, 2019 9:50 am
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here
Thyroid Medication Absorption And Weight Loss Surgery
June 10, 2019 8:59 am
Question : “Do I have to take higher dose of thyroid medication after the duodenal switch? ”
Answer : “Maybe”
With all weight loss surgical procedures, there may be changes to absorption of medications. It is easily understood why duodenal switch may results in decreased absorption of fat-soluble medication. What is not as clear is the reduction in absorption of other medication with procedures that do not explicitly change the absorption at the level of the small bowel directly.
The research data is all over on this topic. There is published literature that shows improvement in the thyroid function after gastric bypass and the sleeve gastrectomy. However, the exact mechanism is not completely understood.
There is research that reports “…decreased postoperative levothyroxine requirements.” Other have shows no correlation between the length of the bowel distal to duodenum to absorption of thyroid medication.
With all this confusing data, the best course would be to always “treat the patient and not the lab results.”
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
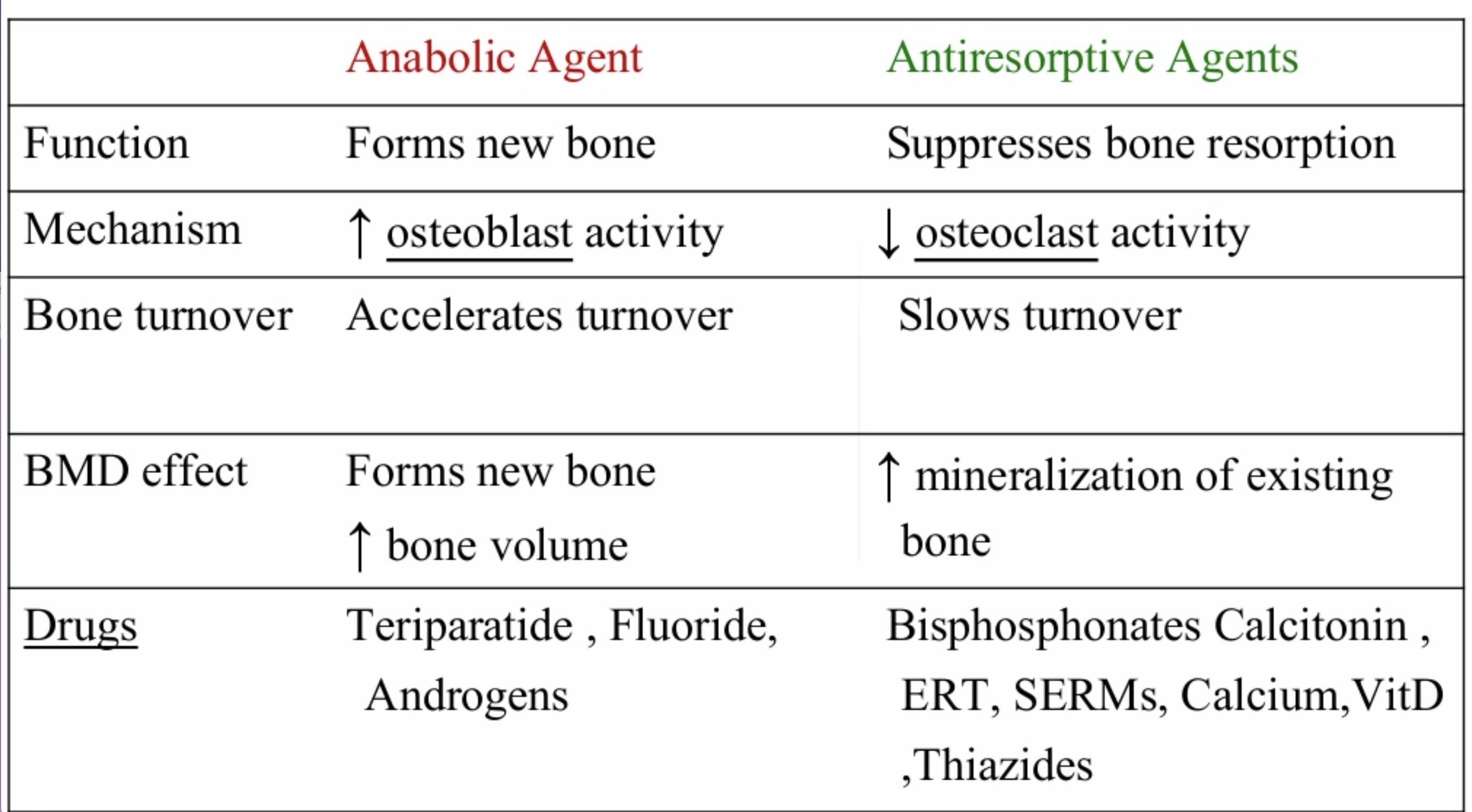
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
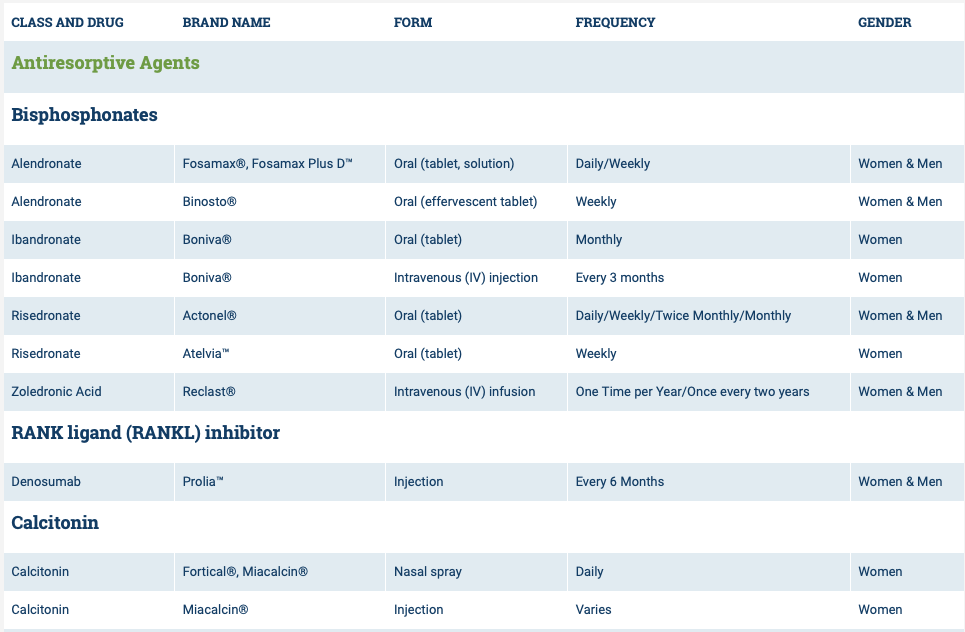
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

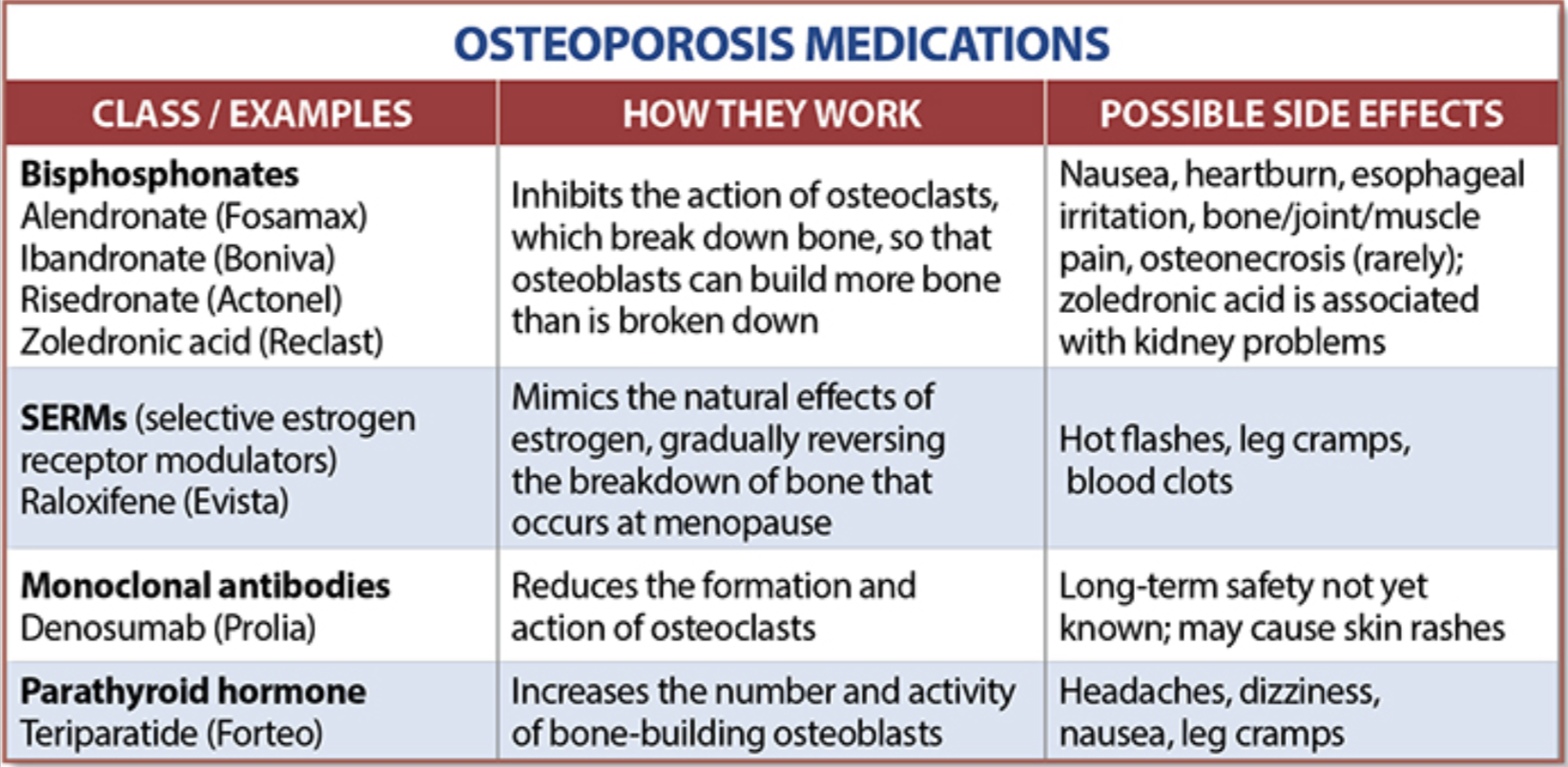
The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
