Category: Uncategorized
Will Weight Loss Surgery Resolve All Common Co-Morbid Conditions?
August 28, 2020 1:07 pm

Covid-19 Mutation – Please physically distance and Wear Masks
August 18, 2020 1:16 pm
Introduction:
There is evidence emerging of Covid-19 mutation. This may explain the difference between the severity and intesity of the disease presented in the those geographical locations where the disease first.
Scientists from The Scripps Research Institute, Jupiter, Florida have identified changes in the Spike protein. This protein is used to bind the virus to host membranes. As we now know Florida is one of the few hot spots of the Covid-19 pandemic.
This has significant implications for the long term strategy needed to control transmission and manage resurrgence.
Until there is effective vaccination or effective treatment available for everyone, prevention by wearing face mask is the most efficient form to avoid transmistion.
Prevention:
The facts are that the most consistent effective preventive measures are wearing face masks and physical distancing.
There are those who may feel invincible and think that you will 1. either not get the disease or even if you get it it will 2-not affect your health. Lets first remind ourselves that wearing a mask is more to prevent passing the virus that getting it. We should all assume that someone that we come in contact with may already have it. Would you like them to breath the virus toward you ? This then brings the second issue: We do not know what the long term health effect of the virus is for those who develop significant symptoms and those who are asymtphomatic.
The unkown:
Let’s look at other viral infections that provide either no or minimal disease condition at the time of initial exposure only to result in long term health conditions that may result in death. These include hepatitis and HIV exposures and infections. Admitedly Coronavirus is a differnt family of virus. I am not suggesting that this will behave like other family of the viruses. We just do not have enough information to know what happens to those exposed to the virus (regardless of being asymptotic or not). Could the virus become dormant and over time result in organ injury (lung) like in the case of hepatitis (liver). Or make a home in our body and have recurrent debilitating infections and symptoms as it is seen with Varicella-zoster virus (VZV) which causes chickenpox and the time of the initial infection and makes residence in our body to reappear later on as herpes zoster (shingles). Will we need a new strain of vaccine every year similar to the flu vaccine?
That is the crux. We do not know because the COVID virus is new and we do not know the long term effects.
Vitamin D and COVID 19
June 13, 2020 4:40 pm
There has been extensive discussion on the importance of Vitamin D published over the last few years in regards to bone health, immune health and Calcium physiology. The importance of vitmain D and bone structure has been discussed extensively. It is also important in the absorption of Calcium. It further plays role in immune modulation.
What is new is the possible correlation of Vitamin D and COVID 19. Recently it is been shown that low vitamin D may increase the risk of a poor outcome with Covid-19 exposure and infection.
There are different standard recommendation for the Vitamin D levels.
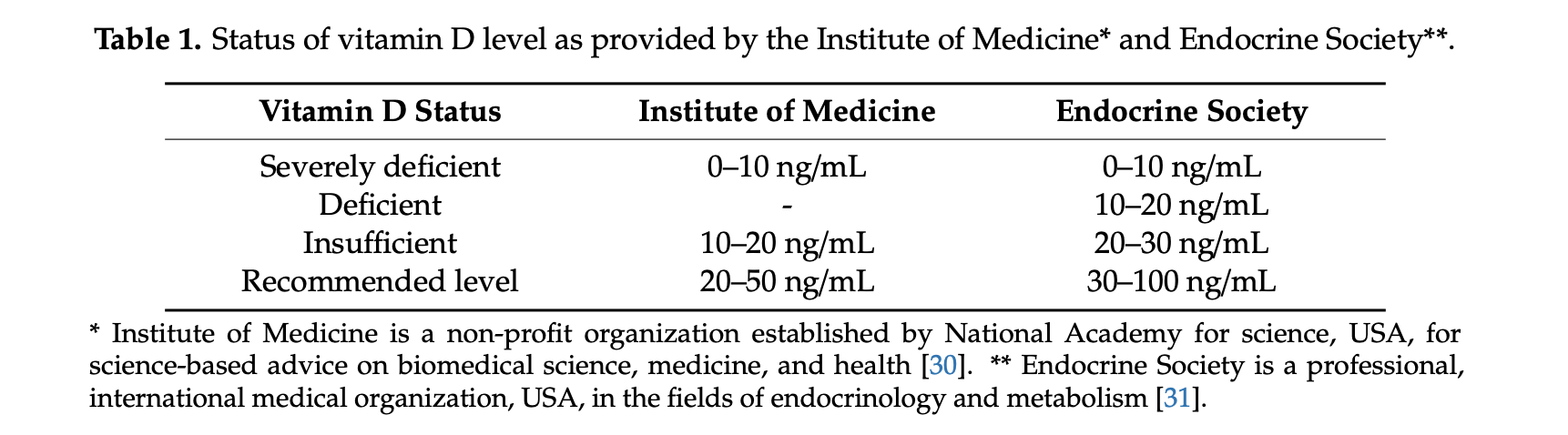
In our practice we aim to maintain a Vitamin D level of 0ver 60 in post weight loss surgical patients.