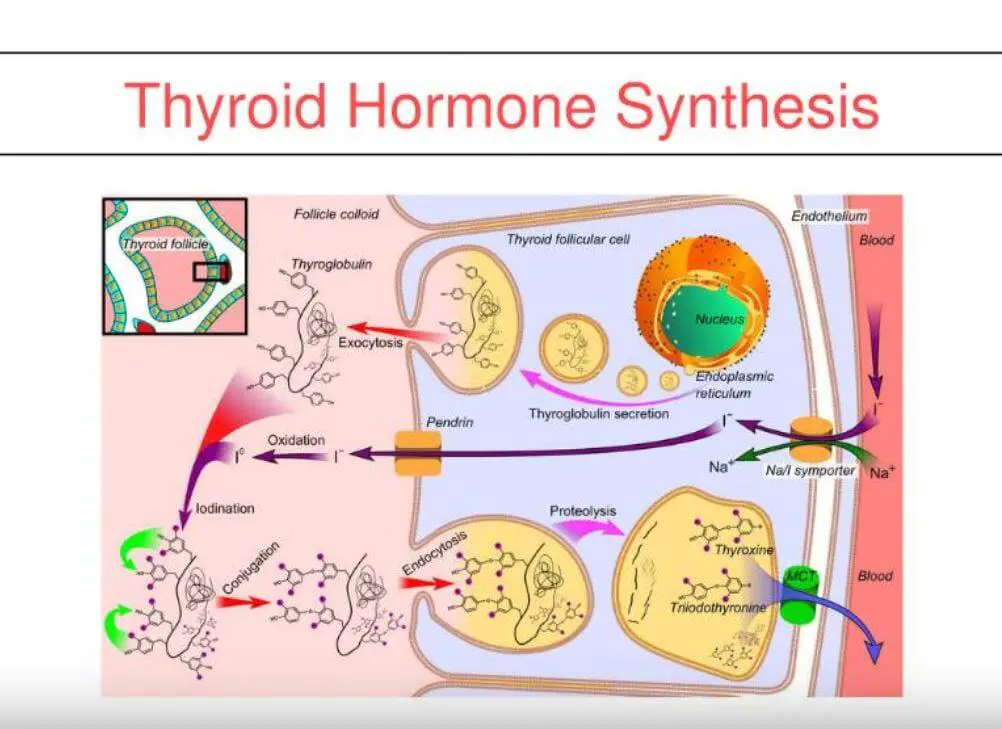
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
Vitamin K1 & K2, Interaction with Anticoagulant
May 11, 2019 6:00 am
During a recent group meeting, questions were raised regarding supplementing with Vitamin K1 or Vitamin K2 along with anticoagulant treatment. The table below provides a generalized summary of the Vitamin K1 and K2. The forms of Vitamin K in dietary supplements may differ depending on the supplement and the choice of the supplements may affect their absorptive behavior. This creates a challenge in regulating lab values, especially in patient who require anticoagulation therapy. 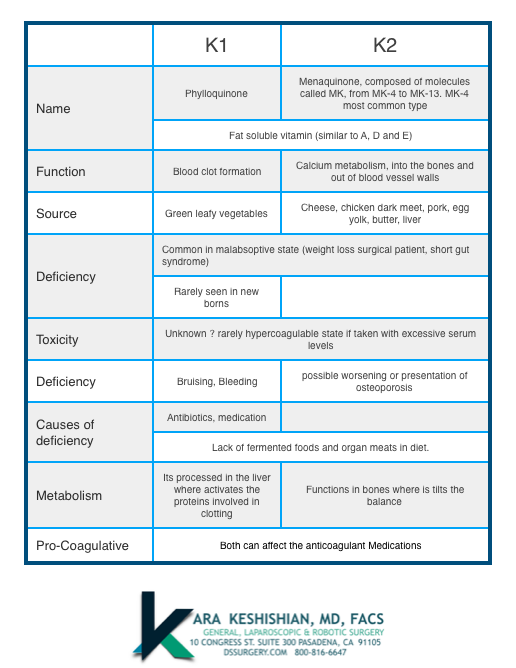
There is a lot of evidence that distinguishes between the vitamin K1 and K2 and their respective function with Cognition , Skeletal Muscle Energy Metabolism and the flexibility of the arterial wall.
In summary K1 and K2 counteract the function of the anticoagulant medications. You should consult the physician prescribing the anticoagulant before taking any vitamin K1 or K2. Even as we think of K2 having less to do with coagulation pathways, it is recommended that the patients do not take any vitamin K supplements unless cleared by their physician, since K2 may also affect the anticoagulation treatment. As a patient who is prescribed anticoagulation treatment you should make your prescribing physician aware of ANY changes in your medications or supplements either over the counter or prescribed.