There are a number of theories as to how the Vitamin D deficiency may play a role in this. An emerging observation is that low Vitamin D may cause abnormal and excessive blood clot formation. Mohammad et. al. in 2019 published a study on the association of low vitamin D and “…Pathogenesis of Thrombosis”
This pathologic blood clot formation in COVID-19 patients may explain the extensive lung injury and multi system organ failure in some patient. It is also one of the reason that some COVID-19 patients have loss limbs or appendages.
Please follow all supplement recommendations based on your laboratory studies and all COVID-19 recommendations. We would recommend frequent hand washing, surface cleaning, social distancing, and wearing face masks as the most basic precautions and increase precautions based on your health status.
Vitamin D and Covid -19
May 07, 2020 9:24 am
We are all aware of the many roles that Vitamin D plays in our bodies. This includes immune function in addition to all the regulatory roles that Vitamin D plays in several physiologic reactions. There may be a correlation of low Vitamin D and COVID-19 infection increasing death risk as looked at in research articles.
Covid -19 in a subset of patience causes significant lung injury. These patients require mechanical ventilation.
Previously reported publications have suggested a possible correlation between ace inhibitors and increased risk of pulmonary complications of Covid -19. Some researchers suspect that the Covid-19 may be able to enter lung cells by the ACE receptors.
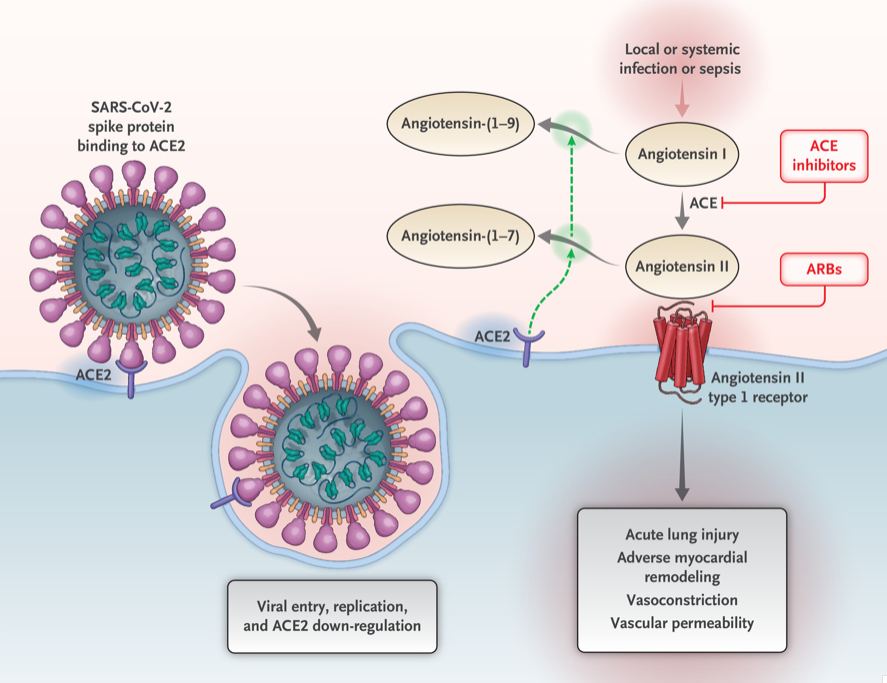
Vitamin D may positively implact the receptor ACE2. This study, report clear correlation between the high death rate with low vitamin D levels in Covid infected patients. There are limitation to this study that the attached abstract outlines.
Our take home message would be to please make sure you have updated labs and that you are all taking the recommended Vitamin D based on your surgical anatomy and laboratory values, not just an average non-bariatric person recommended dose.
https://www.dssurgery.com/wp-content/uploads/2020/05/manuscript.pdf
Why Oxygenation in Covid-19 is a major problem
April 21, 2020 7:27 am
Covid-19 is a respiratory virus. The majority of patient may experience no or minimal symptoms. But small subset of those infected will unfortunately progress to have significant pulmonary dysfunction. Some will even require mechanical ventilation. Oxygenation in COVID 19 patients with severe symptoms is altered. This is the due to the changes caused by the virus.
Normal Physiology
Oxygen (O2) is exchanged with Carbon Dioxide(CO2) in the lungs. The CO2 is exhaled and the O2 is taken up by the blood. This high O2 continuing blood is then pumped to every single organ. With complete distribution network of capillary vessels, every cell then gets access to the O2 rich blood. Hemoglobin is the carrier that transports the O2.
The O2 is removed and dissociated from the Hgb depends on a number of variables. Each red cell Hgb has four binding site for the oxygen. The affinity and strength of each one of those four units for oxygen changes based on a number variables. These are CO2, Acidity (PH), DPG and temperature.
Oxygen Dissociation Curve
The oxygen dissociation curve has a long “S” shape. On the low end of oxygen in the blood most of the Hgb site are occupied. As the oxygent level increase there is little change to the saturation.

Normally the relationship of the blood in the lungs (horizontal axis) and the amount of the O2 in the red cell (vertical axis) is following the red line. When the amout of oxygen insired is 25mmhg the blood saturation is at 50% (A). The blood saturation is nearly 100% when room air is inhaled (C). Room air has PO2 of 75mmHg. Note that there is very little change in blood saturation (SaO2) by increasing the PO2 from 75 to 100 mmHg (the red line is horizontal between 75-100).
{kind=link}
Another way to look at this: If you increase the PO2 from 25 to 50 (doubling) the Saturation goes from 50 (A) to nearly 85(B). Whereas increaseing the PO2 from 50 to 100 (doubling) only mober the Saturation from 85(B) to 100(C). This shows the efficiancy of system to be able to deliver the most amout of oxygen to the tissue even with the low level of oxygen present in the lungs.
As the Green and the Blue lines demosntrate the balance can change by changes in CO2, Acidity (PH), DPG and temperature.
COVID-19
When it comes to COVID-19 illness there may be a number of factors in play. Most patients with pre-existing conditions already have changes that may shift the curve to the right (high fever and high Co2). Furthermore, obesity, asthma and other conditions may decrease the ability to clear the lungs of secretions and mucus may contribute to decreased oxygenation. Additionally, there is significant inflammation associated with the chemicals released in COVID-19 (cytokines). These can cause devastating changes to the ability to exchange oxygen in the lungs.
Oxygenation in COVID-19 severely symptomatic patient can deprive oxygen from organ. This can progress to organ failure. One of the most common organ systems to fail is the kidneys which may require dialysis.
Covid-19 Pandemic and Obesity
April 12, 2020 7:44 pm
We have now seen several articles with data collection regarding patients with obesity and COVID-19 being at greater risk of hospitalization. We can look at metabolic syndrome associated with obesity as a risk factor also.
We have all been in physical isolation due to Covid-19 pandemic. The strategy of minimizing contact has worked. The data is clear when comparing information from states that instituted an aggressive containment plans compared to those who have not. This shows a sigifnicat flattening of the curve in California for example.