Sleeve Gastrectomy Failure
May 07, 2019 12:53 pm
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
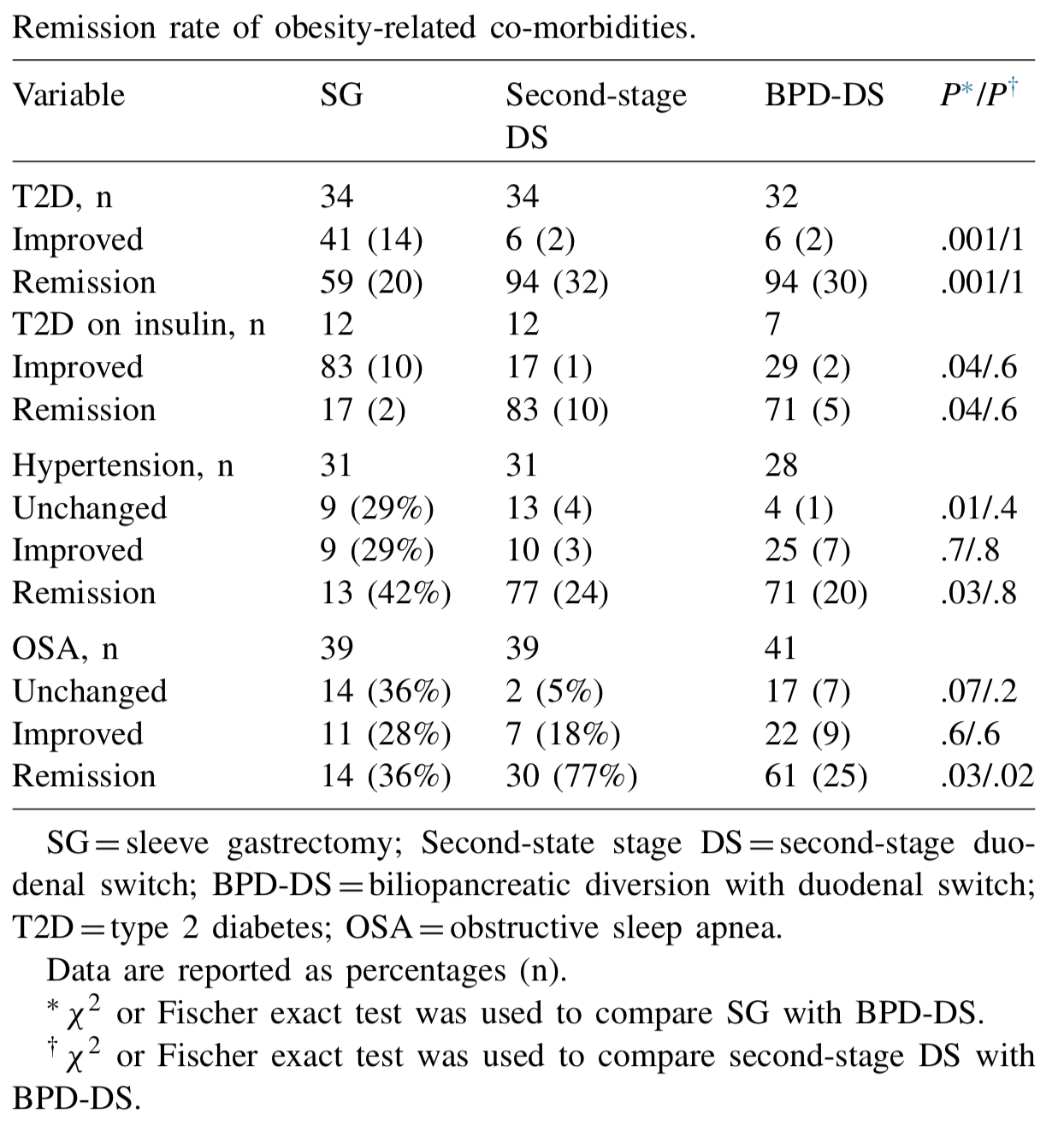