The CDC publishes the Morbidity and Mortality Weekle Report (MMWR) . The latest publushed summary (as of date of publucation of this blog) provides an insight to the risk factors of hospitalization.
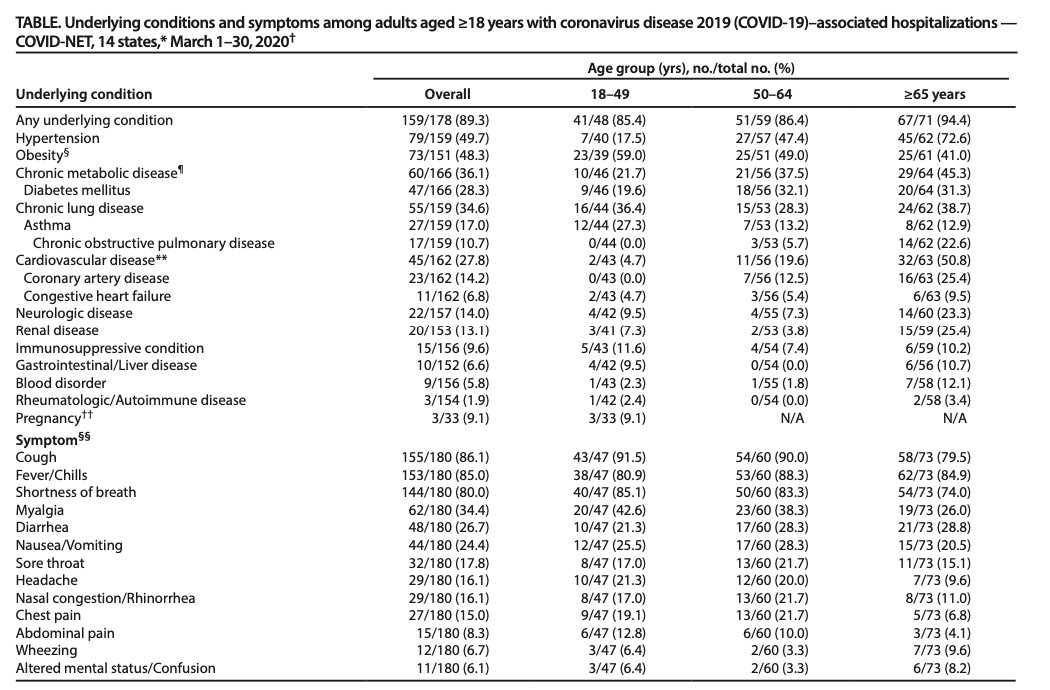
Concerning to see that a respiratory virus is more likely to hospitalize those with Obesity, Diabetes and hypertension at a higher rate than lung and pulmonary related conditions.
Let us recognize that this is only a summary collected data. Therefore, there are limitatation to making any assumption of conclusion based on this information.
With those limitation aknowldged, and relying on our obesity related comobidities, we can make a few conclusions:
Not surprising, Obesity as with other diseases, compounds Covid-19 exposure and infection. Diabates is also a risk factor. There are no indepth information available on the diabetic patients. There is now data showing superior outcome of diabetes resoultion with weight loss surgery compared ro medical treatment.
Vitamin D Metabolism and Deficiency file
March 28, 2020 8:17 am
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
In some cases, patients may need injectable Vitamin A or D to improve vitamin levels.
Click the links to view the information below and within the comments of this file:
Vitamin D3 50 by Biotech: Amazon
directly from BioTech:
Many DS surgeon’s do not recommend Children’s vitamins or chewable vitamins unless there is a specific reason or need for them.
DS Surgeon Blog on Vitamin D:
Webinar on Vitamin D metabolism:
Medications that effect Bone health:
This does not constitute medical advice, diagnosis or prescribing. It is simply a compiled list of gathered information. If you are in doubt or have questions please contact your medical healthcare professional.