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss. 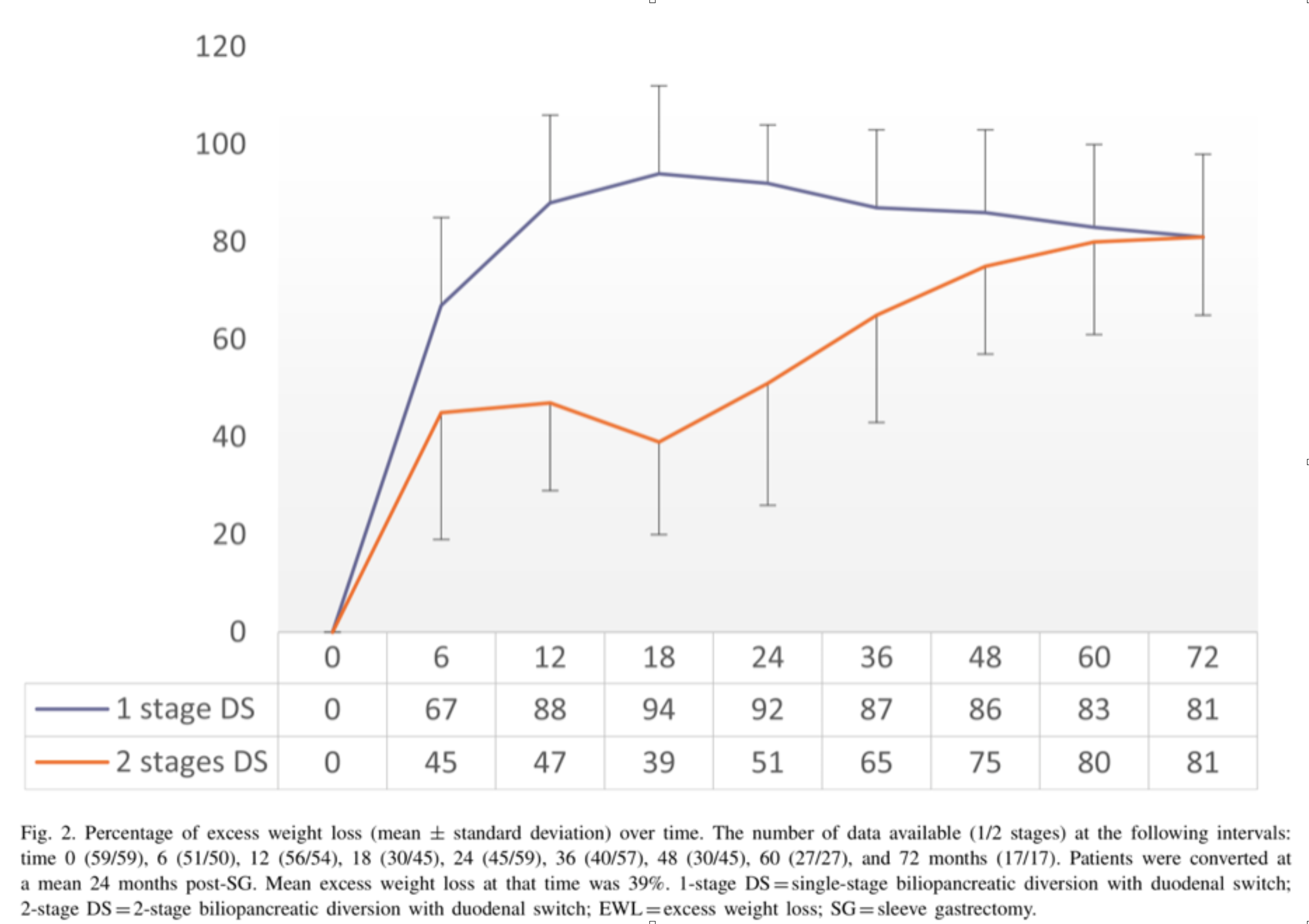
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.