Articles
March 22, 2020 6:57 pm
Coronavirus – Protect Yourself And Those Around You
March 15, 2020 6:19 pm
Stapled Anastomosis
December 30, 2019 11:23 am
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
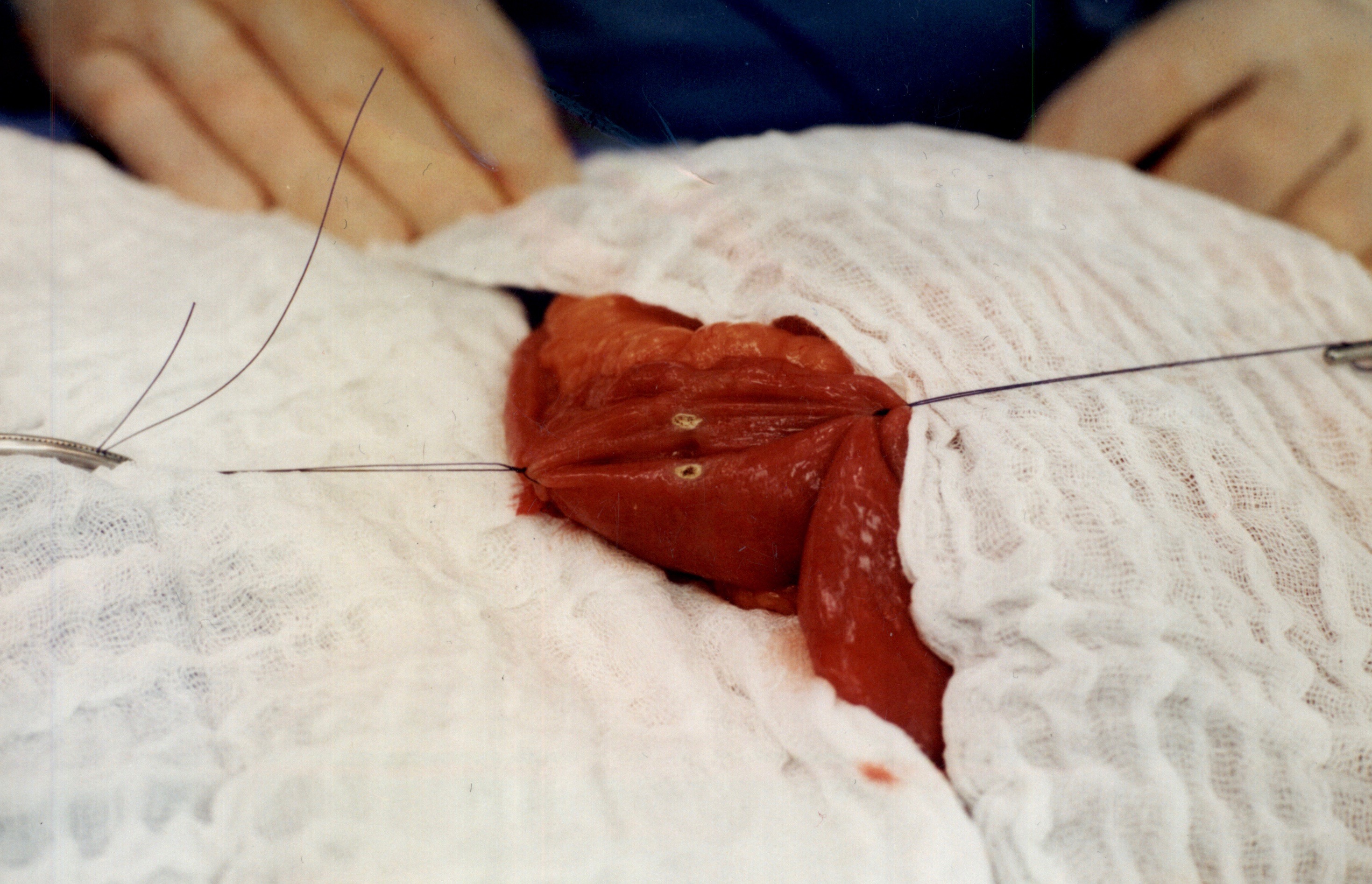
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
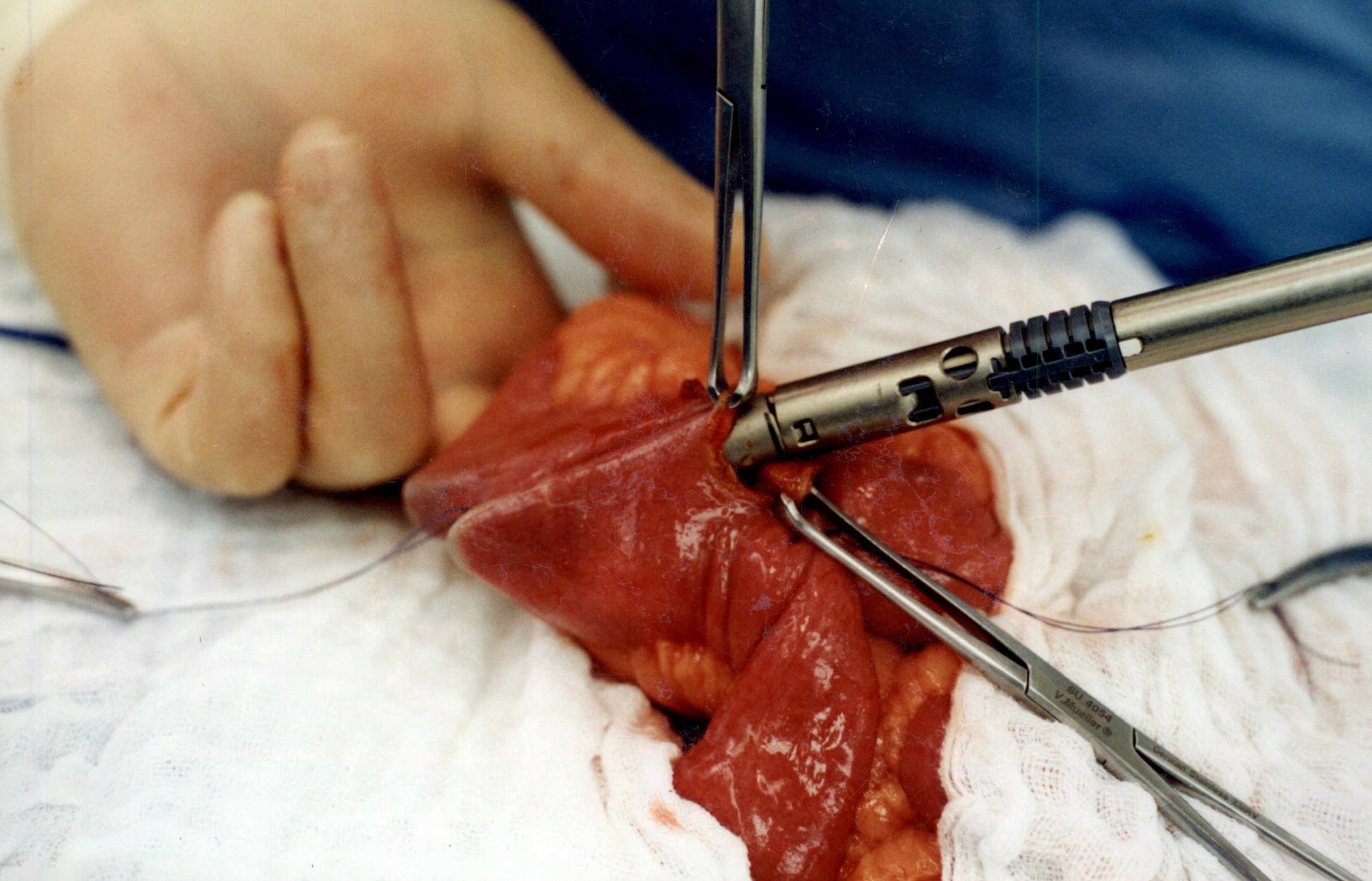
When the stapler is fired in opposite direction, a very wide anastomosis is created.
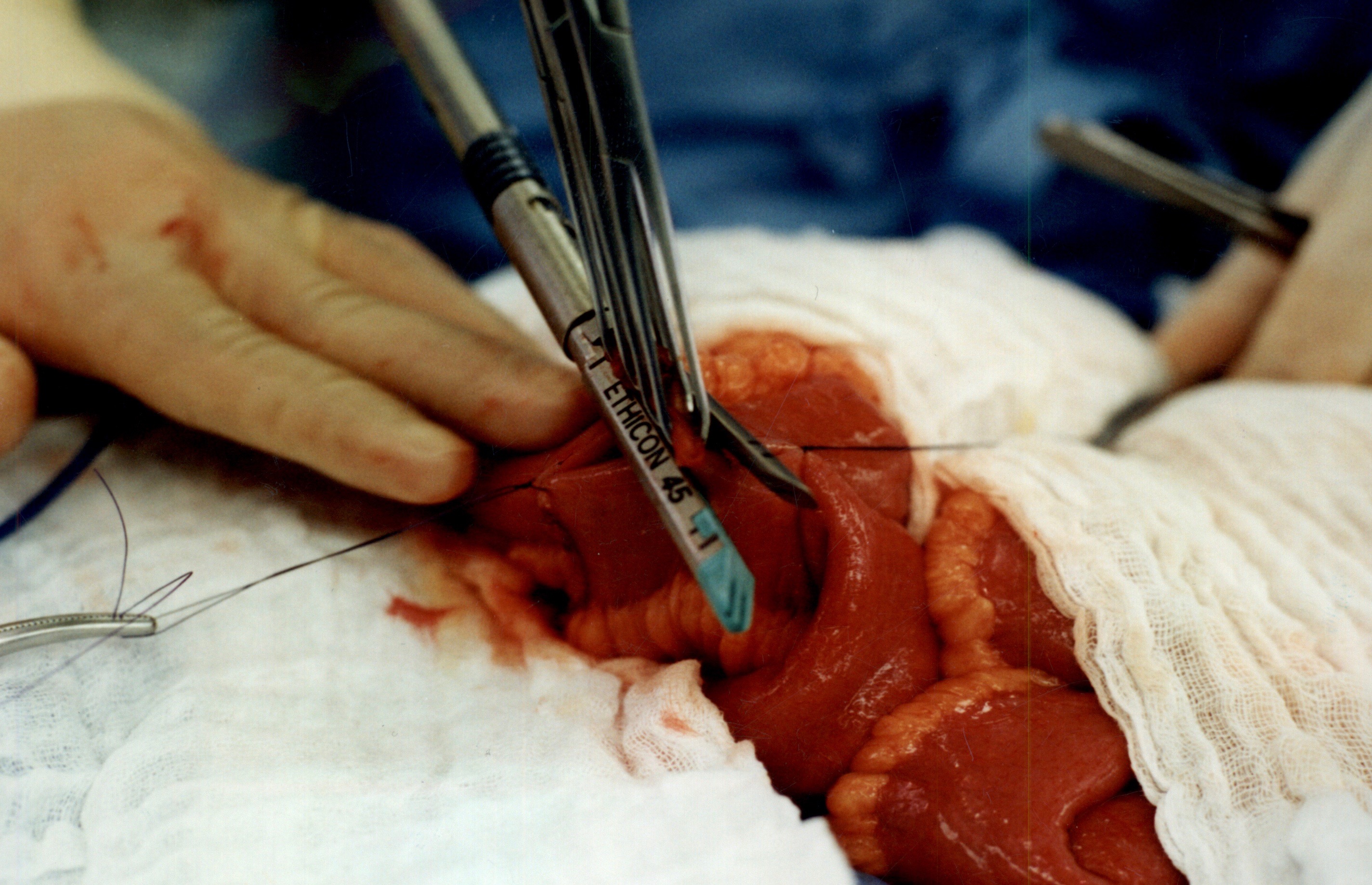
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.